A 2026 medRxiv preprint built a reusable NeuroMark SPECT template from 2 large independent component analysis rounds, then applied it to 137 schizophrenia patients and 76 controls; after false-discovery-rate correction, 23 of 68 perfusion components differed between groups.1 Those data support infrastructure for comparing SPECT perfusion networks across datasets, with standalone schizophrenia diagnosis left outside the evidence.
Research Highlights
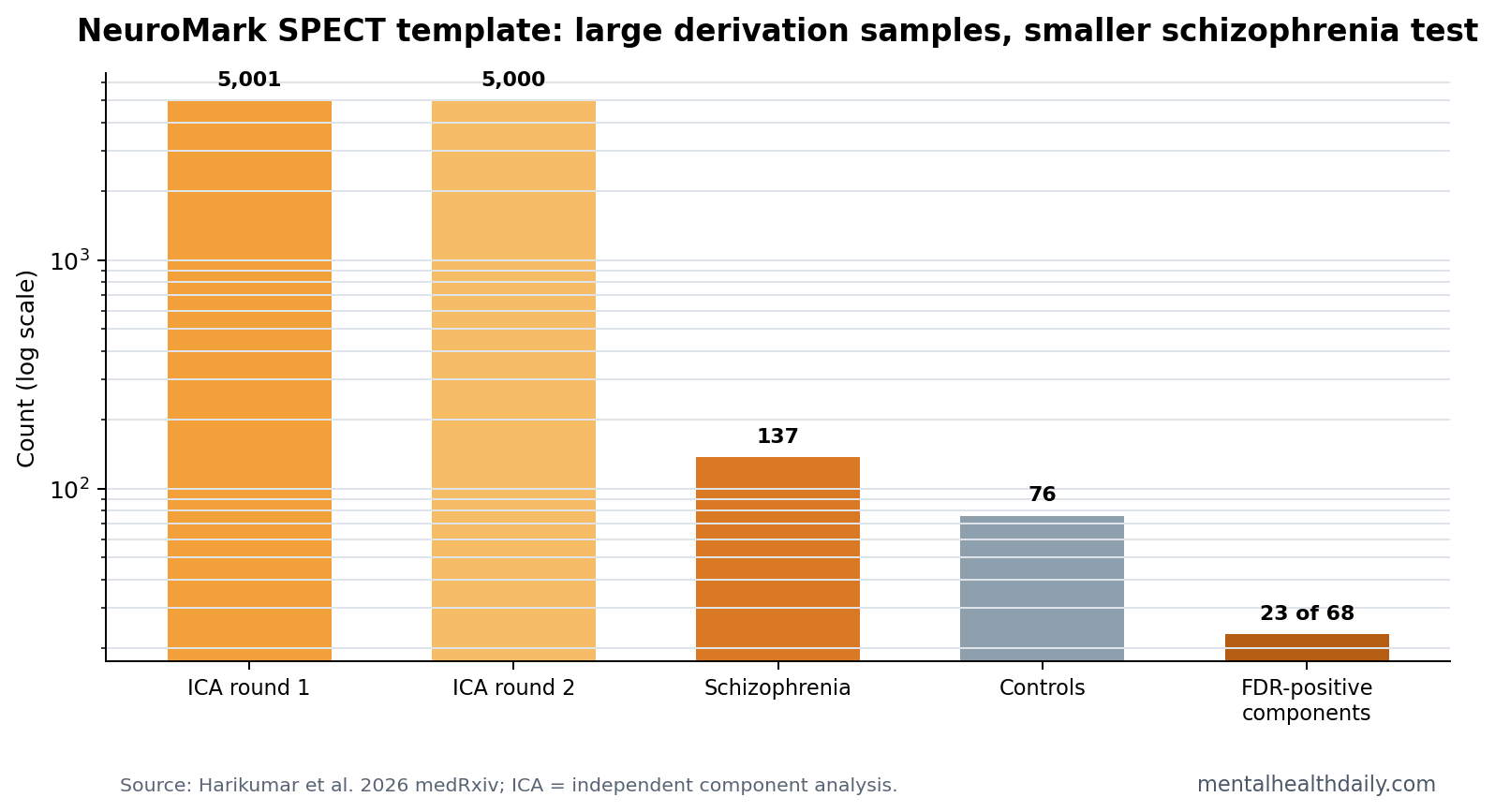
- Template scale was large: blind independent component analysis used 5,001 SPECT scans in round 1 and 5,000 scans in round 2, drawn from a 22,733-person depressed-clinic imaging pool.1
- Schizophrenia testing used 213 scans: spatially constrained ICA then applied the template to 137 schizophrenia patients and 76 controls.1
- Group differences were broad: 23 of 68 SPECT components differed between schizophrenia patients and controls after false-discovery-rate correction.1
- The method extends fMRI logic: NeuroMark-style templates have been used in fMRI to make network components correspond across participants and studies.2,3
- Clinical use remains limited: the 2026 preprint supports network-level research standardization, with individual diagnosis, treatment selection, and medication monitoring still untested.
Single photon emission computed tomography (SPECT) is a nuclear-imaging method that estimates regional cerebral blood flow by tracking a radiotracer. In psychiatry, the argument for SPECT has often been oversold at the individual-patient level. The stronger scientific use is narrower: if scans are already being collected, a stable network template can make resting perfusion patterns more reproducible across studies.
Independent component analysis (ICA) is a data-driven method that separates imaging data into spatial patterns that tend to vary together. Spatially constrained ICA adds a template prior so the same component label means roughly the same network across people. That is the NeuroMark move: less bespoke map-reading, more comparable network estimation.
Two 5,000-Scan ICA Rounds Built the SPECT Template
Harikumar et al. first ran blind ICA on 2 large random samples from an Amen Clinics SPECT database. Round 1 used 5,001 scans. Round 2 used 5,000 scans after 1 participant was removed for a quality-control problem involving mask registration.1
Why 2 rounds matter: an imaging template is weak if it only reflects the quirks of one sample. Repeating blind ICA in a second large sample asks whether similar perfusion covariance patterns reappear when the algorithm sees different people from the same broad imaging pool.
The source pool was not a community cohort. It came from 22,733 depressed individuals in a clinical imaging setting. That improves scale but limits generalizability. The template is a tool built from real clinical SPECT data, not a population atlas of ordinary brain perfusion.
23 of 68 Components Differed in the Schizophrenia Application
The independent test case used SPECT images from 137 schizophrenia patients and 76 controls. The researchers applied the new template with spatially constrained ICA, then compared component expression across the 2 groups.
Main result: 23 of 68 components were statistically different between schizophrenia patients and controls after false-discovery-rate correction.1 False-discovery-rate correction is a multiple-testing adjustment that reduces the chance of calling random component differences meaningful when many components are tested at once.
The result is notable because it shifts the claim away from isolated regional blobs. Schizophrenia was associated with altered expression across a distributed set of perfusion components, which fits the modern view of schizophrenia as a network-level brain disorder rather than a lesion in one location.
The stronger wording is still group-level. A component can differ on average and still be unusable for individual classification if patient and control distributions overlap. That is why the article’s useful claim is “23 FDR-corrected component differences,” not “SPECT diagnoses schizophrenia.” The former is what the paper tested; the latter would require sensitivity, specificity, and prospective validation that this preprint did not provide.
Template-Guided SPECT Is a Replication Tool, Not a Diagnostic Shortcut
NeuroMark has stronger precedent in functional MRI. Du et al. used template-guided ICA methods to create participant-specific functional-network estimates with stable component correspondence.2,3 Harikumar et al. adapted that logic to SPECT, where psychiatric interpretation has often been more heterogeneous.
- Research advantage: the same component framework can be applied across studies, making schizophrenia-control comparisons easier to replicate.
- Clinical boundary: diagnosis would require patient-level accuracy testing plus more than a group-level component difference.
- Quality-control need: SPECT templates still depend on scanner protocol, radiotracer handling, preprocessing, and the population used to build the template.
The Schizophrenia Signal Needs Careful Framing
The preprint gives schizophrenia imaging researchers a clearer SPECT network surface to test. It does not settle whether SPECT should be used routinely in schizophrenia clinics. The schizophrenia group was compared with controls in an exploratory imaging framework; the paper did not test diagnostic sensitivity, specificity, positive predictive value, medication-response prediction, relapse prediction, or cost-effectiveness.
Evidence-strength note: this was a preprint using a clinical imaging provider’s database. It can support replication of a network-analysis pipeline and motivate independent validation. It cannot support patient-facing claims that a scan can confirm schizophrenia, replace clinical interview, or choose antipsychotic treatment.
That distinction is especially important for SPECT because psychiatric SPECT marketing has sometimes run ahead of evidence. The data are interesting because they make perfusion-network research more standardized. The data are not a permission slip for broad diagnostic claims.
Where This Could Become Useful
A reusable SPECT template could help answer narrower questions that are hard to study when every group defines components differently:
- Subtype work: whether schizophrenia subgroups have reproducible perfusion-network patterns.
- Medication studies: whether antipsychotic exposure, dose, or symptom response shifts specific perfusion components.
- Cross-modality comparison: whether SPECT perfusion components align with fMRI connectivity, structural MRI, or cognitive phenotypes.
- Replication audits: whether reported schizophrenia perfusion patterns survive independent samples and standardized preprocessing.
The most defensible next step is not a bigger headline. It is independent replication with prespecified components, blinded group labels, and clinically interpretable endpoints.
What 23 Component Differences Can Show
The 23-component result is useful because it gives future schizophrenia SPECT work a more explicit target. Researchers can ask whether the same components separate schizophrenia from controls in another site, whether the pattern changes with symptom domains, and whether component expression tracks cognition, negative symptoms, or medication exposure.
Component-level replication: a reusable template lets one study’s “component 12” resemble another study’s “component 12.” That sounds technical, but it is the difference between a literature that accumulates and a literature that keeps redrawing maps from scratch. If the same perfusion components repeatedly separate schizophrenia groups, the signal becomes harder to dismiss as a local preprocessing artifact.
That still leaves the patient-level question separate. A between-group difference can exist even when many individual patients and controls overlap. Psychiatry imaging has seen this repeatedly: group averages can be robust while individual classification remains too noisy for routine care.
Validation Should Move Toward Prespecified Clinical Questions
The next validation step should be designed around a question a clinic or trial would actually use. Schizophrenia is heterogeneous, so a broad case-control contrast may be less useful than narrower tests:
- Negative symptoms: whether perfusion components track low motivation, blunted affect, or social withdrawal.
- Cognition: whether components align with working memory, processing speed, or executive function.
- Medication exposure: whether antipsychotic dose or treatment duration explains part of the perfusion pattern.
- Longitudinal stability: whether the same person’s component expression is stable enough to use in follow-up studies.
Those endpoints would make the template more valuable than a diagnostic slogan. The best use of NeuroMark SPECT may be as a shared measurement system for research programs that already have careful clinical phenotyping.
A strong replication paper would also report ordinary clinical overlap: how many schizophrenia patients fall inside the control range for each component, how medication status changes the estimates, and how stable the components remain when scans are repeated. Those details decide whether a promising network template becomes a practical research instrument.
Medication is the biggest immediate confounder to name plainly. Antipsychotic exposure, illness duration, smoking, sleep, caffeine, movement during scanning, and comorbid depression can all shift perfusion. A template can standardize the measurement surface, but it cannot remove those clinical differences by itself.
That is why the 23 of 68 result should be treated as a target list, not an endpoint.1 Future studies need to ask whether those same components survive scanner-site differences, blinded preprocessing, matched medication strata, and symptom-domain models. If they do, SPECT becomes more useful for schizophrenia research. If they do not, the template still helps by showing which claims fail replication.
Questions About NeuroMark SPECT and Schizophrenia
Does this study show that SPECT diagnoses schizophrenia?
No. It found group-level differences in 23 of 68 perfusion components. Diagnosis would require patient-level accuracy testing against appropriate clinical and non-clinical comparison groups.
Why use a template instead of reading each scan manually?
A template gives the analysis stable component labels. That makes it easier to compare results across people and studies instead of relying on subjective regional interpretation.
What makes this result preliminary?
The paper is a medRxiv preprint, the derivation data came from a clinical imaging provider, and the schizophrenia analysis tested group differences rather than clinical decision rules.
References
- Harikumar A, Baker B, Amen D, Keator D, Calhoun VD. A replicable NeuroMark template for whole-brain SPECT reveals data-driven perfusion networks and their alterations in schizophrenia. medRxiv. 2026. doi:10.64898/2026.04.08.26349985
- Du Y, Fu Z, Sui J, et al. NeuroMark: an automated and adaptive ICA based pipeline to identify reproducible fMRI markers of brain disorders. NeuroImage: Clinical. 2020. doi:10.1016/j.nicl.2020.102375
- Du Y, Pearlson GD, Lin D, et al. Identifying dynamic functional connectivity biomarkers using GIG-ICA. NeuroImage. 2015. doi:10.1016/j.neuroimage.2015.07.054
- Harikumar A, et al. SPECT-based psychiatric neuroimaging analysis before the NeuroMark SPECT template. Journal of Psychiatry & Neuroscience. doi:10.52294/001c.138726