A 2026 review argues that neurovascular-unit dysfunction may precede amyloid-beta generation in Alzheimer’s disease and then synergize with amyloid deposition, tau pathology, inflammation, and neuronal loss.1 The model is vascular biology plus amyloid biology: blood vessels, barrier integrity, and amyloid deposition can amplify each other early enough to affect dementia risk and progression.
Research Highlights
- Early timing is the headline: the 2026 review describes decreased cerebral blood flow before amyloid-beta generation as a reason neurovascular dysfunction may be upstream in Alzheimer’s disease.
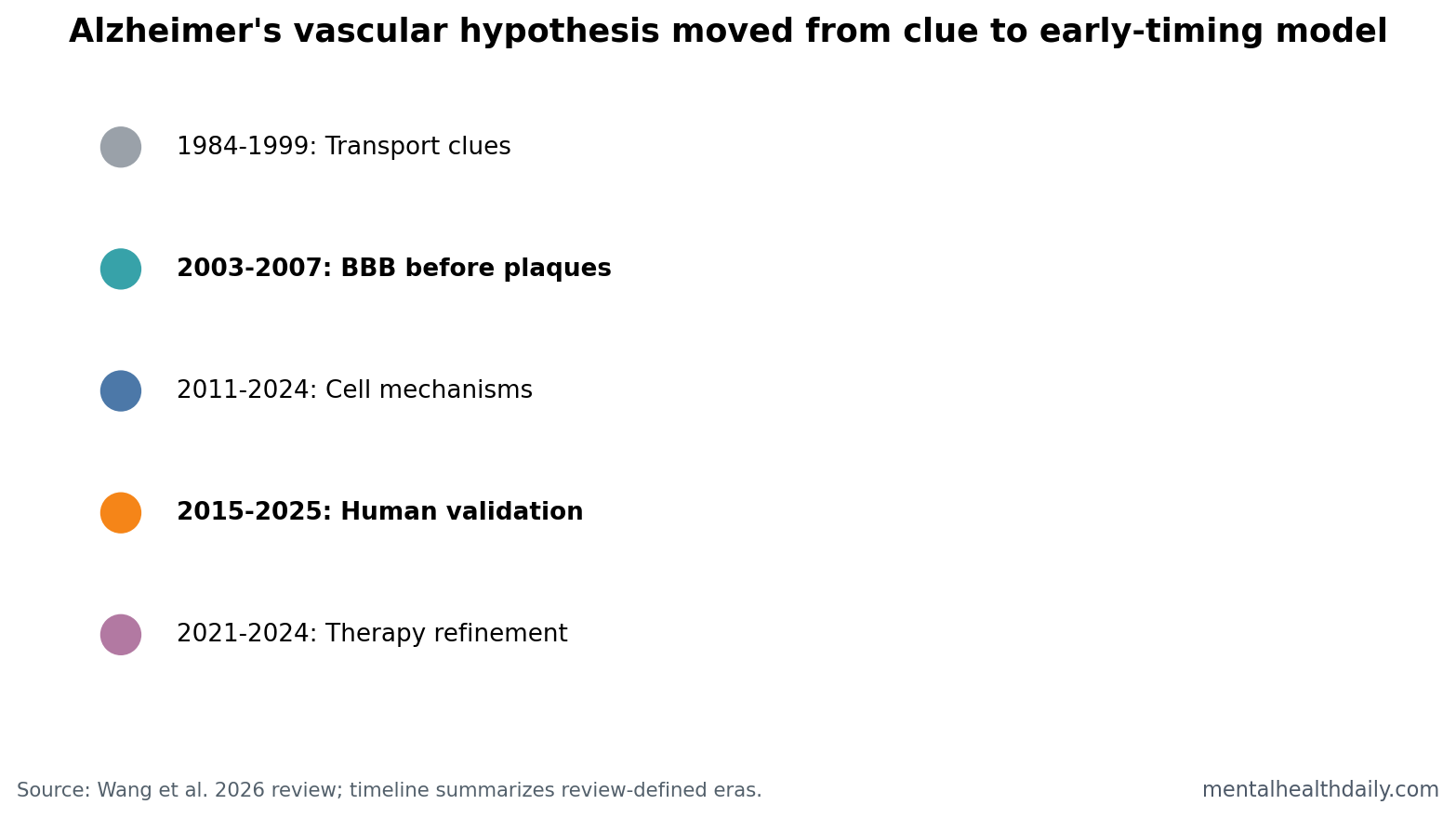
- 5 research eras changed the model: the review traces vascular clues from 1984-1999 through BBB-before-plaque evidence in 2003-2007 and human validation in 2015-2025.
- The neurovascular unit has 6 failure points: endothelial tight junctions, pericytes, astrocytes, microglia, neurons, and blood-brain barrier transport can all contribute.
- 2 amyloid antibodies do not erase vascular biology: lecanemab and donanemab showed modest clinical efficacy, while vascular repair may still shape treatment response and risk.
- New tools may refine patient subtypes: 3-dimensional NVU organoids, spatial transcriptomics, and machine learning could separate vascular-heavy Alzheimer’s patterns from other pathways.
Neurovascular unit means the working partnership among brain endothelial cells, pericytes, astrocytes, microglia, neurons, and basement membranes. It controls blood-brain barrier integrity, cerebral blood flow, nutrient delivery, waste clearance, and inflammatory signaling.
Cerebral blood flow is the amount of blood reaching brain tissue. If flow falls before amyloid-beta generation or before cognitive symptoms, vascular dysfunction becomes a possible driver of disease biology rather than only a late complication.
Early Blood-Brain Barrier Failure Challenges Amyloid-Only Timing
The review keeps amyloid-beta and tau in the frame. Amyloid precursor protein cleavage, amyloid-beta aggregation, tau pathology, neuroinflammation, synaptic loss, and cognitive decline remain central Alzheimer’s biology. The update is temporal: vascular dysfunction can appear early enough to affect that cascade.1
Wang et al. point to several early vascular signals: blood-brain barrier alterations before clinical onset in models, population evidence linking cerebral hypoperfusion with prodromal dementia, and human neuroimaging work identifying blood-brain barrier breakdown as an early biomarker of cognitive decline.
Clinical translation: a patient with Alzheimer’s biology may not have one clean pathway. Vascular injury, amyloid deposition, tau spread, inflammation, and metabolic stress can move together.
5 Eras Moved Vascular Dysfunction From Bystander to Driver
Wang et al. organize the vascular hypothesis into 5 chronological eras. The first era, 1984-1999, identified blood-brain barrier transport systems and vascular iron transport abnormalities near amyloid plaques, but vascular pathology was still not treated as core Alzheimer’s causation.
The second era, 2003-2007, shifted the model by showing blood-brain barrier breakdown before plaque formation and linking reduced cerebral blood flow with cognitive impairment. That is the key timing claim: vessels can fail before amyloid plaques dominate the explanation.
The third era, 2011-2024, focused on mechanisms such as pathological angiogenesis, pericyte dysfunction, endothelial failure, HIF1α-VEGFA signaling problems, vascular inflammation, and senescence. The fourth era, 2015-2025, brought living-human imaging and biomarker validation. The fifth era, 2021-2024, focused on therapeutic refinement and vascular-targeting experiments.
Endothelial Cells, Pericytes, and Astrocytes Are Not Background Support
Endothelial cells line brain blood vessels and form tight junctions that restrict leakage. If those junctions loosen, proteins, inflammatory signals, and other blood-derived factors can enter brain tissue more easily.
Pericytes wrap small vessels and help control blood-brain barrier permeability, blood-flow regulation, and amyloid-beta clearance. Pericyte degeneration can therefore connect vascular injury with protein-clearance failure.
Astrocytes place endfeet around blood vessels and help regulate neurovascular coupling, the process that increases local blood flow when neurons become active. If astrocyte signaling becomes reactive or disorganized, vascular responses may no longer match metabolic demand.
These cells are active control points. They determine whether neurons receive oxygen and glucose, whether waste products leave, whether inflammation stays contained, and whether amyloid-beta clearance keeps pace with production.
Amyloid and Vessels Can Reinforce Each Other
The most useful model is bidirectional. Amyloid pathology can damage vessels through cerebral amyloid angiopathy, abnormal angiogenesis, endothelial dysfunction, and inflammatory signaling. Vascular dysfunction can then worsen amyloid clearance, reduce perfusion, and increase barrier leakage.
That loop helps explain why amyloid-removal treatments can show modest benefit without solving the entire disease. Lecanemab and donanemab improved some clinical outcomes in early Alzheimer’s disease, but vascular integrity may still shape who benefits, who declines, and who develops amyloid-related imaging abnormalities.2
Calibration: vascular dysfunction does not disprove amyloid. It makes an amyloid-only treatment frame too narrow for many patients.
Organoids and Spatial Transcriptomics Could Separate Vascular Subtypes
Organoids are 3-dimensional cell models grown to mimic parts of tissue organization. Neurovascular-unit organoids could let researchers test endothelial, pericyte, astrocyte, immune, and neuronal interactions in controlled systems.
Spatial transcriptomics measures gene expression while preserving where cells sit in tissue. That matters because Alzheimer’s disease is spatial: plaques, vessels, inflammatory cells, and vulnerable neurons are not randomly distributed.
Machine learning may help integrate these layers, but only if the data are biologically grounded. A model that combines blood-brain barrier imaging, cerebrospinal-fluid vascular markers, amyloid/tau biomarkers, and clinical trajectory could identify vascular-heavy Alzheimer’s subtypes more usefully than a single biomarker label.
Evidence Strength: Review Synthesis, Not a New Trial
Evidence-strength note: Wang et al. wrote a review. It synthesizes animal, pathology, imaging, biomarker, organoid, transcriptomic, and therapeutic literature. It does not newly enroll patients or test a vascular intervention.
The temporal claim is strongest when multiple evidence types line up: barrier breakdown before plaques in experimental systems, hypoperfusion before dementia in human cohorts, early blood-brain barrier leakage on imaging, and vascular markers that track tau and cognitive decline. Any one layer is incomplete; the synthesis becomes more persuasive because the layers converge.
Still, Alzheimer’s disease is heterogeneous. Some patients may have dominant amyloid/tau trajectories, some may have vascular-heavy trajectories, and many may have mixed biology. A vascular model should improve stratification, not replace the rest of Alzheimer’s research.
Vascular Risk Management Fits the Model, But Does Not Prove It
The review’s mechanism is compatible with ordinary clinical advice: treat hypertension, diabetes, sleep apnea, smoking, atrial fibrillation, kidney disease, and sedentary behavior because vascular health affects brain health. Those steps are already justified without needing a new Alzheimer’s theory.
What changes: neurovascular-unit biology gives those risk factors a more direct mechanistic bridge to amyloid clearance, blood-brain barrier leakage, inflammatory signaling, and neuronal energy supply. A blood-pressure number can shape the microvascular environment in which amyloid and tau pathology unfold over decades.
What does not change: no patient should hear that vascular care replaces amyloid/tau diagnosis, cognitive evaluation, medication review, sleep workup, or neurologic follow-up. The stronger inference is layered risk management. Vascular repair may make the brain less permissive to degeneration, but it is not a standalone cure.
Future trials may need to stratify patients by vascular leakage, perfusion, pericyte markers, amyloid burden, tau burden, APOE status, and inflammation instead of treating Alzheimer’s disease as one uniform biological state.
What a Vascular-Heavy Alzheimer’s Trial Would Need
A clean trial would first identify people with evidence of blood-brain barrier leakage, impaired cerebral blood flow, vascular inflammation, or pericyte-related biomarker change before testing a vessel-targeting intervention.
Baseline biology: amyloid and tau status would still matter. A vascular-heavy patient with amyloid positivity may need a different strategy from a vascular-heavy patient without amyloid pathology. Mixing those groups could hide a true effect or create a false one.
Outcome selection: cognition alone may be too slow or noisy for early proof. Trials may need intermediate markers such as blood-brain barrier permeability, perfusion, cerebrospinal-fluid vascular injury markers, amyloid clearance markers, and tau progression, followed by longer cognitive endpoints.
Safety boundary: vascular manipulation in older adults can affect blood pressure, bleeding risk, edema, and perfusion. Any vascular-targeting Alzheimer’s strategy needs safety evidence as strong as its biomarker rationale.
Combination logic: the most realistic future may pair vascular-risk management with amyloid or tau-directed therapy, not force a choice between them. If blood-brain barrier failure worsens amyloid clearance or inflammation, vascular stabilization could become a response modifier even when amyloid remains the named target.
That combined design would match the review’s central claim: Alzheimer’s progression can reflect interacting vascular, amyloid, tau, inflammatory, and metabolic systems.
Trial timing would matter as much as target choice. A vascular intervention may be most informative before advanced neuronal loss, when barrier repair, perfusion improvement, or inflammatory dampening still has tissue to protect.
Patient selection should therefore include vascular imaging or fluid markers rather than assuming every Alzheimer’s patient has the same neurovascular contribution. Otherwise, a targeted intervention could be diluted across biologically mismatched participants.
Questions About Alzheimer’s Vascular Dysfunction
Does this mean Alzheimer’s disease is vascular dementia?
No. The argument is that neurovascular dysfunction can contribute to Alzheimer’s pathogenesis and may appear early. It does not collapse Alzheimer’s disease into ordinary vascular dementia.
Does fixing blood flow prevent Alzheimer’s disease?
Not proven. Blood-pressure control, exercise, sleep treatment, and vascular-risk management are sensible brain-health strategies, but this review does not prove prevention through vascular repair.
Why does timing matter?
If barrier and blood-flow problems occur before or alongside amyloid changes, they may be treatment targets before extensive neuronal loss. Late vascular repair may be less effective.
References
- Wang L, Han L, Liu S. Dysfunction of the neurovascular unit as a temporal driver in Alzheimer’s pathogenesis. Translational Neurodegeneration. 2026;15:17. https://doi.org/10.1186/s40035-026-00548-2
- PubMed search: lecanemab donanemab vascular blood-brain barrier Alzheimer’s disease. https://pubmed.ncbi.nlm.nih.gov/?term=lecanemab+donanemab+vascular+blood-brain+barrier+Alzheimer%27s+disease
- PubMed search: blood-brain barrier breakdown early Alzheimer’s disease cognitive decline. https://pubmed.ncbi.nlm.nih.gov/?term=blood-brain+barrier+breakdown+early+Alzheimer%27s+disease+cognitive+decline
- PubMed search: cerebral blood flow hypoperfusion prodromal dementia Alzheimer’s. https://pubmed.ncbi.nlm.nih.gov/?term=cerebral+blood+flow+hypoperfusion+prodromal+dementia+Alzheimer%27s