A 2026 PRO-ACT analysis of amyotrophic lateral sclerosis (ALS) trial data found a signal that ordinary ALSFRS total-score slopes cannot even express: Shannon entropy trajectories diverged between pooled active and placebo arms, including a 5-month delay in peak Fine Motor distributional spread for active-arm patients.1
Research Highlights
- Entropy found an endpoint-level signal: Rodriguez analyzed 7,512 PRO-ACT patients with treatment labels and found total integrated absolute divergence of 4.476, p < 0.001, across 4 ALSFRS domains.1
- Fine Motor timing separated the arms: placebo entropy peaked at month 8, while active-arm entropy peaked at month 13, a 5-month delay in maximal population spread across Fine Motor function levels.1
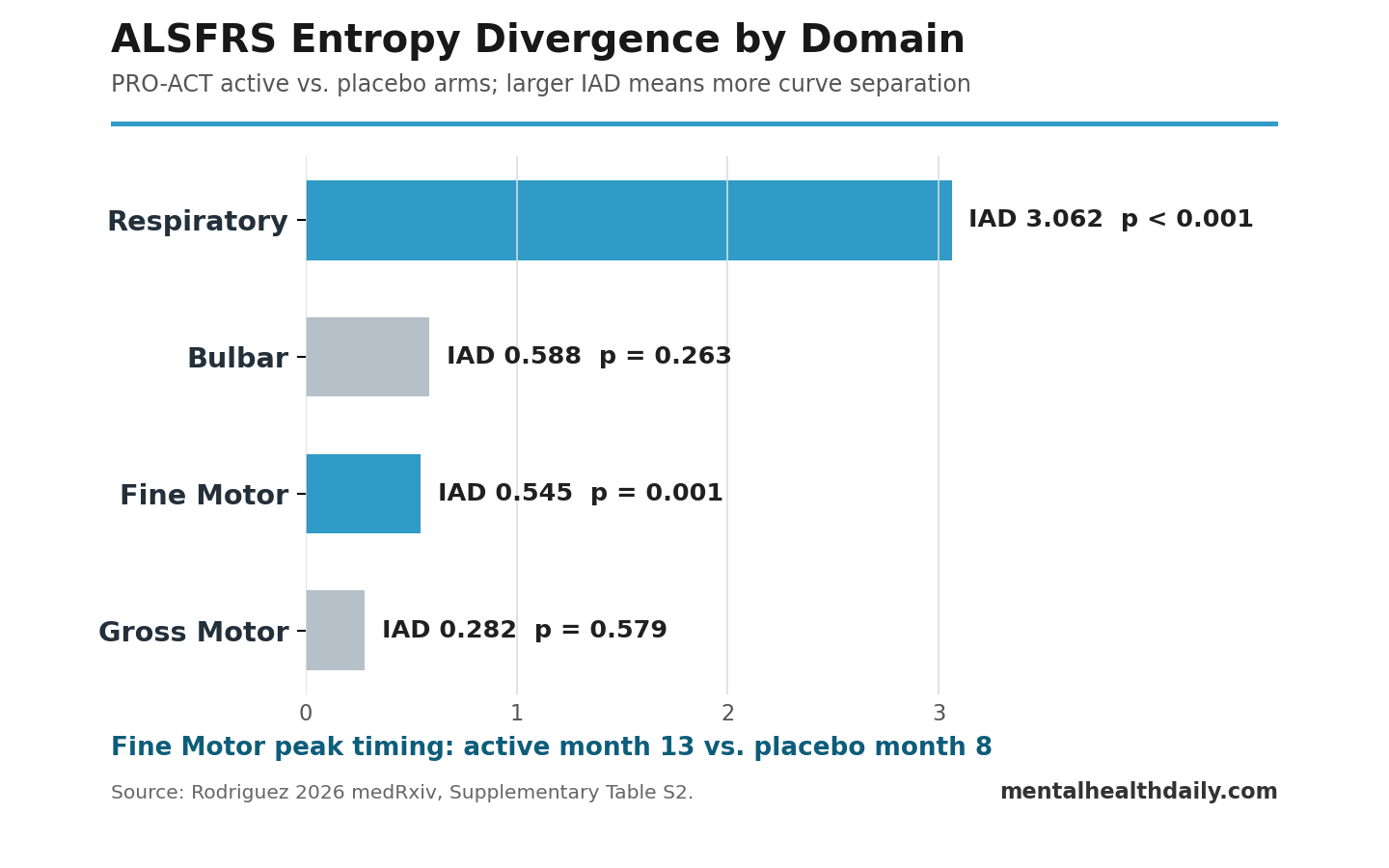
- Respiratory divergence dominated the total: Respiratory integrated absolute divergence was 3.062, p < 0.001; Fine Motor was also significant at 0.545, p = 0.001.1
- The finding is not a drug-approval result: PRO-ACT pools de-identified trials and compounds, so the analysis cannot separate genuine treatment effects from trial-composition artifacts.1
- The endpoint critique is broader than one preprint: prior ALSFRS-R measurement work already showed that total scores can flatten multidomain disease progression into one misleading number.4,5
Shannon entropy is an information measure: instead of asking only whether the average ALSFRS score fell, it asks how widely patients are distributed across score categories inside each functional domain. For an ordinal scale such as ALSFRS, that distinction matters because 2 patient groups can have similar total-score slopes while moving through different combinations of speech, hand, walking, and breathing loss.
The methodological interpretation is stronger than the promotional one. The paper cannot show that an unnamed ALS drug worked; it shows that the standard summed-score endpoint can discard arm-level distributional structure before the main trial comparison ever starts.
PRO-ACT Included 4,581 Active-Arm and 2,931 Placebo Patients
The 2026 analysis used the Pooled Resource Open-Access ALS Clinical Trials (PRO-ACT) database, a public ALS trial resource assembled from contributed clinical-trial data.2 After cleaning records with missing time stamps or invalid item-level scores and restricting follow-up to 18 months from baseline, Rodriguez analyzed 77,889 observations from 8,819 unique patients.1
Treatment-arm labels: 7,512 patients had usable labels, including 4,581 assigned to active arms and 2,931 assigned to placebo.
Interpretation limit: the public database does not identify the original trial, compound, or mechanism for each active-arm assignment, which is why the result has to be read as a pooled endpoint signal.
- Scale: ALS Functional Rating Scale (ALSFRS), an ordinal function scale where item scores run from 0, meaning total loss of function, to 4, meaning normal function.
- Domains: Bulbar function, Fine Motor function, Gross Motor function, and Respiratory function.
- Time window: 19 monthly time points from baseline through month 18.
- Primary comparison: active-arm vs. placebo-arm Shannon entropy trajectories within each ALSFRS domain.
Integrated absolute divergence is the area between 2 entropy curves over time. A larger value means the active and placebo distributions were separated for more of the follow-up window or by a larger amount. Rodriguez then used 1,000 patient-label permutations to test whether the observed divergence exceeded what random active/placebo reassignment would produce.1
Fine Motor Entropy Peaked 5 Months Later in Active Arms
The most reader-visible result was the Fine Motor trajectory. Both arms started near 2.05 bits of entropy at baseline. Placebo patients reached peak Fine Motor entropy around month 8 and then partially reversed; active-arm patients reached peak entropy at month 13 and showed less reversal by month 18.1
In plain terms, the placebo population moved earlier into its widest spread of hand-related function levels. The active-arm population reached that distributional spread 5 months later. The Fine Motor integrated absolute divergence was 0.545, p = 0.001.
The Respiratory domain showed the largest contribution to total divergence. Respiratory integrated absolute divergence was 3.062, p < 0.001, with placebo entropy rising faster and reaching higher values from about month 4 onward. Bulbar and Gross Motor curves also differed visually, but their individual permutation tests were not significant: Bulbar IAD 0.588, p = 0.263; Gross Motor IAD 0.282, p = 0.579.1
Total ALSFRS Slopes Cannot Represent This Kind of Difference
ALSFRS total-score analysis sums multiple functional items into one score and then often compares linear decline slopes between trial arms. That makes trial analysis simple, but it also compresses different kinds of loss into the same scalar endpoint.
A patient losing swallowing function while walking remains stable can have a similar total-score slope to a patient losing walking function while swallowing remains stable. A total-score model can notice that both patients declined; it cannot preserve the distributional path that produced the decline.
Prior ALS endpoint papers already warned about this structure:
- ALSFRS-R construction: Cedarbaum et al. revised the scale to incorporate respiratory function, helping make ALSFRS-R a dominant trial endpoint.3
- Multidimensionality: Franchignoni et al. used Rasch analysis and found evidence that ALSFRS-R should be treated as a domain profile, not as a clean single dimension.4
- Endpoint overreach: van Eijk et al. argued that ALSFRS-R total score had become an overused primary endpoint because it can hide clinically important heterogeneity.5
- Trajectory timing: Proudfoot et al. showed that ALSFRS outcome behavior is tied to symptom onset and disease-stage timing, which complicates simple slope interpretation.6
Rodriguez extends that critique with a different measurement object: active and placebo populations can differ in the timing and shape of their domain-score distributions while a total-score slope fails to store that information.
The Pooled Active-Arm Signal Could Be Treatment, Composition, or Both
The main caveat is not small. PRO-ACT de-identifies constituent trials and compounds. The “active” arm is therefore a pooled label across experimental treatments with different mechanisms, enrollment criteria, visit schedules, and randomization ratios.
That creates 3 interpretations that the public dataset cannot separate:
- Genuine treatment effect: some active compounds may have delayed or changed domain-level functional transition without producing an obvious total-score slope win.
- Trial-composition artifact: pooled active and placebo arms may differ because the contributing trials enrolled different ALS phenotypes or used different active/placebo ratios.
- Mixed mechanism: treatment effects and compositional imbalance may both shape the entropy curves.
Simpson’s paradox means an aggregate result can differ from subgroup-level results when groups with different baseline structures are pooled. In this setting, the same aggregation problem cuts both ways: total-score summation could hide a real domain-specific treatment effect, while pooled cross-trial arms could also create a between-arm pattern that would not appear inside individual trials.7
That is why the paper’s strongest claim is narrower than a therapy claim. It says the discarded distributional information is not empty. It does not say which active compound changed ALS progression.
Preprint Status Keeps the Result in the Endpoint-Discovery Category
This analysis is a medRxiv preprint, so it has not passed peer review. The design also uses population-level entropy curves, not patient-level prediction. A clinician could not use this result to forecast an individual ALS patient’s trajectory or choose a treatment.
The evidence-strength note is straightforward:
- What the analysis can support: ALSFRS item-score distributions in PRO-ACT contain active/placebo arm divergence that total-score linear slopes cannot represent.
- What it cannot support: a named drug slowed ALS, active-arm patients personally improved, or entropy should replace standard endpoints without individual-trial validation.
- What would settle the next step: unblinded individual-trial decomposition showing whether the signal appears inside specific trials, specific compounds, or specific ALS phenotypes.
The minimum-n sensitivity check was reassuring within the paper’s own design. Using item-month thresholds of 20, 30, or 50 observations left the 5-month Fine Motor peak delay unchanged; total divergence remained p < 0.001 across thresholds.1
ALS Trial Endpoints Need Domain-Aware Stress Tests
For ALS trials, the practical implication is measurement discipline. A total ALSFRS or ALSFRS-R slope can remain useful, especially because regulators and trialists need interpretable primary endpoints. The risk is treating that slope as if it contains every clinically relevant pattern inside the scale.
Domain-aware endpoint checks could include:
- Domain trajectories: separate Bulbar, Fine Motor, Gross Motor, and Respiratory curves before collapsing into a total score.
- Distribution checks: entropy or other ordinal-distribution measures that track how patients spread across score categories over time.
- Phenotype stratification: bulbar-onset vs. limb-onset ALS, fast vs. slow progressors, and baseline respiratory status.
- Trial-level replication: reanalysis inside each original trial before interpreting a pooled active-arm pattern as treatment response.
The broader warning applies to other ordinal scales in neurology and psychiatry. Parkinson’s disease, Alzheimer’s disease, multiple sclerosis, depression, and schizophrenia trials often use summed ordinal endpoints. If domain-specific distributional timing carries treatment information, a single total-score slope can be a convenient summary and a lossy filter at the same time.
Questions About ALS Entropy Endpoints
Does this prove an ALS treatment worked?
No. The public PRO-ACT dataset pools active arms across de-identified trials and compounds, so the result cannot identify a specific drug effect. The safer conclusion is that the standard total-score endpoint can miss distributional structure in ALSFRS data.
Why use Shannon entropy instead of average ALSFRS decline?
Average decline asks how the mean score changes. Shannon entropy asks how widely patients are spread across item-score categories inside each domain. A treatment could alter timing or distribution shape even when the summed-score slope looks muted.
Could the entropy signal be an artifact?
Yes. Trial pooling, phenotype imbalance, differential dropout, and visit-schedule differences could contribute. Rodriguez’s permutation test shows the observed divergence exceeded random relabeling, but it cannot reconstruct the hidden trial and compound structure.
What would make the result more clinically actionable?
Individual-trial reanalysis would be the key step. If the same entropy divergence appears within specific randomized trials after accounting for ALS phenotype, baseline severity, and dropout, then entropy-style endpoints would become stronger candidates for secondary or exploratory trial endpoints.
References
- Rodriguez AM. Shannon entropy trajectories reveal between-arm distributional structure invisible to standard endpoint analysis in pooled ALS clinical trials. medRxiv. 2026. doi:10.64898/2026.04.20.26351319
- Atassi N, Berry J, Shui A, Zach N, Sherman A, Sinai E, et al. The PRO-ACT database: design, initial analyses, and predictive features. Neurology. 2014;83(19):1719-1725. doi:10.1212/WNL.0000000000000951
- Cedarbaum JM, Stambler N, Malta E, Hilt D, Thurmond B, Nakanishi A. The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. Journal of the Neurological Sciences. 1999;169(1-2):13-21. doi:10.1016/s0022-510x(99)00210-5
- Franchignoni F, Mora G, Giordano A, Volanti P, Chio A. Evidence of multidimensionality in the ALSFRS-R scale: a critical appraisal on its measurement properties using Rasch analysis. Journal of Neurology, Neurosurgery and Psychiatry. 2013;84(12):1340-1345. doi:10.1136/jnnp-2012-304701
- van Eijk RPA, de Jongh AD, Nikolakopoulos S, McDermott CJ, Eijkemans MJC, Roes KCB, et al. An old friend who has overstayed their welcome: the ALSFRS-R total score as primary endpoint for ALS clinical trials. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2021;22(3-4):300-307. doi:10.1080/21678421.2021.1879865
- Proudfoot M, Jones A, Talbot K, Al-Chalabi A, Turner MR. The ALSFRS as an outcome measure in therapeutic trials and its relationship to symptom onset. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2016;17(5-6):414-425. doi:10.3109/21678421.2016.1140786
- Bonovas S, Piovani D. Simpson’s paradox in clinical research: a cautionary tale. Journal of Clinical Medicine. 2023;12(4):1633. doi:10.3390/jcm12041633
- Rodriguez AM. An entropy-initiated coupled-trait ODE framework for modeling longitudinal cohort dynamics. PLOS ONE. 2026;21(3):e0344090. doi:10.1371/journal.pone.0344090