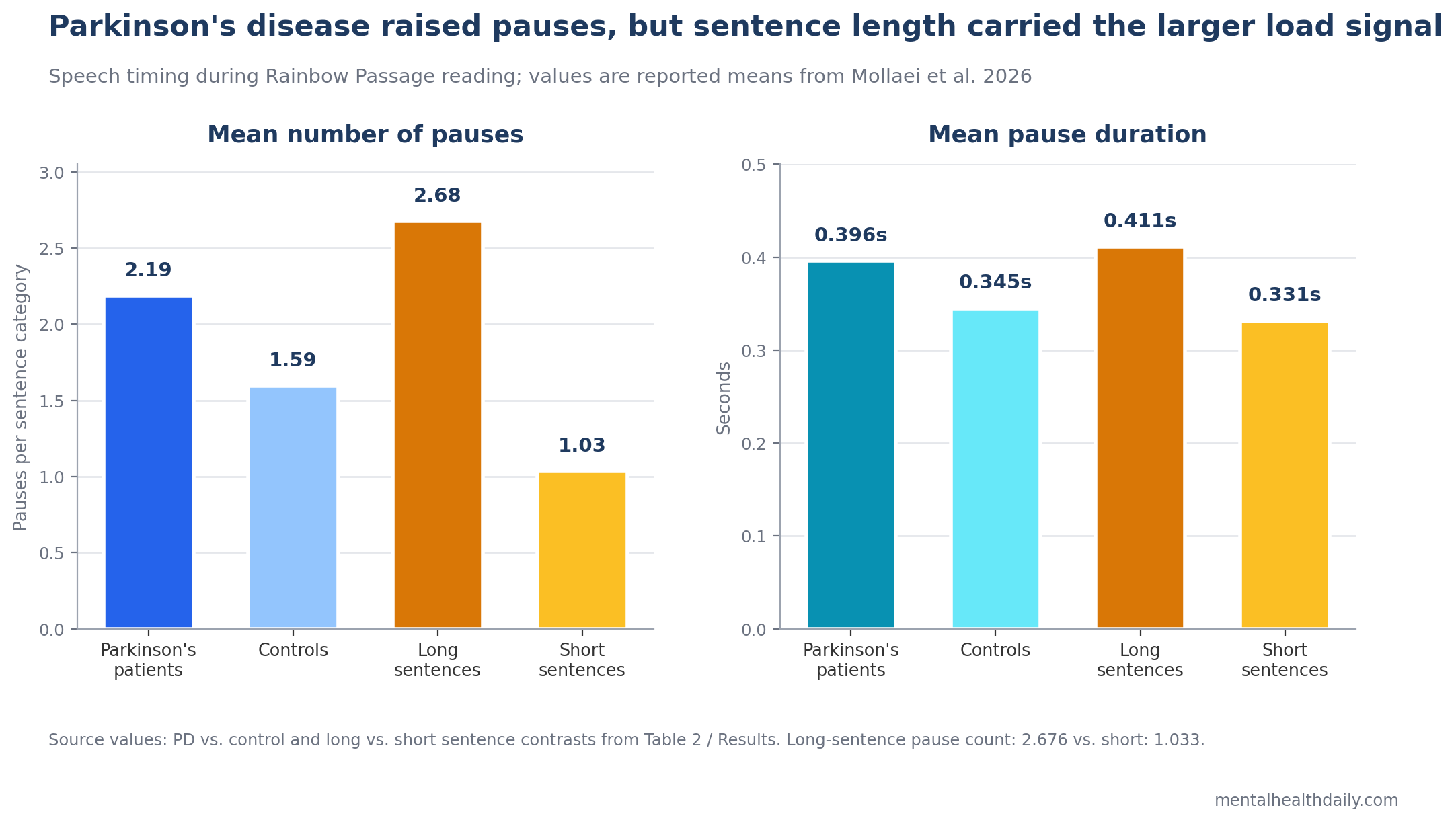
A 2026 connected-speech study found that people with Parkinson’s disease produced more silent pauses than older controls while reading aloud: 2.185 vs. 1.595 mean pauses, while long sentences produced 2.676 pauses vs. 1.033 in short sentences.1 Within the Parkinson’s group, MoCA scores correlated with total pause count (rs = −0.502, p = 0.005).
Research Highlights
- Parkinson’s speech included more pauses: a 71-person study found higher mean pause counts in Parkinson’s disease than controls during passage reading, 2.185 vs. 1.595 pauses, F(1,66) = 11.905, p < .001.1
- Sentence length carried the biggest load signal: long sentences produced 2.676 mean pauses vs. 1.033 in short sentences, and pause duration rose from 0.331 to 0.411 seconds.
- Complex syntax raised pause frequency: complex sentences produced 2.224 mean pauses vs. 1.118 in simple sentences, with a disease-by-complexity interaction for pause number (p = .012).
- Cognition tracked pause count, not pause duration: MoCA scores correlated with total pauses in Parkinson’s disease (rs = −0.502, p = 0.005) but not with pause duration measures.
- Dysarthria tracked pause length: speech-motor severity correlated with pause duration in short, long, and complex sentences, including rs = 0.509 for complex sentences.
Hypokinetic dysarthria is the motor-speech pattern commonly associated with Parkinson’s disease, usually involving reduced loudness, reduced pitch variation, imprecise articulation, and disrupted rhythm. Silent pauses are intervals of no speech; in this study, pauses longer than 200 milliseconds were counted because that threshold is long enough to suggest planning, timing, breathing, or speech-motor disruption rather than ordinary articulation gaps.
Pause timing works best as a mechanism-sensitive fluency measure. Basal-ganglia motor timing, respiratory-speech coordination, sentence planning, cognitive load, and the structure of the speech task can all move the numbers.
32 Parkinson’s Patients and 39 Controls Read the Rainbow Passage
Mollaei et al. analyzed speech recordings from 32 adults with idiopathic Parkinson’s disease and 39 older neurotypical controls.1 The Parkinson’s group had a mean age of 67.59 years, mean disease duration of 73.41 months from diagnosis, mean MoCA score of 26.69, and mean dysarthria severity rating of 55 on the study team’s perceptual scale.
Participants read the 327-word Rainbow Passage aloud. The researchers coded silent pauses in Praat, manually checked boundaries with 2 raters, and reported reliability coefficients of 0.93 for pause number and 0.86 for pause duration.
The passage was divided by sentence features:
- Short sentences: 11 sentences, 7-17 words, mean 11.82 words.
- Long sentences: 8 sentences, 21-28 words, mean 23.75 words.
- Simple vs. complex syntax: sentence categories based on prior Rainbow Passage coding criteria.
- Pause locations: within-sentence pauses and between-sentence pauses.
All Parkinson’s participants withheld medication for at least 12 hours before testing. That design reduces medication-state noise, but it also means the sample probably leaned toward people with mild-to-moderate disease who could tolerate withdrawal.
Parkinson’s Increased Pause Number, but Sentence Load Was Larger
Disease status mattered. Parkinson’s participants produced more pauses than controls in the sentence-length analysis, with mean pause count 2.185 vs. 1.595, F(1,66) = 11.905, p < .001. In the sentence-complexity analysis, the same disease effect appeared: 1.938 vs. 1.404 pauses, F(1,66) = 12.123, p < .001.
Sentence load was numerically larger than the group gap. Across groups, long sentences produced 2.676 pauses vs. 1.033 in short sentences, F(1,66) = 327.827, p < .001. Complex sentences produced 2.224 pauses vs. 1.118 in simple sentences, F(1,66) = 231.502, p < .001.
Interpretation: Parkinson’s disease shifted pause counts upward, but the act of reading a longer or syntactically more demanding sentence created an even stronger pressure to pause. That makes pause frequency a task-sensitive fluency marker, not a pure disease marker.
Long Sentences Lengthened Pauses More Than Simple Group Labels Did
Pause duration showed a smaller but still meaningful group effect. Parkinson’s participants had longer pauses than controls, 0.396 vs. 0.345 seconds, F(1,66) = 6.935, p = .011. The sentence-complexity analysis produced a similar disease effect, 0.408 vs. 0.353 seconds, F(1,66) = 9.456, p = .003.
Sentence length again changed the signal. Long sentences produced longer pauses than short sentences, 0.411 vs. 0.331 seconds, F(1,66) = 67.873, p < .001, with a disease-by-length interaction (p = .043). Complex sentences also produced longer pauses than simple sentences, 0.395 vs. 0.365 seconds, F(1,66) = 15.637, p < .001, but the disease-by-complexity interaction for duration was not significant.
Clinical implication: a patient who pauses more during long or syntactically complex sentences may be showing a combined speech-motor and planning burden. The same patient could look less impaired during short phrases, automatic speech, or rehearsed sentences.
MoCA Scores Tracked Pause Count in Parkinson’s Disease
Montreal Cognitive Assessment (MoCA) is a brief cognitive screen that samples attention, executive function, memory, language, visuospatial ability, and orientation. In the Parkinson’s group, lower MoCA scores were associated with more pauses:
- Total pauses: rs = −0.502, p = 0.005.
- Complex sentences: rs = −0.492, p = 0.006.
- Long sentences: rs = −0.477, p = 0.008.
- Short sentences: rs = −0.437, p = 0.016.
- Simple sentences: rs = −0.436, p = 0.016.
MoCA did not significantly correlate with pause duration. That split is useful: cognitive status appeared to relate more to how often speech flow was interrupted than to how long each interruption lasted.
Andrade et al. reported a related pattern in Parkinson’s disease: pausing before verb production was associated with mild cognitive impairment.4 Lee et al. also linked pauses during story retell to language planning in aging and Parkinson’s disease.3 Mollaei et al. extended that logic into a controlled reading task where the words were supplied, but sentence-level planning and speech-breath coordination still had to be managed.
Dysarthria Severity Tracked Pause Duration, Especially in Complex Sentences
Speech-motor severity pointed to a different part of the pause signal. Dysarthria severity correlated with pause duration in:
- Complex sentences: rs = 0.509, p = 0.004.
- Long sentences: rs = 0.428, p = 0.018.
- Short sentences: rs = 0.420, p = 0.021.
- Simple sentences: rs = 0.359, p = 0.052, a borderline result.
Dysarthria severity did not significantly correlate with pause number. A practical interpretation is that cognitive-linguistic load may increase interruption frequency, while speech-motor severity may stretch the duration of pauses once the flow is interrupted.
Huber et al. previously showed that Parkinson’s disease can change the relationship among breath pausing, syntax, and punctuation.2 Lowit et al. found that rhythmic performance in hypokinetic dysarthria varied across reading, spontaneous speech, and rapid syllable tasks.5 Those adjacent findings make the Mollaei result less surprising: pause timing moves with language structure, breathing, task demands, and motor-speech impairment.
Pause Timing Is a Therapy Target, Not a Standalone Diagnostic Test
Speech-language therapy for Parkinson’s disease often targets loudness, respiratory support, rate control, and intelligibility. Pause metrics could sharpen that work when they identify where fluency breaks down.
The most useful assessment would not ask only “how many pauses?” It would separate several questions:
- Task load: do pauses emerge mainly in long or complex sentences, spontaneous speech, story retell, or all speaking contexts?
- Cognitive load: do pause counts rise alongside lower MoCA scores, executive dysfunction, word-finding difficulty, or dual-task demands?
- Motor severity: do pause durations lengthen with perceptual dysarthria, reduced loudness, impaired articulation, respiratory control problems, or delayed initiation?
- Treatment response: do pause patterns improve after loudness training, rate modification, cueing, respiratory work, or cognitive-linguistic strategy training?
Interpretation guardrail: a long pause in Parkinson’s speech can reflect planning time, respiratory reset, sentence boundary marking, motor initiation difficulty, fatigue, microphone context, or a speaker’s deliberate pacing strategy. The measurement becomes clinically useful only when the task and mechanism are named.
Limitations of This Parkinson’s Speech-Pause Study
The design was cross-sectional. The study cannot show whether pause timing predicts later cognitive decline, dysarthria progression, falls, communication disability, or therapy response.
The Rainbow Passage mixed length and complexity. Long sentences and complex sentences overlapped, and the passage was not built to independently manipulate syntax and length. The main pattern is credible, but the separate effects of length and complexity are not perfectly isolated.
Motor staging was incomplete. The study did not collect Movement Disorder Society-Unified Parkinson’s Disease Rating Scale or Hoehn and Yahr scores, so global motor severity could not be mapped directly onto pause metrics.
Recording conditions differed across sites. Some data came from in-person recordings and some from online collection during COVID-19 restrictions. Manual inspection helped, but recording modality could still affect pause measurement.
The sample was not broad Parkinson’s disease. Participants had to tolerate at least 12 hours without dopaminergic medication, and the Parkinson’s group had more men than women. Results may not generalize cleanly to advanced disease, severe cognitive impairment, or patients unable to complete medication withdrawal.
Questions About Parkinson’s Speech Pauses
Do more pauses mean someone has Parkinson’s disease?
No. Pause timing is too nonspecific for diagnosis. The finding is more useful for understanding speech fluency and therapy targets in people already known to have Parkinson’s disease.
Why did long sentences produce such a large effect?
Long sentences require more planning, respiratory coordination, and working-memory management. Parkinson’s disease can affect motor timing and cognitive control, so longer utterances can expose problems that short phrases hide.
Why did MoCA relate to pause count but not pause duration?
One plausible split is that cognitive load increases how often speech planning is interrupted, while motor-speech severity influences how long interruptions last. The study supports that pattern, but it did not include detailed neuropsychological testing.
Could pause timing guide speech therapy?
Potentially. Pause metrics may help identify whether a patient needs work on pacing, respiratory phrasing, sentence planning, cueing, or rate control. Longitudinal treatment studies are still needed before pause timing can be used as a validated outcome marker.
References
- Mollaei F, Evans H, Pool A. Pause characteristics of sentence production in Parkinson’s disease: insights from sentence complexity and length. PLOS One. 2026;21(4):e0330808. doi:10.1371/journal.pone.0330808
- Huber JE, Darling M, Francis EJ, Zhang D. Impact of typical aging and Parkinson’s disease on the relationship among breath pausing, syntax, and punctuation. American Journal of Speech-Language Pathology. 2012;21(4):368-379. doi:10.1044/1058-0360(2012/11-0059)
- Lee J, Huber J, Jenkins J, Fredrick J. Language planning and pauses in story retell: evidence from aging and Parkinson’s disease. Journal of Communication Disorders. 2019;79:1-10. doi:10.1016/j.jcomdis.2019.02.004
- Andrade EIN, Manxhari C, Smith KM. Pausing before verb production is associated with mild cognitive impairment in Parkinson’s disease. Frontiers in Human Neuroscience. 2023;17:1102024. doi:10.3389/fnhum.2023.1102024
- Lowit A, Marchetti A, Corson S, Kuschmann A. Rhythmic performance in hypokinetic dysarthria: relationship between reading, spontaneous speech and diadochokinetic tasks. Journal of Communication Disorders. 2018;72:26-39. doi:10.1016/j.jcomdis.2018.02.005
- Fumel J, Bahuaud D, Weed E, Fusaroli R, Basirat A. A systematic review and Bayesian meta-analysis of acoustic measures of prosody in Parkinson’s disease. Journal of Speech, Language, and Hearing Research. 2024;67(8):2548-2564. doi:10.1044/2024_JSLHR-23-00588