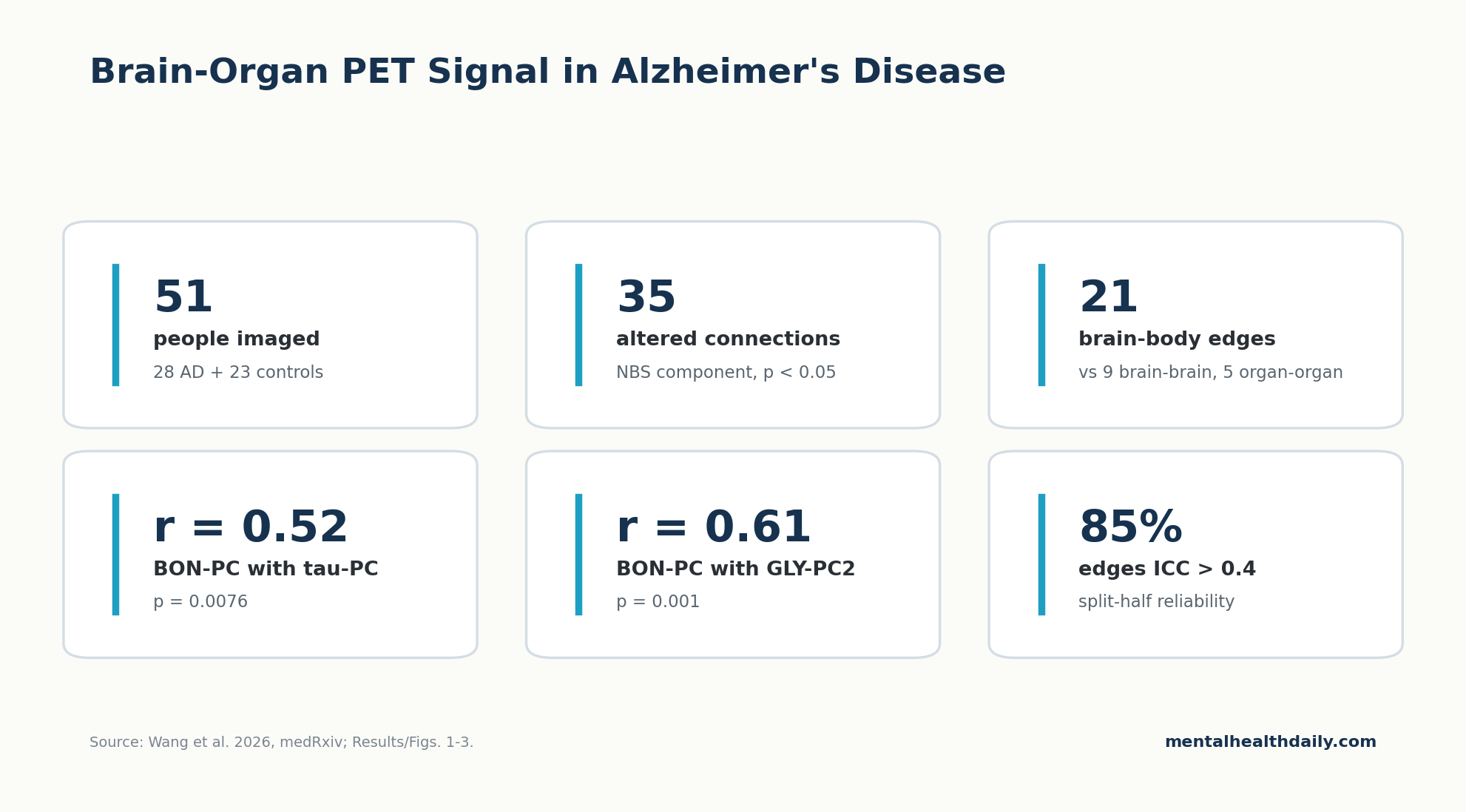
A 2026 total-body tau-PET study of 28 people with Alzheimer’s disease and 23 biomarker-negative controls found stronger brain-organ network connectivity in Alzheimer’s disease than in biomarker-negative controls: 35 altered connections, including 21 brain-body edges, plus AD-only links between brain-organ coupling, cortical tau burden, MRI-derived glymphatic markers, and cognition.1 The result is best read as a source-numbered systems-biology signal, not as proof that the body causes Alzheimer’s or that a clinic can order a brain-organ coupling test today.
Research Highlights
- AD showed 35 altered network connections: Wang et al. found a network-based-statistic component with 35 supra-threshold edges in 28 Alzheimer’s patients vs. 23 controls, adjusted for age, sex, and education.1
- Most altered edges crossed brain-body boundaries: 21 of the 35 altered connections were brain-body links, compared with 9 brain-brain and 5 organ-organ connections.1
- Tau tracked the brain-organ signal: the brain-organ network principal component correlated with the cortical tau principal component in the AD group (r = 0.52, p = 0.0076).1
- Glymphatic MRI markers also tracked coupling: brain-organ connectivity correlated with GLY-PC1 (r = 0.40, p = 0.045) and GLY-PC2 (r = 0.61, p = 0.001), 2 components derived from 11 MRI-based clearance proxies.1
- The method is promising but early: roughly 85% of edge-wise split-half reliability values exceeded ICC 0.4, but the study was cross-sectional, single-center, and posted as a 2026 preprint.1
Brain-organ network connectivity means correlated low-frequency signal changes across brain regions and extracranial organs. In this study, the signal came from plateau-phase total-body tau-PET, not from ordinary resting-state fMRI.
Researchers reconstructed the 60–70 minute post-injection PET window into 60 consecutive 10-second frames, extracted time-activity curves from 10 bilateral cortical regions and 9 extracranial regions, regressed out motion-related variance, and then computed pairwise correlations across the remaining time series.1
That method matters because the old brain-only Alzheimer’s frame leaves out physiology that can plausibly shape neurodegeneration: vascular pulsatility, autonomic flexibility, sleep-linked cerebrospinal-fluid movement, liver and kidney clearance, inflammation, and heart-brain signaling. Wang et al. did not prove those pathways are causal.
They did show that an AD cohort had a measurable whole-body network signature even when conventional static PET did not show extracranial tau differences.1
35 Altered Connections Were Mostly Brain-Body Edges
Wang et al. used a network-based statistic (NBS), a method that tests whether a connected subnetwork differs between groups while controlling family-wise error across many possible edges. After adjustment for age, sex, and education, the AD group showed significantly stronger brain-organ connectivity than biomarker-negative controls: 35 supra-threshold connections survived the NBS procedure.1
The altered network was more than a brain-network result wearing a whole-body label. The 35 edges split into 3 categories:
- 21 brain-body connections linking cortical regions with extracranial tissues.
- 9 brain-brain connections within the cerebral network.
- 5 organ-organ connections among extracranial tissues.
Hub analysis pointed to the right occipital and temporal cortices, the spinal cord, kidneys, liver, skeleton, and heart as prominent nodes in the altered network. The paper highlighted right occipital-to-liver, right temporal-to-skeletal muscle/heart, and spinal cord-to-left parietal links as examples of the reorganized pattern.1
Important calibration: stronger coupling is not automatically healthier coupling. Wang et al. interpreted the AD pattern as pathological hypersynchronization: the brain and body may be moving together more rigidly, with less adaptive buffering, rather than communicating with useful flexibility.
Tau and Glymphatic Proxies Carried the Cognition Link
Static PET behaved as expected inside the brain. AD patients had higher tau SUVRs across major cortical lobes after false-discovery-rate correction, while extracranial tau SUVRs did not significantly differ between AD and control groups.1
That contrast is central: the whole-body result was a dynamic connectivity signal, not a claim that tau tracer uptake was broadly higher throughout the body.
To reduce high-dimensional data into interpretable summary variables, Wang et al. used probabilistic principal component analysis. The cortical tau component (SUVR-PC) explained 70% of tau variance, and the brain-organ connectivity component (BON-PC) explained 50% of altered-connection variance.
Within the AD group, BON-PC correlated with SUVR-PC (r = 0.52, p = 0.0076). Higher tau burden also correlated with worse cognition: MMSE r = −0.56 (p = 0.0035) and MoCA r = −0.46 (p = 0.0298), adjusted for age, sex, and education.1
Glymphatic proxies added a second path. The researchers derived 11 MRI-based glymphatic indices, including choroid plexus volume fraction, perivascular-space volume fractions, free-water indices, analysis-along-perivascular-space indices, and global BOLD-CSF coupling. Their first 2 glymphatic components explained 32% and 28% of variance.
BON-PC correlated with both GLY-PC1 (r = 0.40, p = 0.045) and GLY-PC2 (r = 0.61, p = 0.001).1
Mediation models were exploratory, but they sharpen the interpretation. In a parallel model for MMSE, BON-PC predicted both SUVR-PC (a1 = 0.277, p = 0.018) and GLY-PC1 (a2 = 0.142, p = 0.032); both mediators then independently predicted lower MMSE scores (SUVR-PC b1 = −1.815, p < 0.001; GLY-PC1 b2 = −2.880, p = 0.001).
After both mediators entered the model, the direct BON-to-MMSE path was no longer significant (c’ = 0.603, p = 0.097).1
For MoCA, the same 2 mediator paths remained significant, but the direct BON-to-MoCA path was attenuated rather than eliminated (c’ = 0.600, p = 0.049). That is why the most direct source-faithful language is not “brain-organ hypersynchrony causes cognitive decline.” It is: elevated dynamic brain-organ coupling in this AD cohort shared variance with cognitive impairment through cortical tau burden and MRI-derived glymphatic dysfunction.1
Why Hypersynchrony Is Not Automatically Good Coupling
Synchrony can be healthy when it reflects flexible coordination. Heart rate, respiration, blood pressure, cerebrospinal-fluid movement, and cortical activity all interact.
Network physiology research has long treated organ systems as dynamically linked rather than isolated machines.2 Visceral signals also shape brain function in attention, emotion, and bodily awareness.3
Pathological hypersynchrony is different. In Wang et al.’s interpretation, the AD network may have lost physiological flexibility: slow vascular, autonomic, and tracer-exchange fluctuations propagate through brain and body with too little damping.
That fits a broader aging-biology idea in which disease reduces complex variability and pushes systems toward rigid coupling.
Alzheimer’s biology gives this idea a plausible route. Neurovascular dysfunction can reduce the brain’s ability to buffer pressure and flow changes.
Tau-vulnerable posterior cortices may then become more exposed to systemic low-frequency fluctuations. The spinal cord can carry cerebrospinal-fluid, autonomic, inflammatory, and vascular signals between central and peripheral compartments.
Liver, kidney, heart, and skeletal signals can enter the network even without higher extracranial tau SUVRs because their role is physiological regulation, not necessarily tau deposition.1
Total-Body PET Makes the Signal Interesting and Fragile
The technical novelty is the reanalysis of standard late-phase total-body PET data as a quasi-dynamic network signal. Whole-body functional PET had already shown that cross-organ metabolic connectivity can be measured with PET-derived time-varying signals.4
Wang et al. applied a related logic to a biomarker-defined Alzheimer’s cohort using the tau tracer 18F-PI-2620.
What makes the method interesting: it captures brain and extracranial tissues in one acquisition window, then uses temporal correlation to ask whether regions fluctuate together. That is closer to a systems-physiology map than a static tracer-uptake map.
What makes the method fragile: late-phase PET fluctuations can reflect hemodynamics, tracer exchange, motion, respiratory displacement, scanner noise, and preprocessing choices. Wang et al. tried to reduce obvious artifacts with motion correction, organ segmentation, aorta normalization, 28 nuisance regressors, NBS correction, and split-half reliability testing.
The roughly 85% edge-wise ICC-above-0.4 result is reassuring, but it does not remove the need for external replication.1
The strongest near-term use is research stratification, not clinical diagnosis. A repeatable BON signature could help researchers ask whether Alzheimer’s progression differs in people with vascular stiffness, sleep apnea, autonomic dysfunction, liver disease, kidney disease, or other systemic stressors.
That is a more disciplined claim than turning a 51-person preprint into a new treatment framework.
Sleep, Vascular Pulses, and Liver Clearance Are Adjacent Clues
Wang et al.’s glymphatic interpretation lands inside a real adjacent literature. The glymphatic system is a perivascular clearance pathway that helps move cerebrospinal fluid and interstitial fluid through brain tissue, including routes relevant to amyloid-beta waste removal.5
It is not a magic drain, but it gives sleep, vascular pulsatility, and brain waste clearance a shared biological vocabulary.
Several adjacent findings make the Wang result plausible without proving it:
- Arterial pulsations drive CSF flow: Mestre et al. found that cerebrospinal-fluid flow is driven by arterial pulsations and reduced in hypertension, linking vascular mechanics to clearance biology.6
- Sleep couples neural, blood-flow, and CSF rhythms: Fultz et al. showed coupled electrophysiological, hemodynamic, and CSF oscillations during human sleep, giving sleep a direct physiological bridge to fluid movement.7
- Glymphatic failure is a dementia hypothesis: Nedergaard and Goldman argued that impaired clearance may be a convergent pathway into dementia, more than an Alzheimer’s side note.8
- Peripheral amyloid handling is biologically plausible: Cheng et al. described physiological beta-amyloid clearance by the liver, supporting the narrower claim that extracranial organs can participate in Alzheimer’s-relevant protein handling.9
None of those papers means that treating sleep apnea, hypertension, or liver dysfunction will normalize BON-PC or slow tau spread through the exact Wang pathway. They do mean that the paper’s brain-body framing is not random speculation.
It is a new imaging readout placed on top of an existing physiology literature.
Limits of the Wang Brain-Organ Analysis
This is a preprint and a small imaging study. The 51-person case-control comparison is useful for signal discovery, but the AD-only correlation and mediation models rest on 28 patients.
Even with careful covariate adjustment, a 28-person subgroup can produce unstable estimates, especially when the variables are high-dimensional principal components rather than simple clinical measurements.
Causality remains open. The mediation diagrams are statistical models fitted to cross-sectional data. They can show that the data are consistent with a pathway from BON-PC through tau or glymphatic proxies to cognition.
They cannot show temporal order. Tau pathology could increase network rigidity, glymphatic impairment could worsen both tau and network physiology, or a third factor such as vascular disease could influence all 3.
Glymphatic measurement is indirect. The MRI proxies are useful, but they are not direct measurements of cerebrospinal-fluid waste clearance. Free water, perivascular spaces, ALPS indices, and BOLD-CSF coupling can all be influenced by vascular, motion, and tissue-structure factors.
Wang et al. were appropriately cautious in describing the mediation as exploratory.1
Clinical translation is not here yet. Total-body PET is expensive and not standard dementia workup. The paper’s more practical contribution is conceptual: it suggests that Alzheimer’s imaging should not stop at plaques, tangles, and cortical atrophy when systemic physiology may help explain why pathology accumulates or why cognition declines at different rates.
Reader Questions About Alzheimer’s Brain-Organ PET
Did the 2026 study prove brain-organ hypersynchrony causes Alzheimer’s decline?
No. It found a cross-sectional association pattern in which AD patients had 35 altered brain-organ network connections, and the AD-only BON component correlated with tau and glymphatic MRI components.
Longitudinal and intervention studies are needed before causality is credible.1
Why do 21 brain-body edges matter if extracranial tau was not higher?
The result separates tracer uptake from dynamic coupling. Static tau SUVRs were higher in the AD cortex, not in extracranial organs, while dynamic PET fluctuations still showed altered brain-body synchronization.
That points to physiological coordination rather than whole-body tau deposition.1
Could a dementia clinic order BON-PC testing now?
No. BON-PC is a research-derived principal component from dynamic total-body PET processing.
It is not a validated clinical biomarker, diagnostic test, or treatment-selection tool.
Does this make sleep treatment an Alzheimer’s therapy?
No. Sleep remains important because it affects vascular, metabolic, and glymphatic physiology, and treating sleep apnea or insomnia can be medically worthwhile for its own reasons.
Wang et al. did not test whether sleep treatment changes BON-PC, tau burden, or cognition.
What is the most useful takeaway from the liver, heart, kidney, and spinal-cord links?
The useful takeaway is systems-level risk modeling: future Alzheimer’s studies should measure vascular, sleep, autonomic, kidney, liver, and inflammatory variables alongside amyloid and tau, because peripheral physiology may help explain differences in clearance, network rigidity, and cognitive trajectory.
References
- Wang L, Li L, Tao Y, et al. Brain-organ hypersynchrony and cognitive decline in Alzheimer’s disease: potential links with tauopathy and glymphatic dysfunction. medRxiv. 2026. doi:10.64898/2026.04.22.26351474
- Bartsch RP, Liu KKL, Bashan A, Ivanov PC. Network physiology: how organ systems dynamically interact. PLoS One. 2015;10(11):e0142143. doi:10.1371/journal.pone.0142143
- Critchley HD, Harrison NA. Visceral influences on brain and behavior. Neuron. 2013;77(4):624–638. doi:10.1016/j.neuron.2013.02.008
- Reed MB, Ponce de León M, Vraka C, et al. Whole-body metabolic connectivity framework with functional PET. NeuroImage. 2023;271:120030. doi:10.1016/j.neuroimage.2023.120030
- Hablitz LM, Nedergaard M. The glymphatic system: a novel component of fundamental neurobiology. Journal of Neuroscience. 2021;41(37):7698–7711. doi:10.1523/JNEUROSCI.0619-21.2021
- Mestre H, Tithof J, Du T, et al. Flow of cerebrospinal fluid is driven by arterial pulsations and is reduced in hypertension. Nature Communications. 2018;9:4878. doi:10.1038/s41467-018-07318-3
- Fultz NE, Bonmassar G, Setsompop K, et al. Coupled electrophysiological, hemodynamic, and cerebrospinal fluid oscillations in human sleep. Science. 2019;366(6465):628–631. doi:10.1126/science.aax5440
- Nedergaard M, Goldman SA. Glymphatic failure as a final common pathway to dementia. Science. 2020;370(6512):50–56. doi:10.1126/science.abb8739
- Cheng Y, Tian DY, Wang YJ. Physiological β-amyloid clearance by the liver and its therapeutic potential for Alzheimer’s disease. Acta Neuropathologica. 2023;145(6):717–731. doi:10.1007/s00401-023-02559-z