A 2026 CARDIOSA-12 secondary analysis found that active hypoglossal nerve stimulation improved sleepiness, insomnia, snoring, and sleep-related function, but objective cognitive test performance mostly did not improve compared with partially therapeutic stimulation.1 Symptom relief and measurable cognitive recovery answer separate clinical questions in treated obstructive sleep apnea.
Research Highlights
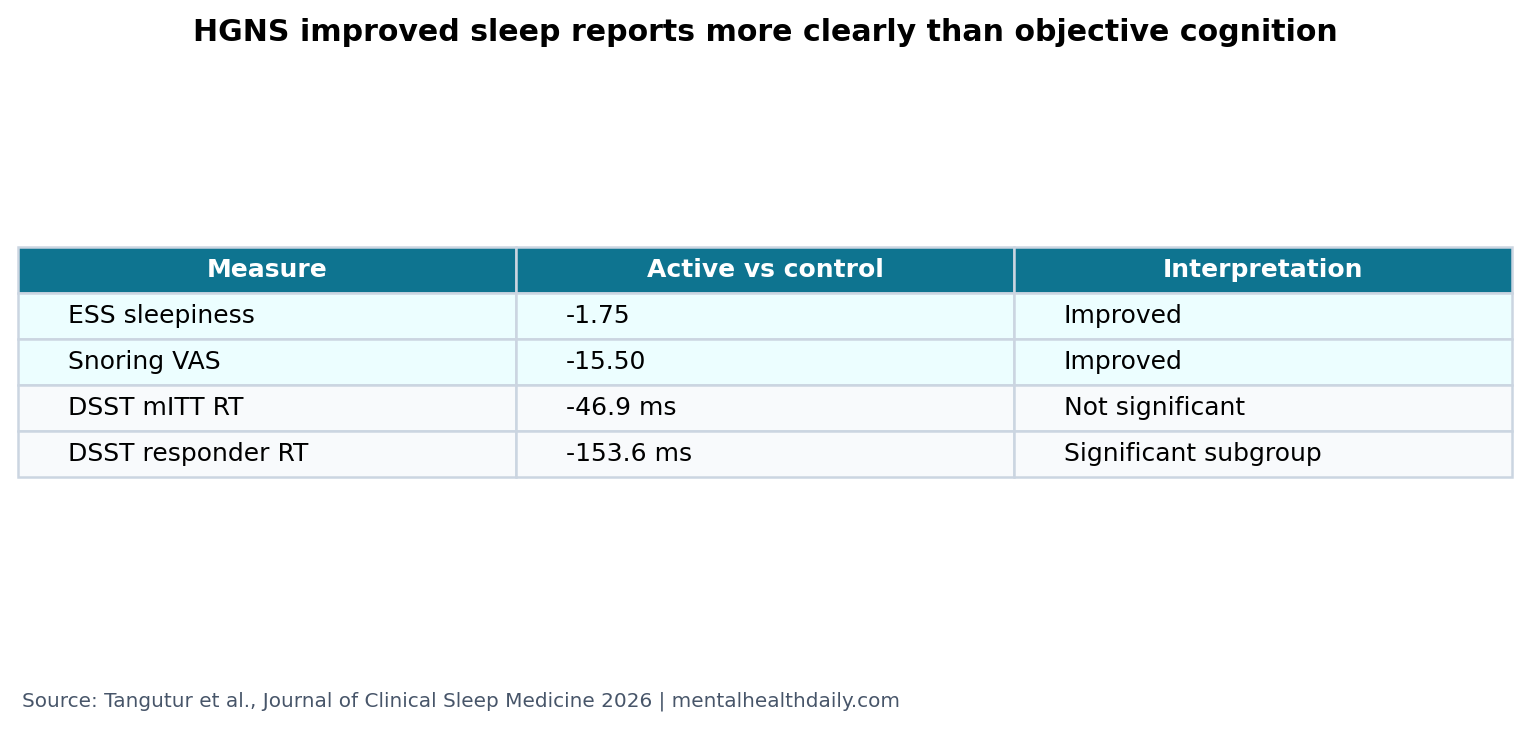
- Subjective outcomes improved: active HGNS improved Epworth Sleepiness Scale by −1.75, Snoring VAS by −15.50, ISI by −2.37, and FOSQ by 0.88.1
- Main cognitive tests were not significant: DSST reaction time changed by −46.9 ms in the mITT cognitive subset, with a 95% CI crossing no effect.1
- Responder analysis looked more favorable: participants with at least 50% AHI reduction improved DSST reaction time by −153.6 ms.1
- Breathing improved modestly over control: active HGNS lowered AHI by 4.9 events/hour compared with partially therapeutic HGNS.1
- Interpretation is exploratory: 60 participants completed PRO analysis, but only 43 underwent cognitive testing.1
Hypoglossal nerve stimulation (HGNS) is an implanted treatment for obstructive sleep apnea that stimulates the nerve controlling tongue movement. The goal is to keep the upper airway more open during sleep by reducing tongue-related airway collapse.
Obstructive sleep apnea repeatedly interrupts breathing during sleep. It can worsen sleepiness, mood, cardiovascular risk, driving safety, and cognitive performance, but cognitive recovery after treatment has been uneven across studies.
Sleep Symptoms Improved Across All Patient-Reported Outcomes
Tangutur et al. analyzed a 10-week double-blind randomized crossover trial in adults already implanted and optimized on HGNS. Participants completed 4 weeks of active HGNS and 4 weeks of control HGNS, with the control condition set at a partially therapeutic level rather than a fully inactive sham.1
In the modified intention-to-treat analysis, active HGNS improved all measured patient-reported outcomes. Epworth Sleepiness Scale changed by −1.75, Snoring Visual Analog Scale by −15.50, Insomnia Severity Index by −2.37, and Functional Outcomes of Sleep Questionnaire by 0.88.1
Those changes line up with the symptom target of sleep-apnea treatment. Less snoring, less sleepiness, and better sleep-related function are direct patient-facing benefits even when cognitive test scores do not move.
Objective Cognition Mostly Did Not Improve in the Main Analysis
The cognitive-testing subset included 43 participants. Active HGNS did not significantly improve the primary cognitive measures compared with partially therapeutic control HGNS. PVT reciprocal reaction time changed by 0.05 1/ms (95% CI −0.03 to 0.13; p = 0.239), and DSST reaction time changed by −46.9 ms (95% CI −113.1 to 19.2; p = 0.160).1
PVT is a psychomotor vigilance test measuring sustained attention and reaction time. DSST is a digit symbol substitution task that reflects processing speed, attention, and executive efficiency. Neither test captures every cognitive complaint a patient may notice in daily life.
The result is not a contradiction. Sleep symptoms can improve before objective cognition changes, and brief performance tests may miss fatigue relief, mood improvement, or functional gains that patients feel.
DSST Reaction Time Improved Only in AHI Responders
The per-protocol analysis focused on participants who had at least a 50% AHI reduction with active HGNS compared with control. In that subgroup, DSST reaction time improved by −153.6 ms (95% CI −285.3 to −22.0; p = 0.025).1
AHI means apnea-hypopnea index, the number of breathing interruptions per hour of sleep. The responder finding suggests that cognitive benefit may require a sufficiently large breathing improvement beyond turning the device to active settings.
Calibrated read: the responder analysis is plausible but exploratory. It could reflect true threshold biology, regression to the mean, selection of better responders, or limited power in the full cognitive sample.
Partially Therapeutic Control Makes the Trial Harder and More Useful
The control condition was not a pure placebo. It produced modest physiologic improvement, and participants used it for longer per night than active HGNS: 8.19 hours/night vs. 6.80 hours/night.1
This makes the comparison conservative. Active HGNS had to beat a lower-level version of the same intervention, not untreated sleep apnea. That design helps isolate dose/intensity effects, but it can shrink differences between conditions.
Blinding was also imperfect. At trial completion, 87.9% of responders correctly guessed their treatment order.1 That matters most for subjective outcomes, because perceived treatment intensity can influence symptom reports.
OSA Treatment Often Helps Symptoms More Reliably Than Cognition
The pattern fits older sleep-apnea evidence. APPLES, a large CPAP trial, found limited and complex neurocognitive changes despite treating obstructive sleep apnea.3 A meta-analysis of CPAP and mandibular advancement devices also showed that treatment effects vary by outcome and modality.4
Dedhia et al.’s parent CARDIOSA-12 cardiovascular trial provided the randomized HGNS framework for this secondary analysis.2 Tangutur et al. add a narrower point: in optimized HGNS users, patient-reported sleep function improved more clearly than objective cognitive performance.1
Supported: active HGNS improved sleep-related patient-reported outcomes in this crossover trial.
Not supported: claiming broad cognitive restoration from HGNS, especially when the main cognitive analysis did not reach statistical significance.
Subjective Benefit and Cognitive Recovery Are Different Endpoints
The study helps separate 2 patient-centered claims that are often blurred. One claim is that active HGNS makes treated patients feel and function better during the day. The patient-reported outcomes support that. The other claim is that active HGNS measurably restores attention, processing speed, or executive function. The main cognitive analysis did not support that with statistical confidence.
Symptom relief: lower sleepiness, less snoring, less insomnia, and better sleep-related function can improve daily life even without a cognitive-test change. Those outcomes are not cosmetic; they are part of why OSA is treated.
Objective cognition: reaction-time and symbol-substitution tasks are narrower. They may require larger AHI reductions, longer treatment duration, worse baseline impairment, or more sensitive cognitive batteries before a signal appears.
Measurement mismatch: patients may report better energy, mood, or alertness while a 3-minute vigilance task stays unchanged. Conversely, a test can improve from practice or statistical noise without changing daily function.
The clean clinical message is to track both. A patient who feels better after HGNS may still have residual OSA, persistent cognitive symptoms, medication effects, depression, insomnia, circadian disruption, or vascular risk that needs separate evaluation. Repeat sleep testing and targeted cognitive assessment answer different questions.
Future HGNS cognition studies should enroll people with measurable baseline cognitive impairment, prespecify cognitive endpoints, use longer follow-up, and separate airway-response thresholds from device exposure. Otherwise, symptom benefit and cognitive recovery will keep being treated as interchangeable when they are not.
Baseline severity is especially important. A participant with normal processing speed at baseline has little room to improve on DSST, even if sleep quality improves. A participant with slower baseline reaction time, more hypoxemia, or more daytime sleepiness may have more measurable cognitive upside. That is exactly the kind of subgroup question this secondary analysis raises but cannot settle.
The partially therapeutic control also matters for real-world interpretation. If low-level stimulation already reduces AHI and symptoms somewhat, the active-vs-control difference underestimates the contrast between optimized HGNS and untreated OSA. It also makes the study less useful for deciding whether HGNS beats other treatments.
For patients already using HGNS, the practical move is not to dismiss cognitive complaints because the device improves breathing. Persistent brain fog after OSA treatment should prompt a broader review: residual AHI, oxygen desaturation, insomnia, depression, sedating medications, cardiometabolic risk, and sleep duration can all keep cognition impaired after airway treatment improves.
That broader review keeps device success separate from unresolved cognitive symptoms.
It also protects against the opposite mistake: calling HGNS ineffective because a short cognitive battery did not move. The trial’s patient-reported outcomes still favored active stimulation, and those outcomes matter for daytime function.
The calibrated read is split, not negative. HGNS can improve sleep-related symptoms in selected implanted patients while leaving the cognition question only partly answered, especially when the comparator is not an inert sham and the cognitive subset is smaller than the symptom-analysis sample.
Questions About HGNS and Cognition
Does hypoglossal nerve stimulation improve cognition?
Not clearly in the main analysis. Objective cognitive tests did not significantly improve, although DSST reaction time improved in the responder subgroup.
Why did symptoms improve if cognition did not?
Sleepiness, snoring, insomnia, and daily function are not the same endpoint as reaction time. Patients can feel better without showing measurable gains on brief cognitive tasks.
Is HGNS a replacement for CPAP?
HGNS is an option for selected OSA patients, often when CPAP is not tolerated or appropriate. This study did not compare HGNS with CPAP.
What result would strengthen the cognition claim?
A larger trial powered for cognitive endpoints, with stronger blinding and a less therapeutic control condition, would better test whether AHI improvement causes objective cognitive gains.
Should persistent brain fog after HGNS be ignored?
No. Device response and cognitive symptoms should be evaluated separately. Residual apnea, oxygen dips, insomnia, depression, medication effects, short sleep, and vascular risk can all keep attention or memory impaired after breathing improves, especially in older patients.
References
- Tangutur A, Yu PK, Basner M, Keenan BT, Dedhia RC. Subjective and objective measures of sleep-related function from the Cardiovascular Endpoints For Obstructive Sleep Apnea with Twelfth Cranial Nerve Stimulation (CARDIOSA-12) trial. Journal of Clinical Sleep Medicine. 2026;22:45. doi:10.1007/s44470-026-00067-x
- Dedhia RC, Bliwise DL, Quyyumi AA, et al. Hypoglossal nerve stimulation and cardiovascular outcomes for patients with obstructive sleep apnea: a randomized clinical trial. JAMA Otolaryngology-Head & Neck Surgery. 2023;150:39-48. doi:10.1001/jamaoto.2023.3756
- Kushida CA, Nichols DA, Holmes TH, et al. Effects of continuous positive airway pressure on neurocognitive function in obstructive sleep apnea patients: the APPLES study. Sleep. 2012;35:1593-1602. doi:10.5665/sleep.2226
- Schwartz M, Acosta L, Hung YL, Padilla M, Enciso R. Effects of CPAP and mandibular advancement device treatment in obstructive sleep apnea patients: a systematic review and meta-analysis. Sleep and Breathing. 2018;22:555-568. doi:10.1007/s11325-017-1590-6