
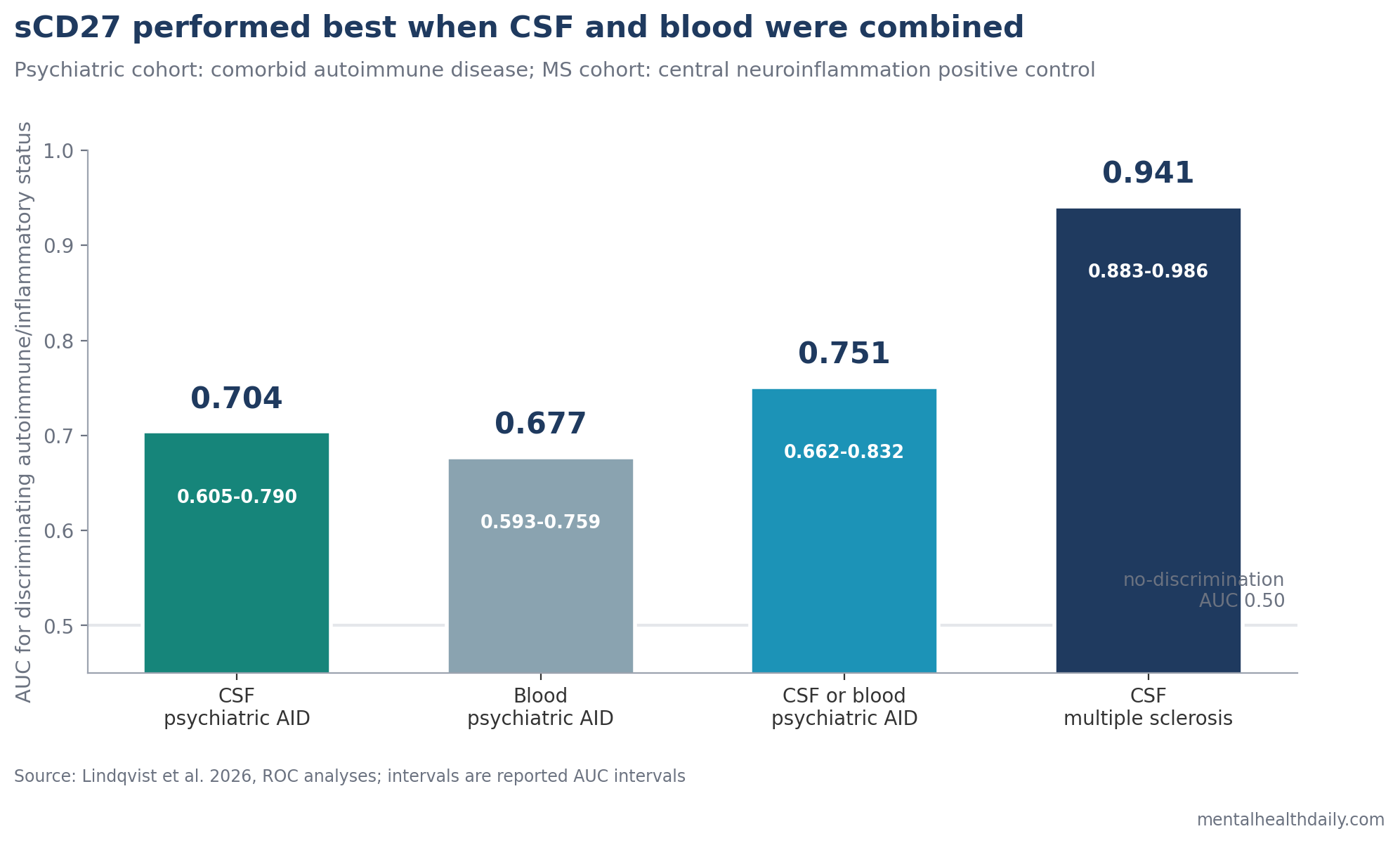
A 2026 immunopsychiatry cohort study found that soluble CD27 (sCD27), a marker of T-cell activation, was positive in cerebrospinal fluid in 23% of severe psychiatric patients selected for suspected immune involvement and in 88% of multiple sclerosis patients used as a positive-control group. In the psychiatric cohort, combined cerebrospinal fluid or blood sCD27 positivity was associated with comorbid autoimmune disease and produced the strongest autoimmune-disease discrimination in that cohort, with AUC 0.751.1
Research Highlights
- CSF positivity was common in the enriched psychiatric cohort: 26 of 115 patients with severe psychiatric disorders were CSF-sCD27+, compared with 30 of 34 multiple sclerosis patients and 3 of 122 controls.1
- Blood alone was weaker than CSF plus blood: blood-sCD27+ identified 17 of 114 psychiatric patients, but blood positivity alone was not significantly associated with autoimmune disease.
- Autoimmune disease tracked the combined marker: CSF and/or blood sCD27 positivity was more likely in patients with comorbid autoimmune disease (X² = 8.56, p = 0.003) and had AUC 0.751 for autoimmune vs. non-autoimmune classification.
- CSF pathology supported the signal: sCD27 positivity was associated with elevated CSF total tau, neurofilament light, pleocytosis, and any abnormal CSF marker (X² = 8.72, p = 0.003).
- The clinical use is triage, not diagnosis: the study was a preprint in a selected high-risk cohort, so sCD27 should be read as a candidate immune-workup marker for complex cases rather than a screening test for ordinary psychiatric symptoms.
Soluble CD27 is a shed form of CD27, a receptor found on T lymphocytes and memory B cells. When adaptive immune cells are activated, CD27 can be released into fluid compartments; elevated sCD27 in cerebrospinal fluid (CSF; the fluid around the brain and spinal cord) is therefore used as a marker of intrathecal immune activation, meaning immune activity inside the central nervous system compartment.
The psychiatry question is narrower than “is mental illness autoimmune?” The useful question is whether a measurable immune marker can help identify a subgroup of severe psychiatric patients whose symptoms sit near autoimmune disease, neuroinflammation, or central nervous system immune activity.
115 Severe Psychiatric Cases Were Compared With MS and Surgical Controls
Lindqvist et al. measured sCD27 in the Immunopsychiatry cohort at Uppsala University Hospital.1 These were not general outpatient psychiatric patients. The cohort included 115 people with severe psychiatric disorders and clinical signs suggesting possible immunological involvement.
The design used 2 comparison groups:
- Surgical controls: 154 age-matched people undergoing surgery, with 122 usable CSF samples and 154 blood samples after exclusions.
- Multiple sclerosis controls: 37 people with multiple sclerosis (MS), an inflammatory demyelinating disease of the central nervous system, used as a positive-control group for central neuroinflammation.
The psychiatric cohort was diagnostically mixed. Psychosis was recorded in 63 of 115 patients, obsessive-compulsive disorder (OCD) in 48, neurodevelopmental disorders in 37, catatonia in 10, and anxiety or affective symptoms in 80. Many patients had more than 1 psychiatric syndrome, so the biomarker was tested against immune and CSF pathology rather than against a single Diagnostic and Statistical Manual category.
Positive sCD27 was defined conservatively: above the 97.5th percentile of age-stratified controls in CSF or blood. That choice makes the result less vulnerable to calling ordinary variation “positive,” but it also means sensitivity can be modest.
CSF-sCD27 Was Positive in 23% of Psychiatric Patients and 88% of MS Patients
CSF-sCD27 was elevated in 26 of 115 psychiatric patients, or 23%. Blood-sCD27 was elevated in 17 of 114, or 15%. In the MS positive-control group, 30 of 34 patients with CSF data were CSF-sCD27+, while 8 of 37 were blood-sCD27+.
Median CSF-sCD27 also separated the groups:
- Controls: 136 pg/mL, range 25-528.
- Psychiatric cohort: 184 pg/mL, range 25-3797.
- MS cohort: 742 pg/mL, range 101-2447.
The MS pattern anchors what the assay is supposed to detect: T-cell-mediated central nervous system inflammation.
Feresiadou et al. measured CSF-sCD27 in 803 people and found that sCD27 above 250 pg/mL carried a likelihood ratio of 10 for inflammatory neurologic disease.4 Van der Vuurst de Vries et al. later found that higher CSF-sCD27 after clinically isolated syndrome predicted later MS diagnosis and a 5.5-fold higher annualized relapse rate.5
The psychiatric result therefore does not stand alone. It extends an existing neuroinflammation marker into a selected psychiatric population where autoimmune comorbidity and CSF abnormalities were already clinically suspected.
Autoimmune Disease Was More Common When CSF or Blood sCD27 Was Positive
Comorbid autoimmune disease was identified in 43 psychiatric patients after specialist review. Those diagnoses included systemic lupus erythematosus, autoimmune thyroiditis, inflammatory bowel disease, type 1 diabetes, antiphospholipid syndrome, celiac disease, rheumatoid arthritis, multiple sclerosis, psoriasis, anterior uveitis, Kawasaki disease, and polymyalgia rheumatica.
Among patients with autoimmune disease, 21 of 43 were sCD27+ in CSF and/or blood. The association between combined positivity and autoimmune disease was statistically significant (X² = 8.56, p = 0.003). CSF positivity alone was also associated with autoimmune disease (X² = 4.85, p = 0.028), while blood positivity alone was not (X² = 1.35, p = 0.245).
Disease activity signal: CSF-sCD27+ was associated with moderate or severe autoimmune disease activity compared with subclinical or mild activity (OR = 5.14, p = 0.029). Combined CSF and/or blood positivity produced a similar activity signal (OR = 4.81, p = 0.038). Blood values alone again failed to carry the result.
Compartment signal: several patients had high CSF-sCD27 without blood positivity, including all 4 psychiatric-cohort patients with pleocytosis, meaning elevated white blood cells in CSF. That pattern argues against treating blood and CSF as interchangeable. Blood may help when peripheral autoimmune activity is relevant, but CSF appears necessary when the question is central nervous system immune activation.
CSF Abnormalities Strengthened the Neuroinflammation Interpretation
sCD27 positivity was not tied to a single psychiatric diagnosis. Univariate analyses did not show a specific disorder category, such as psychosis, OCD, neurodevelopmental disorder, catatonia, or anxiety/affective symptoms, as the main driver.
The stronger pattern was biological:
- Total tau: 11 of 15 patients with elevated CSF total tau were sCD27+, X² = 4.78, p = 0.03.
- Neurofilament light: 11 of 14 patients with elevated CSF neurofilament light were sCD27+, X² = 6.27, p = 0.01.
- Pleocytosis: 4 of 4 patients with elevated CSF cells were CSF-sCD27+, p = 0.008.
- Any abnormal CSF marker: 21 of 41 patients with an abnormal CSF marker were sCD27+, X² = 8.72, p = 0.003.
Neurofilament light is a marker of axonal injury, while total tau can rise with neuronal injury or neurodegenerative stress. These markers do not prove an autoimmune psychiatric disease by themselves, but their association with sCD27 makes the T-cell activation signal more biologically coherent.
The study also found 15 sCD27+ psychiatric patients without a known autoimmune diagnosis. That subgroup is the most clinically provocative and the most uncertain. It could include patients with undiagnosed autoimmune disease, patients with immune activity that does not fit current diagnostic categories, or false-positive biomarker findings in a complex cohort.
Autoimmune Psychiatry Needs Red-Flag Triage, Not Mass Screening
Marrie et al. found that psychiatric diagnoses can rise before later immune-mediated inflammatory disease diagnosis.2 Pollak et al. later proposed a consensus approach to suspected autoimmune psychosis, emphasizing red flags, neurologic features, CSF testing, electroencephalography, magnetic resonance imaging, and immune evaluation rather than diagnosis from psychiatric symptoms alone.3
Lindqvist et al. fit that clinical lane. The study does not say that schizophrenia, OCD, affective symptoms, or catatonia are usually autoimmune. It says that in a severe, selected psychiatric population, an adaptive-immune activation marker tracked autoimmune comorbidity and CSF pathology.
Clinically, sCD27 would make the most sense when several features converge:
- Severe or atypical psychiatric presentation: abrupt onset, marked fluctuation, confusion, catatonia, new cognitive dysfunction, seizures, or neurologic signs.
- Autoimmune context: personal autoimmune disease, multiple autoimmune diagnoses, strong family history, or inflammatory systemic symptoms.
- Objective abnormalities: CSF pleocytosis, oligoclonal bands, elevated IgG index, elevated neurofilament light, elevated total tau, abnormal MRI, or abnormal EEG.
- Treatment implication: a plausible question about immunology referral, diagnostic escalation, or immune-directed treatment inside a specialist framework.
Without those features, sCD27 testing risks becoming another nonspecific lab value attached to a broad psychiatric label. The marker is most useful as part of an immune-neurology workup, not as a standalone mental-health test.
Limitations of This sCD27 Psychiatric Biomarker Study
The paper is a preprint. It has not completed peer review, and the authors explicitly note that it should not guide clinical practice by itself.
The cohort was enriched for immune suspicion. A 23% CSF-sCD27 positivity rate should not be projected onto ordinary psychiatric populations. The base rate would probably be lower in routine depression, anxiety, OCD, ADHD, or psychosis clinics.
AUC was moderate for autoimmune disease. Combined CSF or blood positivity reached AUC 0.751, which is useful for research triage but not enough for diagnosis. AUC can also look cleaner than real clinical decision-making when the predictor is binary and the population is selected.
Blood was not enough. Blood-sCD27 positivity alone did not significantly identify autoimmune disease in the psychiatric cohort. Any future clinical pathway would need to justify when invasive CSF sampling is worth the added information.
No peripheral autoimmune control group was included. The study compared psychiatric patients, MS patients, and surgical controls. A group with active systemic autoimmune disease but no severe psychiatric presentation would help separate psychiatric-specific signals from broader autoimmune activity.
Questions About sCD27 and Autoimmune Psychiatry
Is sCD27 a diagnostic test for autoimmune psychiatric disease?
No. It is a candidate biomarker of T-cell activation that may help triage selected complex cases. It does not diagnose autoimmune psychosis, autoimmune OCD, schizophrenia, depression, or any other psychiatric syndrome by itself.
Why does CSF matter more than blood here?
CSF is closer to central nervous system immune activity. In this study, several patients had CSF positivity without blood positivity, and blood alone did not significantly identify autoimmune disease.
What does a positive result suggest?
In the right clinical context, a positive result may support further evaluation for autoimmune disease, neuroinflammation, or central nervous system immune activation. It should be interpreted with symptoms, neurologic exam, CSF markers, imaging, EEG, infection evaluation, and autoimmune history.
Should psychiatric patients ask for sCD27 testing?
Routine testing is not supported. The evidence is most relevant to severe, atypical, or treatment-resistant cases with autoimmune red flags or objective neurologic/CSF abnormalities.
References
- Lindqvist I, Tigchelaar C, Rasmusson AJ, et al. Soluble CD27 as an indicator of autoimmune disease in severe psychiatric disorders. medRxiv. 2026. doi:10.64898/2026.04.16.26351038
- Marrie RA, Walld R, Bolton JM, Sareen J, Walker JR, Patten SB, et al. Rising incidence of psychiatric disorders before diagnosis of immune-mediated inflammatory disease. Epidemiology and Psychiatric Sciences. 2019;28(3):333-342. doi:10.1017/S2045796017000579
- Pollak TA, Lennox BR, Müller S, Benros ME, Prüss H, Tebartz van Elst L, et al. Autoimmune psychosis: an international consensus on an approach to the diagnosis and management of psychosis of suspected autoimmune origin. Lancet Psychiatry. 2020;7(1):93-108. doi:10.1016/S2215-0366(19)30290-1
- Feresiadou A, Nilsson K, Ingelsson M, Press R, Kmezic I, Nygren I, et al. Measurement of sCD27 in the cerebrospinal fluid identifies patients with neuroinflammatory disease. Journal of Neuroimmunology. 2019;332:31-36. doi:10.1016/j.jneuroim.2019.03.015
- van der Vuurst de Vries RM, Mescheriakova JY, Runia TF, Jafari N, Siepman TAM, Hintzen RQ. Soluble CD27 levels in cerebrospinal fluid as a prognostic biomarker in clinically isolated syndrome. JAMA Neurology. 2017;74(3):286-292. doi:10.1001/jamaneurol.2016.4997