A 2026 BRFSS analysis involving 4,071 U.S. adults who used cannabis and either smoked cigarettes, vaped nicotine, or did both found a strong modality match: people who vaped tobacco were much more likely to vape cannabis than to smoke cannabis.1 For addiction and harm-reduction assessment, the pattern is a route-specific risk signal because smoking, vaping, and mixed routes change lung exposure, dependence maintenance, and cessation planning.
Research Highlights
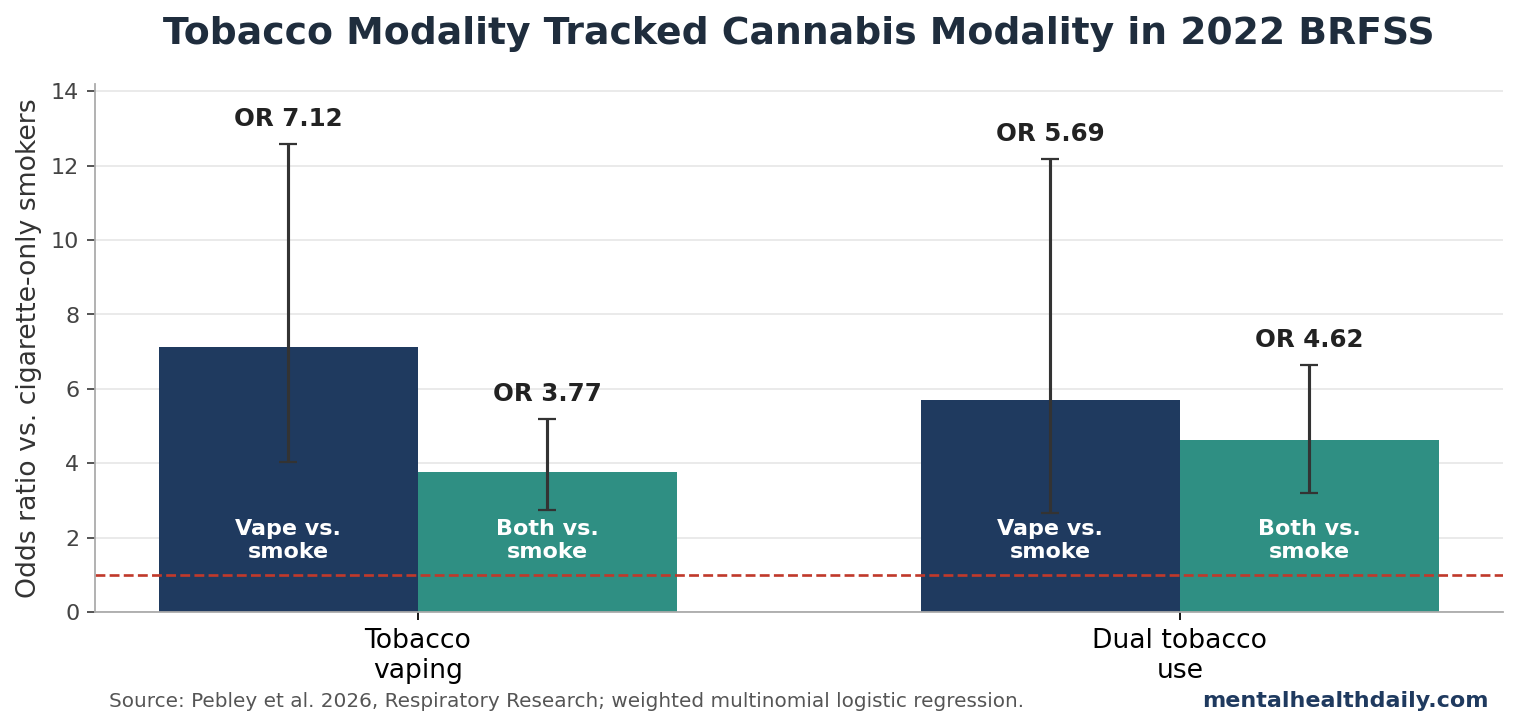
- Vaping clustered across products: among adults who vaped tobacco, the odds favored vaping cannabis over smoking cannabis 7.12x more strongly than among adults who only smoked cigarettes.1
- Dual tobacco users also leaned toward cannabis vaping: among adults who both smoked cigarettes and vaped tobacco, the odds favored vaping cannabis over smoking cannabis 5.69x more strongly than among cigarette-only smokers.1
- Most cannabis co-users still smoked cannabis: weighted BRFSS estimates put cannabis smoking only at 63.0%, cannabis vaping only at 4.7%, and both cannabis smoking plus vaping at 32.3%.1
- Combustion remains the practical risk marker: smoking cannabis exposes users to combustion products, while vaping cannabis may reduce some toxicant exposure but is not risk-free and has less long-term evidence than cigarette smoking.5
- The evidence is associative: this cross-sectional survey analysis cannot determine whether nicotine vaping leads to cannabis vaping, cannabis vaping leads to nicotine vaping, or a third factor drives both behaviors.1
The main clinical and public-health implication is assessment precision: knowing whether an adult uses cannabis or tobacco is useful, but knowing whether each product is smoked, vaped, or used both ways adds route-specific information for respiratory exposure, dependence patterns, cessation planning, and harm-reduction advice.
2022 BRFSS Data Separated Smoking From Vaping
Pebley et al. analyzed the 2022 Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative U.S. adult survey. The researchers focused on 4,071 adults who reported past-30-day cannabis use and current cigarette smoking, current e-cigarette use, or both.1
BRFSS is a surveillance dataset rather than a clinic trial, so it captures real-world use patterns at scale while depending on self-report and leaving product timing, dose, potency, and individual-level changes over time unresolved.
The analysis sorted both tobacco use and cannabis use by route. Tobacco use was classified into 3 groups:
- Cigarette smoking only: adults who currently smoked cigarettes and did not currently vape nicotine.
- Tobacco vaping only: adults who currently used e-cigarettes and did not currently smoke cigarettes.
- Dual tobacco use: adults who currently smoked cigarettes and currently vaped nicotine.
Cannabis use was also classified into 3 route groups:
- Cannabis smoking only: adults who smoked cannabis and did not vape cannabis.
- Cannabis vaping only: adults who vaped cannabis and did not smoke cannabis.
- Both smoking and vaping cannabis: adults who used cannabis through both routes.
Cannabis and tobacco co-use is already common, but route-specific co-use gives a more precise respiratory-risk estimate than a yes-or-no substance checklist because exposure depends heavily on whether each product is combusted, vaporized, or mixed across routes.
Tobacco Vaping Predicted Cannabis Vaping More Than Cannabis Smoking
The largest estimate came from the comparison between tobacco vaping and cigarette-only smoking. After adjustment for race, sex, and education, adults who vaped tobacco had higher odds of vaping cannabis rather than smoking cannabis: odds ratio (OR) 7.12, 95% confidence interval (CI) 4.03 to 12.58.1
An odds ratio compares the odds of one outcome between groups. A 95% confidence interval gives the range of values most compatible with the data under the model; because the full interval sits above 1.0, the association was statistically clear in this analysis.
Dual tobacco use showed the same direction. Adults who both smoked cigarettes and vaped nicotine had OR 5.69, 95% CI 2.66 to 12.19, for vaping cannabis rather than smoking cannabis, compared with cigarette-only smokers.1
The combined cannabis smoking-plus-vaping pattern also tracked tobacco vaping:
- Tobacco vaping only: OR 3.77, 95% CI 2.73 to 5.19, for smoking plus vaping cannabis rather than smoking cannabis only.
- Dual tobacco use: OR 4.62, 95% CI 3.21 to 6.64, for smoking plus vaping cannabis rather than smoking cannabis only.
- Tobacco vaping vs. dual cannabis use: adults who vaped tobacco had lower odds of smoking plus vaping cannabis than vaping cannabis only, OR 0.53, 95% CI 0.29 to 0.97.
The last estimate compares 2 cannabis-route outcomes among adults who vaped tobacco: vaping cannabis only vs. both smoking and vaping cannabis. The OR below 1.0 means tobacco-vaping-only adults were less likely to fall into the dual cannabis-route group than the cannabis-vaping-only group.
63.0% of Cannabis Co-Users Still Smoked Cannabis Only
The odds ratios are large, but the base-rate pattern keeps the finding grounded. In weighted estimates, cannabis smoking was still the most common route among adults who used cannabis and currently smoked or vaped tobacco.1
- Smoke cannabis only: 63.0% of the weighted sample.
- Vape cannabis only: 4.7% of the weighted sample.
- Smoke and vape cannabis: 32.3% of the weighted sample.
Tobacco use was also mixed. In the overall weighted sample, 52.3% smoked cigarettes only, 33.3% vaped tobacco only, and 14.4% used both cigarettes and e-cigarettes.1
Those base rates prevent a common overread: cannabis vaping had not overtaken cannabis smoking among adult co-users in this dataset, but tobacco vaping still identified a subgroup with a sharply different cannabis-use pattern than cigarette-only smokers.
Age was visible descriptively but not modeled. Adults aged 18 to 24 accounted for 33.4% of the weighted smoke-plus-vape cannabis group but only 17.0% of the cannabis-smoking-only group. The researchers did not include age in the regression model because the model became unstable, so age should be treated as an important descriptive signal rather than an adjusted causal explanation.
Education and race also tracked modality. Adults with more than high school education had higher odds of vaping cannabis rather than smoking cannabis, OR 2.51, 95% CI 1.60 to 3.94.
White non-Hispanic adults had higher odds of vaping cannabis rather than smoking cannabis, OR 1.87, 95% CI 1.11 to 3.15, and higher odds of smoking plus vaping cannabis rather than smoking cannabis only, OR 1.58, 95% CI 1.18 to 2.09.1
Respiratory Risk Depends on Combustion, Product Chemistry, and Frequency
Combustion is the clearest risk driver for respiratory damage in this co-use pattern because cigarette smoking remains the leading preventable cause of death in the United States, and smoking cannabis also exposes users to combustion products that can irritate or injure the respiratory system.1
Vaping has a more complicated evidence profile. For nicotine, randomized and review evidence supports e-cigarettes as a smoking-cessation aid for some adults who smoke cigarettes, and toxicant exposure is generally lower than with combustible cigarettes.6
Lower exposure still leaves meaningful exposure because e-cigarette aerosols can deliver nicotine, irritants, and other toxicants, and long-term respiratory data remain incomplete.7
Cannabis vaping has a thinner long-term evidence base than nicotine vaping. Chaiton et al. reviewed respiratory and cardiovascular differences between smoking and vaping cannabis and argued that vaping cannabis may reduce some combustion-related exposure while still carrying product-specific risks, especially with concentrates, oils, additives, and device variability.5
Modality assessment needs more than a moralized “smoking bad, vaping good” frame because the clinically relevant questions are concrete and product-specific:
- Does the person combust cannabis, tobacco, or both?
- Does the person vape nicotine, cannabis, or both?
- Are cannabis products flower, concentrates, oils, or mixed routes?
- How often are products used, and are they used together in the same session?
- Is the goal cessation, harm reduction, symptom relief, or intoxication?
Those answers can change advice because a person who smokes cigarettes and smokes cannabis faces a different respiratory profile than a person who vapes nicotine and vapes cannabis, and both differ from a person who alternates cigarettes, e-cigarettes, smoked cannabis, and cannabis vapes.
Cross-Sectional Data Cannot Explain the Sequence
This analysis is cross-sectional, meaning exposure and outcome were measured at one time point, so it can show that tobacco vaping and cannabis vaping clustered together in 2022 BRFSS but cannot identify the order in which the behaviors developed.
Several explanations remain possible:
- Nicotine vaping could normalize cannabis vaping: device familiarity, social norms, and access may make cannabis vaping easier to adopt.
- Cannabis vaping could normalize nicotine vaping: cannabis device use could make e-cigarette use feel more familiar or less risky.
- A shared third factor could drive both: age, risk tolerance, cannabis legalization, local retail access, product marketing, or peer networks may push both routes together.
- Health concerns could shift routes: some users may move away from combustion because of cough, asthma, clinician advice, or a general preference for lower-odor products.
The paper also could not model age, income, cannabis legalization status, product potency, frequency of use, or sequence of product initiation. Missing data were low at 2.5%, but self-report remains vulnerable to underreporting, especially where cannabis use is illegal or stigmatized.1
Evidence-strength note: this is a nationally representative survey analysis with a clear modality signal, not a longitudinal causal study. It supports better screening questions and stronger hypotheses for follow-up research; it does not prove that a change in tobacco smoking or vaping will automatically change cannabis smoking or vaping.
Harm Reduction Should Ask About Routes and Substances
McClure et al. emphasized that tobacco and cannabis co-use complicates respiratory health and tobacco cessation because the products can reinforce each other behaviorally and pharmacologically.4 A patient may want to quit cigarettes while continuing cannabis, or may view cannabis as medical and tobacco as the only target. The route of cannabis use can then determine whether combustion exposure actually falls.
A more useful intake starts with “Do you use cannabis?” and then separates route, nicotine co-use, and session pattern:
- Cannabis route: smoked flower, blunts, joints, pipes, bongs, vaporizers, concentrates, edibles, tinctures, or mixed use.
- Nicotine route: cigarettes, e-cigarettes, nicotine pouches, smokeless tobacco, or dual use.
- Session pattern: separate use, same-day use, same-session use, or mixing cannabis with tobacco.
- Change target: quit nicotine, reduce combustion, reduce cannabis intoxication, manage withdrawal, or lower respiratory symptoms.
For some adults, reducing combustion exposure may be a realistic intermediate target. For others, dual use may keep nicotine dependence active while adding cannabis-related risks. The assessment has to separate route, frequency, dependence, and purpose.
Questions About Cannabis and Tobacco Co-Use
Did this study show that tobacco vaping causes cannabis vaping?
No. The analysis measured smoking and vaping status for tobacco and cannabis at one time point. It found a strong association, but it cannot establish the order of adoption or rule out shared causes.
What was the strongest result?
Among adults who vaped tobacco, the odds favored vaping cannabis over smoking cannabis 7.12x more strongly than among adults who only smoked cigarettes. Among adults who both smoked and vaped tobacco, the odds favored vaping cannabis over smoking cannabis 5.69x more strongly than among cigarette-only smokers.
Was vaping the most common way people used cannabis?
No. Among adults who used cannabis and currently smoked or vaped tobacco, weighted estimates showed 63.0% smoked cannabis only, 4.7% vaped cannabis only, and 32.3% both smoked and vaped cannabis.
Is cannabis vaping safer than smoking cannabis?
Vaping cannabis may reduce some combustion-related exposure, but product chemistry, concentrate potency, additives, device temperature, frequency, and underlying lung disease can all change the dose of airway irritants, the likelihood of acute lung injury, and the expected respiratory risk.
What should clinicians or harm-reduction workers ask?
Ask about the route for each product. A person who smokes cigarettes and vapes cannabis is not the same risk profile as a person who vapes nicotine and smokes cannabis, even if both count as cannabis-tobacco co-use.
References
- Pebley K, McClure EA, Chen AA, Toll BA, Rojewski AM. A cross-sectional analysis of Behavioral Risk Factor Surveillance System (BRFSS) data to determine if tobacco and cannabis methods of administration are likely to be consistent across products. Respiratory Research. 2026;27:173. doi:10.1186/s12931-026-03638-x
- Rubenstein D, McClernon FJ, Pacek LR. Trends in cannabis and tobacco co-use in the United States, 2002–2021. Addictive Behaviors. 2024;158:108129. doi:10.1016/j.addbeh.2024.108129
- Schauer GL, Berg CJ, Kegler MC, Donovan DM, Windle M. Differences in tobacco product use among past-month adult marijuana users and nonusers: findings from the 2003–2012 National Survey on Drug Use and Health. Nicotine & Tobacco Research. 2015;18(3):281–288. doi:10.1093/ntr/ntv093
- McClure EA, Piper ME, Crotty Alexander LE, Burnham EL, Freeman TP, Galiatsatos P, et al. Effects of inhaled tobacco and cannabis co-use on respiratory health and tobacco cessation: an official American Thoracic Society research statement. American Journal of Respiratory and Critical Care Medicine. 2025;211(11):2021–2042. doi:10.1164/rccm.202507-1792st
- Chaiton M, Kundu A, Nathwani AA. Health impacts of cannabis: focus on smoking vs. vaping effects on the respiratory and cardiovascular systems. Current Opinion in Pulmonary Medicine. 2026;32(2):93–97. doi:10.1097/mcp.0000000000001239
- Lindson N, Butler AR, McRobbie H, Bullen C, Hajek P, Wu AD, et al. Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews. 2025. doi:10.1002/14651858.cd010216.pub8
- Gotts JE, Jordt SE, McConnell R, Tarran R. What are the respiratory effects of e-cigarettes? BMJ. 2019;366. doi:10.1136/bmj.l5275