Whole-body hyperthermia looks less like generic relaxation and more like a timed biological stressor: in a small depression substudy, a single session was followed by early Hamilton Depression Rating Scale improvement, heat-shock gene activation, and immune-process enrichment that included interleukin 6 production.
Research Highlights
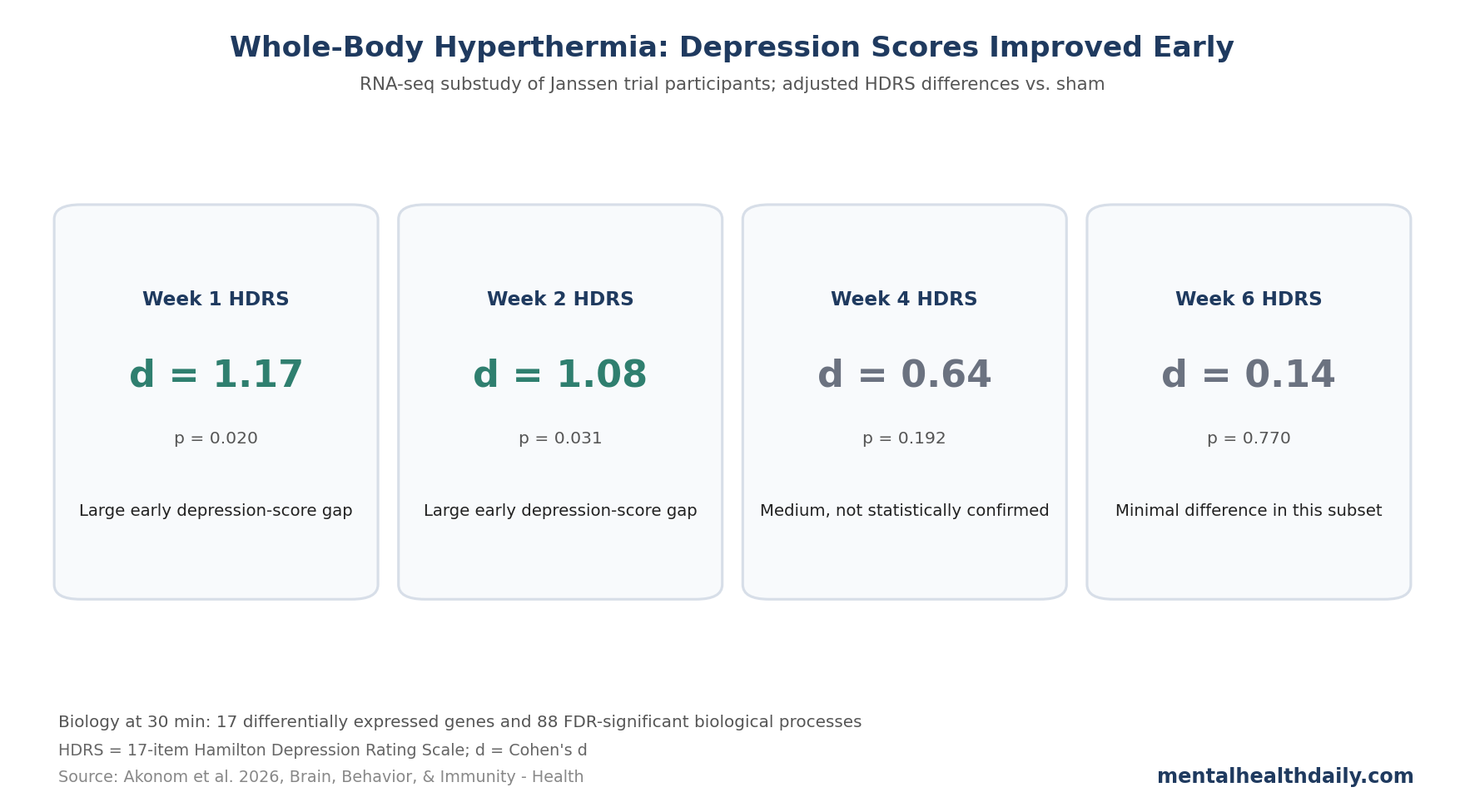
- Depression scores improved early: in the 18-person RNA sequencing substudy, whole-body hyperthermia showed large adjusted Hamilton Depression Rating Scale gaps vs. sham at week 1 (Cohen’s d = 1.17; p = 0.020) and week 2 (d = 1.08; p = 0.031).
- The effect faded in this tiny subset: the same substudy showed a medium, non-significant week 4 difference (d = 0.64; p = 0.192) and a minimal week 6 difference (d = 0.14; p = 0.770), so the strongest signal is early rather than definitively durable.
- Heat-shock biology was obvious: Akonom et al. identified 17 differentially expressed genes 30 min after treatment, with heat-shock protein genes making up 41% of the differentially expressed set.
- IL-6 remains the mechanistic hinge: gene set enrichment found 88 false-discovery-rate-significant biological processes, including interleukin 6 production, matching earlier plasma work from the same trial.
- Clinical translation is still narrow: this was a mechanistic substudy with 9 whole-body hyperthermia and 9 sham participants, not a stand-alone proof that sauna-like treatment is ready to replace antidepressants.
The calibrated interpretation is narrow: whole-body hyperthermia has a plausible antidepressant signal, but the 2026 RNA sequencing analysis mainly strengthens mechanism. It does not turn a 9-vs.-9 biomarker substudy into a definitive clinical trial.
Whole-body hyperthermia (WBH; controlled heating of the whole body) in this research protocol used infrared heat until core body temperature reached 38.5°C, roughly the lower boundary of a mild fever. The intervention is designed to engage fever-like heat biology instead of simple warmth or relaxation.
Week 1 and Week 2 HDRS Differences Were Large
Akonom et al. reanalyzed a subset from the earlier randomized, double-blind, sham-controlled whole-body hyperthermia trial in major depressive disorder (MDD). The parent trial enrolled adults with moderate-to-severe depression, defined by a Hamilton Depression Rating Scale (HDRS; clinician-rated depression severity) score > 16, and randomized them to active whole-body hyperthermia or a credible sham procedure.
The 2026 analysis focused on the 18 participants with whole-blood RNA sequencing (RNA-seq; a method for measuring gene-expression patterns) available 30 min after intervention: 9 received active heating and 9 received sham heating. For the depression-score analysis, 8 active and 9 sham participants had HDRS data.
- Baseline severity was similar: HDRS mean = 20.63 (SD 4.21) in the active group vs. 21.89 (SD 4.08) in sham.
- Week 1 favored active heating: adjusted HDRS mean = 14.68 vs. 20.52; p = 0.020; Cohen’s d = 1.17.
- Week 2 still favored active heating: adjusted HDRS mean = 13.25 vs. 19.04; p = 0.031; d = 1.08.
- Week 4 was directionally favorable but not confirmed: adjusted HDRS mean = 14.25 vs. 17.75; p = 0.192; d = 0.64.
- Week 6 was essentially flat in this subset: adjusted HDRS mean = 15.11 vs. 15.89; p = 0.770; d = 0.14.
The parent Janssen et al. trial reported a more sustained antidepressant pattern across 6 weeks. The RNA-seq substudy is smaller and easier to destabilize by missing data, baseline differences, and a few individual response trajectories. The early signal is biologically interesting, while the durability estimate remains imprecise.
30 Minutes After Heating, 17 Genes Were Differentially Expressed
The molecular result was not subtle. Using a false discovery rate (FDR; a multiple-comparison correction that limits expected false positives) threshold of q < 0.01, Akonom et al. identified 17 differentially expressed genes 30 min after whole-body hyperthermia relative to sham.
Heat-shock protein genes dominated the list. The strongest named signals included HSPA1A and HSPA1B, both heat-shock protein 70 family genes; HSPH1 and HSPA4, members of the broader heat-shock protein 70/110 system; and HSP90AA1 and HSP90AB1, heat-shock protein 90 family genes.
Plain-English read: the body reacted as if it had encountered a real cellular stressor. Heat-shock proteins act as molecular chaperones: they help stabilize, fold, and repair proteins when cells are under stress. That makes the transcriptomic result internally coherent with the intervention itself.
The study also found immune-linked genes and pathways, including C-type lectin domain containing 17A (CLEC17A), a surface protein tied to B-cell biology. The better frame is controlled perturbation: heat triggered a short-lived response involving protein-protection systems and immune signaling.
IL-6 Behaved Like a Context-Specific Heat Signal
Interleukin 6 (IL-6; a cytokine that can transmit inflammatory or anti-inflammatory signals depending on receptor context) is the awkward center of the whole-body hyperthermia story. In depression writing, IL-6 often appears as a bad inflammatory marker. Here, the story is more conditional.
Earlier plasma analyses from the Janssen trial reported that whole-body hyperthermia increased IL-6 30 min after treatment, without the same increase in canonical proinflammatory markers such as interleukin 1β and tumor necrosis factor. Flux et al. then linked larger post-treatment IL-6 increases with better antidepressant response across follow-up.
The 2026 RNA-seq analysis did not show a statistically significant IL-6 messenger RNA increase as a single gene. IL-6 mRNA had a base mean of 6.24, log2 fold change = 1.05, and unadjusted p = 0.1093. That is a directional 2.07-fold estimate, but it is not a confirmed single-gene hit.
The stronger RNA-seq evidence came from gene set enrichment analysis (GSEA; a pathway-level method that asks whether groups of related genes move together). Using an FDR q < 0.05 threshold, the researchers found 88 enriched biological processes, including interleukin 6 production.
Using the stricter family-wise error rate (FWER) threshold, 17 biological processes remained, including cellular response to heat, chaperone-mediated protein folding, positive regulation of response to cytokine stimulus, B-cell receptor signaling pathway, peptide antigen assembly with major histocompatibility complex protein complex, and type I interferon-related processes.
Interpretation: IL-6 is better treated as part of a heat-and-immune response network than as a single magic molecule. The plasma signal, the pathway signal, and the prior antidepressant-response association point in the same direction, but they still need replication in larger samples.
Heat Therapy and Exercise May Share a Controlled-Stress Logic
Whole-body hyperthermia overlaps conceptually with exercise, sauna exposure, and passive heating: all can raise temperature, mobilize cytokines, activate heat-shock proteins, and create a short biological challenge followed by adaptation. Their biology still diverges. Exercise adds muscle contraction, cardiorespiratory training, behavioral activation, and metabolic signaling that passive heating only partly reproduces.
Still, the shared IL-6 logic is useful. Exercise can transiently raise IL-6 from skeletal muscle without producing the same meaning as chronic inflammatory elevation. In the hyperthermia trial, the researchers argued that IL-6 may be acting through classical cis-signaling rather than proinflammatory trans-signaling. The clinical version is simple enough: acute, timed IL-6 spikes may differ from chronically elevated inflammatory tone.
That distinction prevents 2 common overcorrections. First, it avoids the claim that IL-6 is always bad in depression. Second, it avoids the wellness-world jump that any heat exposure is an antidepressant treatment. Mechanism is a map, not a prescription.
Limitations of This Hyperthermia RNA-Seq Analysis
The sample was tiny. The molecular analysis compared 9 active-treatment participants with 9 sham participants. Differential gene expression across thousands of genes in 18 people is hypothesis-generating even when the heat-shock signal is biologically coherent.
Bulk blood RNA-seq blurs cell types. Whole blood mixes immune-cell populations. A signal can reflect gene-expression changes inside cells, shifts in cell composition, or both. Single-cell RNA-seq would be more precise.
The clinical signal is not fully durable in this subset. HDRS differences were large at weeks 1 and 2, weaker at week 4, and minimal at week 6. The parent trial supports a broader antidepressant signal, but this mechanistic subset should not be oversold.
Sham heating was not inert. The sham condition used similar procedures and mild lower-extremity heating to preserve blinding. That improves trial credibility, but it may also shrink between-group differences if mild heating has biological effects.
Questions About Whole-Body Hyperthermia for Depression
Is whole-body hyperthermia the same as sauna use?
No. Sauna and passive heating may share some biology with whole-body hyperthermia, but this trial used a controlled infrared medical device, core-temperature monitoring, and a target of 38.5°C. Ordinary sauna exposure varies in temperature, duration, hydration, cooling, medical supervision, and achieved core temperature.
Does this mean heat therapy treats major depression?
The best answer is: possibly, for some patients, but the evidence is still early. The Janssen trial and related analyses justify more research; they do not justify replacing standard depression care with unsupervised heat exposure.
Why would IL-6 help if inflammation is linked to depression?
IL-6 is context-dependent. Chronic inflammatory elevation and a brief heat-induced IL-6 pulse are not biologically identical. The receptor pathway, timing, tissue source, and surrounding cytokine pattern change the meaning of the signal.
Who should be cautious with intense heat exposure?
People with cardiovascular disease, autonomic instability, pregnancy, heat intolerance, dehydration risk, fainting history, certain neurological conditions, or medications that impair sweating or blood-pressure regulation should not treat intense heat as harmless. The trial setting included medical screening and monitoring.
Whole-body hyperthermia is one of the more biologically interesting non-drug depression interventions because it produces measurable heat-shock and immune responses alongside the subjective experience of warmth. The clinical question is still open: which depressed patients benefit, how durable the benefit is, and whether simpler heat protocols can reproduce the medically monitored trial signal.
References
- Akonom TN, Allen MA, Begay TK, et al. Whole-blood transcriptomic response to whole-body hyperthermia in participants with major depressive disorder. Brain, Behavior, & Immunity – Health. 2026;54:101225. doi:10.1016/j.bbih.2026.101225
- Janssen CW, Lowry CA, Mehl MR, et al. Whole-body hyperthermia for the treatment of major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73:789-795. doi:10.1001/jamapsychiatry.2016.1031
- Flux MC, Smith DG, Allen JJB, et al. Association of plasma cytokines and antidepressant response following mild-intensity whole-body hyperthermia in major depressive disorder. Translational Psychiatry. 2023;13:132. doi:10.1038/s41398-023-02402-9
- Mac Giollabhui N, Lowry CA, Nyer M, et al. The antidepressant effect of whole-body hyperthermia is associated with the classical interleukin-6 signaling pathway. Brain, Behavior, and Immunity. 2024;119:801-806. doi:10.1016/j.bbi.2024.04.040
- Hanusch KU, Janssen CH, Billheimer D, et al. Whole-body hyperthermia for the treatment of major depression: associations with thermoregulatory cooling. American Journal of Psychiatry. 2013;170:802-804. doi:10.1176/appi.ajp.2013.12111395
- Hoekstra SP, Bishop NC, Leicht CA. Elevating body temperature to reduce low-grade inflammation: a welcome strategy for those unable to exercise? Exercise Immunology Review. 2020;26:42-55. PubMed:32139348