
A 2026 meta-analysis of 8 controlled trials found that AVATAR therapy reduced auditory verbal hallucination severity after treatment, Hedges’ g = −0.40, 95% CI −0.54 to −0.25, across 978 participants.1 The signal is real, but the strongest reading is short-term symptom calibration rather than a finished replacement for standard psychosis care.
Research Highlights
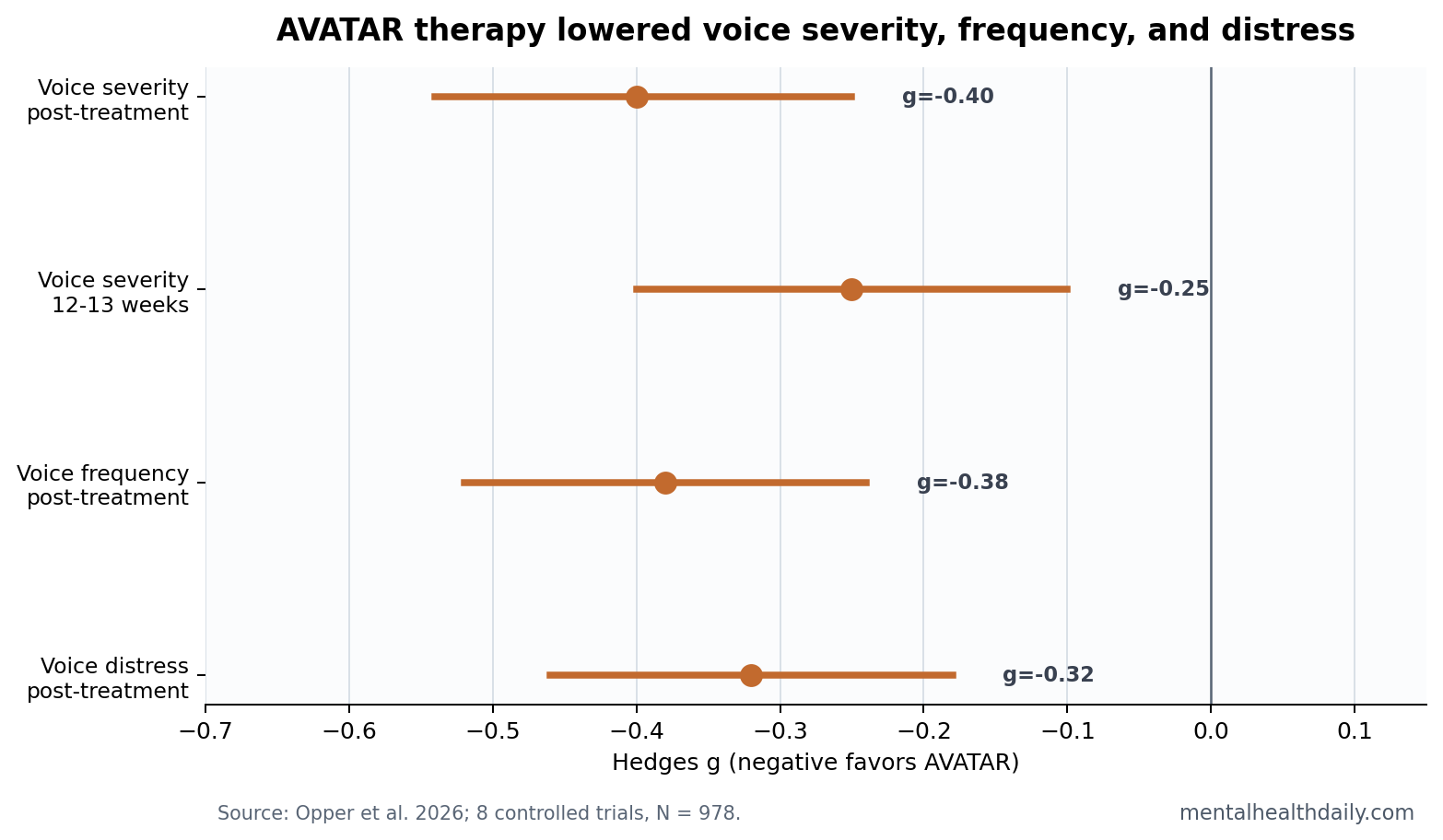
- Voice severity improved: 8 AVATAR trials with 978 participants found lower auditory hallucination severity after treatment, Hedges’ g = −0.40, 95% CI −0.54 to −0.25.1
- Follow-up stayed positive: short-term follow-up still favored AVATAR, g = −0.25, but medium- and long-term estimates came from only 1 study and were very uncertain.1
- Frequency and distress moved too: post-treatment voice frequency improved by g = −0.38 and voice distress by g = −0.32, both favoring AVATAR.1
- Dropout looked comparable: treatment dropout was 24% in AVATAR groups vs. 18% in controls, with risk ratio 1.01, 95% CI 0.43 to 2.35.1
- Comparator choice still matters: control groups included treatment as usual, waitlist, and active controls, and 6 of 8 studies had high overall risk of bias.1
AVATAR therapy is a structured psychological treatment for distressing voices. The person works with a therapist to build a computer-generated representation of the voice, then practices responding to it in a controlled session so the voice feels less powerful, less malevolent, and less uncontrollable.
Mechanism: AVATAR targets the relationship between the voice-hearer and the voice: fear, perceived dominance, loss of control, and distress. For many people with schizophrenia-spectrum disorders, those appraisals drive disability even when medication reduces other psychotic symptoms.
AVATAR Reduced Voice Severity by g = −0.40 After Treatment
Opper et al. pooled 8 randomized or controlled AVATAR trials, representing 9 relevant comparisons. The experimental groups included 554 participants and the control groups included 424 participants. Trial duration ranged from 7 to 16 weeks, with most AVATAR protocols built around roughly 6 to 12 sessions.1
The primary outcome was auditory verbal hallucination severity. Lower scores mean fewer or less severe voice symptoms. At post-treatment, the pooled effect favored AVATAR by Hedges’ g = −0.40, 95% CI −0.54 to −0.25, p < 0.001. In plain English: voice severity was lower in the AVATAR groups than in the comparison groups, with a small-to-moderate effect.
Standardized mean difference means the result is expressed in standard-deviation units so trials using different voice-rating scales can be pooled. A g around −0.40 is not a miracle effect. It is also not trivial when the target symptom is persistent distressing voices after ordinary care.
Voice Frequency and Distress Also Improved
Severity was not the only outcome moving in the same direction. Voice frequency improved at post-treatment, Hedges’ g = −0.38, 95% CI −0.52 to −0.24. Voice distress improved by g = −0.32, 95% CI −0.46 to −0.18. Those 2 outcomes matter because a voice-focused therapy could plausibly reduce distress even when it does not eliminate voices.
The distinction is clinically important. A person may still hear voices but experience them as less threatening, less dominant, or less emotionally overwhelming. AVATAR’s design fits that target: the exposure is not random confrontation with symptoms; it is repeated practice changing the social and emotional meaning of the voice.
Short-term follow-up kept the direction but weakened the certainty. Voice severity remained lower at 12 to 13 weeks, g = −0.25, 95% CI −0.40 to −0.10. Frequency remained lower, g = −0.34. Distress remained lower, g = −0.20. Medium- and long-term follow-up were much less informative because only 1 study contributed those estimates.1
Active Controls Keep the Effect From Looking Like Pure Hype
The subgroup detail makes this meta-analysis more useful than a simple pooled result. Subgroup analyses separated treatment as usual, treatment as usual plus waitlist, and active control comparisons. The post-treatment severity effect favored AVATAR in each control subgroup, including active controls, where g = −0.33, 95% CI −0.52 to −0.15.1
That does not erase all expectancy and attention concerns. Psychotherapy trials are difficult to blind, and a technologically novel therapy can carry strong expectation effects. But a signal against active controls is more useful than a signal against waitlist alone.
Craig et al.’s earlier single-blind randomized trial helped establish the modern AVATAR evidence base, comparing AVATAR therapy with supportive counseling in people with psychosis who heard distressing voices.2 The newer pooled estimate places that trial inside a broader pattern rather than treating it as a standalone proof.
Comparator discipline: active controls matter because voice-hearing therapy is highly sensitive to therapist time, expectancy, novelty, and the chance to discuss frightening experiences in detail. A future AVATAR trial should match contact time, therapist attention, safety monitoring, and credibility as closely as possible before attributing the difference to the avatar element itself.
Risk of Bias and Follow-Up Keep the Claim Narrow
The review rated 2 studies as low risk of bias and 6 as high overall risk of bias. That is the main reason the article should not be read as a victory lap for virtual therapy. A pooled effect can be statistically clean while still depending on small trials, variable protocols, expectancy, and inconsistent control conditions.
Evidence-strength note: this was a meta-analysis of controlled trials, which is stronger than a case series or open pilot. The limits are trial quality, treatment heterogeneity, and durability. The most defensible claim is that AVATAR therapy reduces short-term voice severity, frequency, and distress in controlled trials. The less defensible claim is that it is a proven long-term replacement for coordinated psychosis treatment.
Dropout did not look dramatically worse than control. The pooled AVATAR treatment-dropout proportion was 24%, compared with 18% in control groups, and the dropout risk ratio was 1.01, 95% CI 0.43 to 2.35. That wide interval leaves uncertainty, but it does not show a clear tolerability penalty.
AVATAR Fits a Specific Voice-Hearing Problem
The strongest clinical niche is not “psychosis treatment” in general. It is distressing auditory verbal hallucinations where the person experiences the voice as powerful, malevolent, intrusive, or uncontrollable. Those appraisals are direct targets for a therapy that changes voice dominance and the person’s response to the voice.
- Best-fit target: persistent distressing voices despite ordinary treatment, especially when fear and perceived voice power are central.
- Weaker target: broad negative symptoms, functional recovery, medication adherence, relapse prevention, or cognitive impairment.
- Research gap: larger trials with standardized active controls, longer follow-up, and clearer reporting of adverse events.
Older AVATAR reviews were cautious because the evidence base was small.3 The 2026 review changes the center of gravity: there are now enough controlled data to take the therapy seriously. It still belongs beside, not above, broader care.
The target should also stay symptom-specific. Negative symptoms such as reduced motivation, limited emotional expression, and social withdrawal have their own treatment literature, and psychological interventions have produced mixed, modest effects there.4 AVATAR is built for distressing voices, not for the full schizophrenia syndrome.
That distinction protects both readers and patients. A focused voice intervention can be valuable without promising broad recovery. The better clinical question is which voice-hearers need a targeted dominance-and-distress intervention alongside medication, cognitive behavioral therapy for psychosis, family work, sleep care, and rehabilitation.
Service fit: AVATAR also requires trained therapists, software, privacy controls, and a setting where voice content can be discussed safely. Those requirements make it different from a generic digital self-help tool. The intervention is technologically mediated, but the active clinical work still depends on structured therapist guidance.
Longer-Term Durability Is Still the Missing Test
Durability is the next hard question. Short-term follow-up around 12 to 13 weeks still favored AVATAR, but medium- and long-term follow-up were based on 1 study. That leaves relapse, maintenance sessions, booster dosing, and symptom recurrence mostly unanswered.
For a therapy aimed at distressing voices, durability should be measured in several ways. Voice severity can improve while distress returns. Distress can improve while frequency stays high. A person may gain confidence in sessions but lose that confidence when voices intensify during stress, sleep loss, substance use, or medication disruption.
A mature AVATAR evidence base would report at least 4 follow-up layers: symptom severity, voice distress, functional impairment, and need for additional crisis or medication support. The 2026 meta-analysis supports a short-term symptom effect. It does not yet prove that the new relationship to the voice holds across ordinary life stressors for 6 to 12 months.
Questions About AVATAR Therapy for Voices
Does AVATAR therapy stop voices completely?
The 2026 meta-analysis supports reduced severity, frequency, and distress. It does not prove voice cessation for most people.
Is the effect large?
No. The main post-treatment severity effect was small-to-moderate, g = −0.40. That can be useful for a difficult symptom target, but it is not a cure-sized effect.
Should AVATAR replace CBT for psychosis or medication?
No. Current evidence supports AVATAR as a focused add-on or specialized option for distressing voices, not as a replacement for medication management, CBT for psychosis, crisis care, or rehabilitation.
References
- Opper I, et al. Audio Visual Assisted Therapy Aid for Refractory Auditory Hallucinations (AVATAR) therapy for voice hearers: systematic review and meta-analysis. BJPsych Open. 2026. https://doi.org/10.1192/bjo.2026.11014
- Craig TKJ, Rus-Calafell M, Ward T, et al. AVATAR therapy for auditory verbal hallucinations in people with psychosis: a single-blind, randomized controlled trial. Lancet Psychiatry. 2018;5(1):31-40. doi:10.1016/s2215-0366(17)30427-3
- Aali G, Kariotis T, Shokraneh F. AVATAR therapy for people with schizophrenia or related disorders. Cochrane Database of Systematic Reviews. 2020;5:CD011898. doi:10.1002/14651858.cd011898.pub2
- Lutgens D, Gariepy G, Malla A. Psychological and psychosocial interventions for negative symptoms in psychosis: systematic review and meta-analysis. British Journal of Psychiatry. 2017;210(5):324-332. doi:10.1192/bjp.bp.116.197103