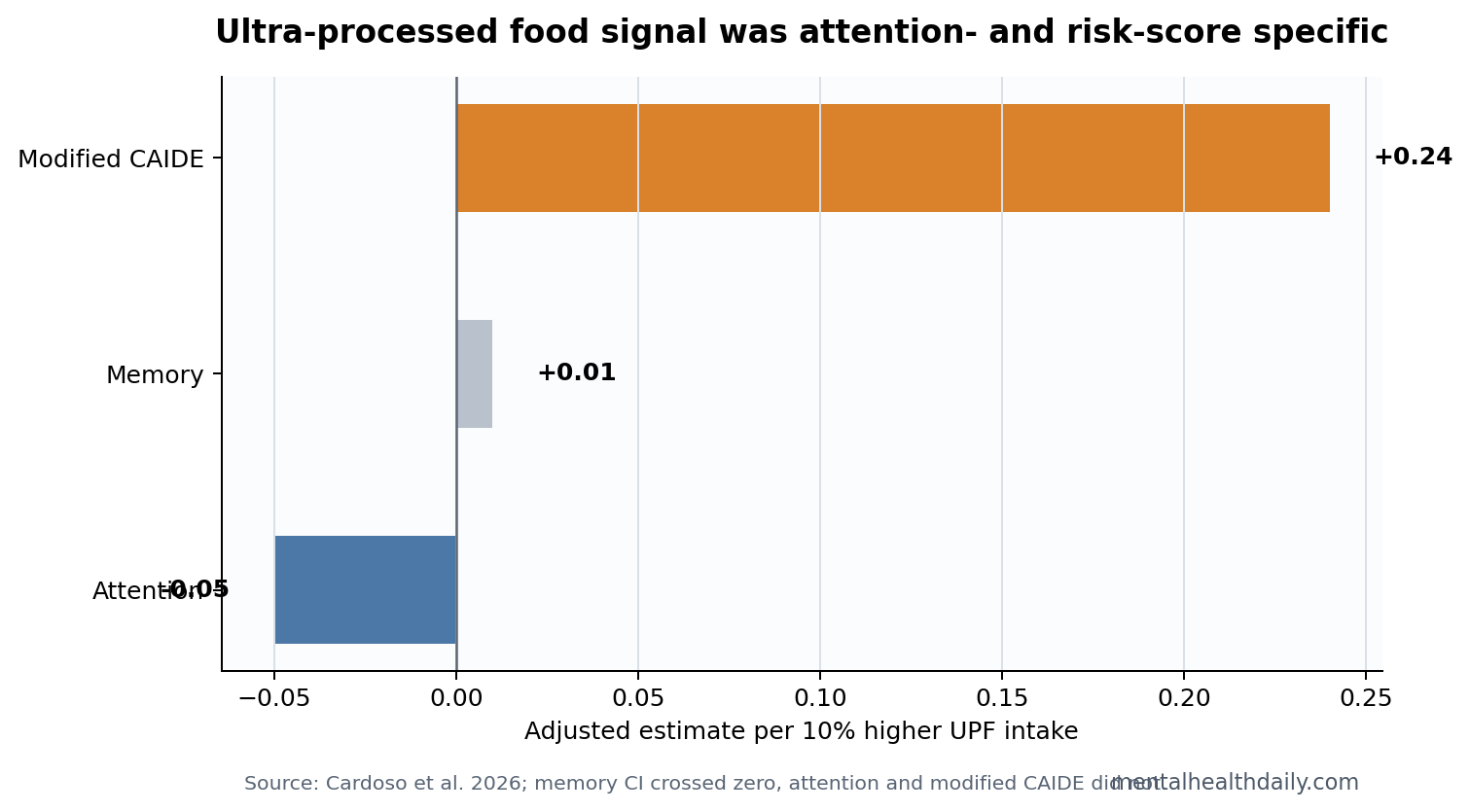
A 2026 Australian study involving 2,192 dementia-free adults found that each 10% higher ultra-processed food intake was associated with 0.05-point lower attention and 0.24-point higher modified CAIDE dementia-risk score.1 The memory result was not significant, so the honest read is attention and risk-score signal, not global cognitive collapse.
Research Highlights
- Attention was lower: Each 10% higher ultra-processed food intake was linked to a 0.05-point lower attention score, 95% CI -0.08 to -0.01, p = 0.012.1
- Dementia-risk score was higher: In 1,891 adults, each 10% higher intake was linked to a 0.24-point higher modified CAIDE score, 95% CI 0.15 to 0.32, p < 0.001.1
- Memory did not move: The adjusted memory estimate was 0.01, 95% CI -0.02 to 0.05, p = 0.389.1
- Diet quality did not erase the signal: Associations were modeled independent of Mediterranean diet adherence in adults aged 40-70 years.1
- Causality remains open: A 2026 cross-sectional study can show association, not that UPFs directly caused cognitive change.
Ultra-processed foods are industrially formulated products such as packaged snacks, sweetened drinks, reconstituted meats, and ready-to-eat meals that often combine refined starches, added sugar, oils, emulsifiers, flavoring agents, and cosmetic additives. The category is not identical to junk food, but it captures a processing pattern that can travel with poorer diet quality, lower fiber, higher energy density, and cardiometabolic risk.
CAIDE is a dementia-risk score built from midlife factors such as age, education, blood pressure, cholesterol, body mass index, and physical activity. A higher modified CAIDE score means a less favorable risk profile, not a dementia diagnosis.
Attention Shifted, Memory Did Not
Cardoso et al. analyzed adults from the Healthy Brain Project and estimated cognition per 10% higher ultra-processed food intake. The clearest cognitive association was attention: -0.05 after full adjustment, with the confidence interval staying below zero.1
Memory did not show the same pattern. The adjusted memory estimate was 0.01, and the confidence interval crossed zero. That makes the result more specific than a broad claim that ultra-processed foods damaged cognition across every domain.
Attention means the ability to hold focus, process information efficiently, and maintain task control. It is often more sensitive to sleep, stress, metabolic health, vascular risk, and medication effects than a single word-list memory score. That makes attention a plausible early signal in a diet-risk study.
The effect size was small at the individual level. A 0.05-point lower score per 10% higher UPF intake should not be sold as a dramatic cognitive drop for 1 person. The public-health question is different: small shifts across thousands of middle-aged adults can still matter when the exposure is common and clusters with other dementia-risk factors.
Higher Modified CAIDE Scores Point Toward Risk Clustering
The modified CAIDE association was larger and more statistically stable than the attention estimate. Each 10% higher UPF intake was tied to a 0.24-point higher risk score, p < 0.001. That matters because ultra-processed food intake can cluster with risk factors that are already plausible dementia-prevention targets: weight, metabolic health, blood pressure, physical activity, and education-linked health behavior.
Risk-score interpretation: the CAIDE result points to a less favorable dementia-risk profile among adults with higher UPF intake during the same period.
Risk clustering: the modified CAIDE score avoids treating diet as an isolated moral choice. A higher UPF pattern may travel with less physical activity, lower food security, fewer cooking resources, higher stress, poorer sleep, or cardiometabolic disease.
Those conditions can all shape dementia risk without requiring 1 additive or 1 food category to be the entire mechanism.
Mechanism candidates:
- Metabolic load: high energy density and lower fiber can worsen insulin resistance, weight gain, and vascular risk.
- Inflammatory tone: low-quality dietary patterns can shift immune and gut-derived signaling, though this study did not prove inflammation mediation.
- Micronutrient displacement: UPF-heavy diets can crowd out fruits, vegetables, legumes, fish, nuts, and whole grains.
- Behavior clustering: diet can mark broader differences in sleep, stress, exercise, and access to preventive care.
Prior Longitudinal Evidence Makes the Signal Harder to Dismiss
A separate Brazilian cohort study linked higher UPF intake to faster cognitive decline over time, which makes the Australian cross-sectional attention finding less isolated.2 Dementia-prevention reviews also place diet, vascular risk, obesity, and physical activity inside the modifiable-risk cluster.3
Still, the Cardoso study does not prove that removing UPFs would improve attention. A randomized dietary intervention would be needed to separate food processing from total diet quality, calories, sleep, income, stress, physical activity, medication use, and baseline health.
The Mediterranean-diet adjustment is important. If the UPF association disappeared after Mediterranean diet adherence entered the model, the result would mostly say that people eating fewer protective foods had worse scores. The reported persistence suggests UPF intake carried information beyond that broad diet-quality index.
Domain specificity: the attention result also fits a prevention model better than a one-step dementia story.
Attention is a near-term cognitive domain that can shift with sleep, glucose stability, vascular load, stress, medication burden, and daily energy regulation. Modified CAIDE is a longer-horizon risk profile.
Seeing both move in the unfavorable direction is more coherent than seeing only a vague global cognition score change, but it still does not identify which pathway is doing the work.
That persistence should be read carefully. Mediterranean diet scores are imperfect, and dietary recall is noisy. UPF intake could still be a marker for unmeasured lifestyle or socioeconomic exposure. The strongest future evidence would use repeated diet measures, objective metabolic markers, cognitive follow-up, and incident dementia outcomes.
The Best Clinical Use Is Risk Conversation, Not Alarm
For a patient, the actionable version is not “never eat packaged food.” It is to reduce the share of daily calories coming from foods engineered to be cheap, shelf-stable, hyperpalatable, and low in fiber. That change should sit beside blood-pressure control, exercise, sleep treatment, smoking cessation, hearing care, diabetes management, and depression care.
Practical substitution logic: the highest-yield changes are usually boring. Replace sweetened drinks with water or unsweetened options, swap snack foods for nuts or fruit when possible, use minimally processed proteins, and build meals around legumes, vegetables, whole grains, and olive oil or similar unsaturated fats. The study supports that direction without pretending diet alone controls dementia risk.
The attention finding also helps set expectations. If a person improves diet, the first benefit may be energy, sleep quality, glucose stability, blood pressure, or weight rather than a noticeable memory change. Cognitive prevention usually works through cumulative risk reduction, not a dramatic day-to-day mental upgrade.
For researchers, the next step is longitudinal specificity. The most useful study would follow UPF intake, diet quality, cardiometabolic markers, attention, memory, and incident cognitive impairment over several years. That design could test whether attention declines first, whether CAIDE changes mediate the association, and whether reducing UPFs changes the trajectory.
A randomized trial would answer a different question. If 2 groups receive diets matched for calories and broad nutrient quality but differing in processing level, any cognitive or metabolic difference becomes easier to attribute to processing itself. Until then, UPF intake should be treated as a risk marker with plausible mechanisms rather than a proven standalone cause.
Reader-level threshold: the evidence is strong enough to justify reducing UPF reliance when the diet is already heavily packaged, but not strong enough to make 1 packaged meal a brain-health emergency. The practical target is pattern change: fewer sweetened drinks, fewer low-fiber snack defaults, more minimally processed staple foods, and better management of the vascular and metabolic risks that CAIDE was built to capture.
Clinically, the result belongs in a prevention bundle. A patient with high UPF intake, hypertension, poor sleep, insulin resistance, hearing loss, depression, and low physical activity needs an integrated plan. Diet can be one lever, but the dementia-risk score reminds readers that brain aging is shaped by multiple modifiable systems at once.
The study also helps prevent overcorrection. A small attention association should not be dismissed because it is not dramatic, and it should not be inflated into proof that packaged foods directly cause dementia. The calibrated position is simpler: higher UPF intake marked a worse attention and dementia-risk profile in this cohort, with enough consistency to justify prevention-oriented dietary change.
That kind of change is usually measured in defaults, not perfection. If UPFs make up a large share of meals, lowering that share while improving protein, fiber, and cardiometabolic care is the reasonable target.
For public health, the result also points upstream. Food price, time, marketing, work schedules, and neighborhood access shape UPF intake. Counseling works better when it is paired with realistic substitutions and attention to the conditions that make minimally processed food easier to choose.
Questions About Ultra-Processed Foods and Cognition
Did the study show that UPFs cause dementia?
No. It found cross-sectional associations with attention and modified CAIDE dementia-risk scores, not incident dementia.
Was memory affected?
Not significantly in the fully adjusted model. The strongest cognitive signal was attention.
How should readers use the UPF finding?
A reasonable target is replacing UPF-heavy meals with higher-fiber, minimally processed foods while also treating blood pressure, sleep, exercise, and metabolic risk. The study supports risk reduction, not panic.
References
- Cardoso BR, et al. Ultra-processed food consumption is associated with poorer attention and higher dementia risk scores. Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. 2026. doi:10.1002/dad2.70335
- Goncalves NG, et al. Association between consumption of ultraprocessed foods and cognitive decline. JAMA Neurology. 2023. doi:10.1001/jamaneurol.2022.4397
- Livingston G, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020. doi:10.1016/s0140-6736(20)30367-6
- Kivipelto M, et al. Risk score for the prediction of dementia risk in 20 years among middle aged people. Lancet Neurology. 2006. doi:10.1016/s1474-4422(06)70537-3