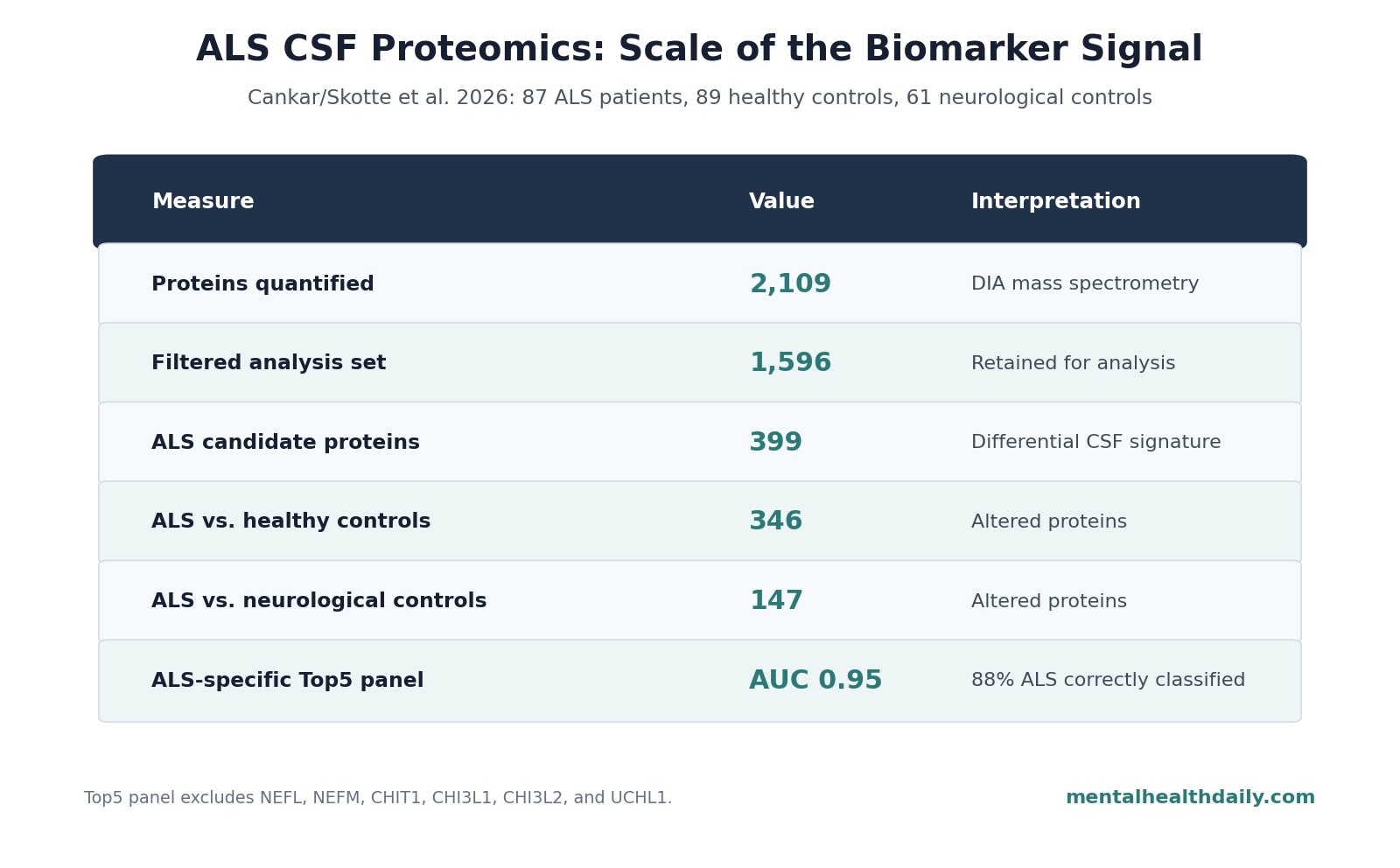
A 2026 cerebrospinal-fluid proteomics preprint involving 87 amyotrophic lateral sclerosis (ALS) patients, 89 healthy controls, and 61 neurological controls reported 399 ALS candidate proteins, complement markers that tracked disease stage, and a 5-protein panel that classified ALS vs. healthy controls with ROC AUC 0.95 after the best-known neurodegeneration markers were removed.1
Research Highlights
- CSF proteomics found a broad ALS signal: Cankar et al. quantified 2,109 cerebrospinal-fluid proteins, retained 1,596 after filtering, and identified 399 ALS candidate proteins.1
- ALS separated from 2 control groups: 346 proteins differed between ALS patients and healthy controls, 147 differed between ALS patients and neurological controls, and 94 were shared across both comparisons.1
- Complement tracked stage: 101 proteins correlated with ALSFRS-R functional scores, 58 correlated with disease duration, and complement proteins including C4A, C4B, C1S, and PROS1 rose in lower ALSFRS-R functional-stage bins or longer disease-duration bins.1
- Classic markers were not the whole answer: neurofilament light (NEFL) helped represent general axonal injury, but it did not significantly correlate with ALSFRS-R or disease duration in this cohort.1
- The 5-protein panel is not clinic-ready: MB, ITLN1, YWHAG, FCGR3A, and PGAM1 classified ALS vs. healthy controls with AUC 0.95, but the preprint lacks external validation and full ALS-mimic testing.1
Amyotrophic lateral sclerosis is a progressive motor neuron disease in which nerve cells controlling movement degenerate, causing weakness, paralysis, and eventually respiratory failure. Median survival is often around 2-4 years, so earlier diagnosis and better monitoring biomarkers have obvious appeal.6
The harder question is specificity. Neurofilament light is a structural axon protein released when neurons are injured; it is useful in ALS, but it also rises in other neurodegenerative diseases, disease mimics, and aging-related white-matter injury.2,6 A biomarker panel that only says “neurons are being damaged” may help triage, but it does not fully explain ALS biology or distinguish ALS from every relevant comparator.
87 ALS Patients, 89 Healthy Controls, and 61 Neurological Controls
The 2026 preprint analyzed cerebrospinal fluid (CSF), the clear fluid surrounding the brain and spinal cord. CSF proteomics means measuring many proteins in that fluid at once to infer which biological systems are active in disease.
Cankar et al. used data-independent acquisition mass spectrometry (DIA MS), a proteomics method that systematically fragments and measures peptides across a sample instead of targeting only a small preselected marker list. The design matters because ALS biomarker work can miss disease-specific biology when it focuses only on familiar markers such as NEFL, CHIT1, or UCHL1.
- Participants: 87 ALS patients, 89 healthy controls, and 61 neurological controls.
- Protein coverage: 2,109 proteins quantified, with an average of 1,688 proteins per sample.
- Filtered set: 1,596 proteins retained for analysis after processing.
- Reproducibility: sample correlations were R = 0.93-0.94, and group-wise median coefficients of variation were 28.1-29.9%.
- Prior-dataset overlap: around 70% of retained proteins overlapped earlier ALS proteomic datasets, while the figure caption reported 47% shared across the current study and 2 2023 comparator datasets.1
Neurological controls were especially useful. Healthy controls can make a biomarker panel look stronger than it will look in practice, because clinics need to distinguish ALS from other neurological presentations as well as from health.
399 CSF Proteins Met the ALS Candidate Criteria
ALS samples separated from both control groups in the proteomic analysis. The study reported 346 altered proteins in ALS vs. healthy controls, 147 altered proteins in ALS vs. neurological controls, and 94 shared dysregulated proteins across those 2 comparisons.1
Those numbers are larger than the prior CSF proteomics comparisons emphasized by the researchers. Earlier reports found smaller dysregulated-protein sets, including 97 and 33 proteins in 2 comparable studies cited by the preprint.3,4
The core signal was not mysterious: ALS CSF again showed established neurodegeneration and neuroinflammation markers.
- Axonal-injury proteins: NEFL and neurofilament medium polypeptide (NEFM) are structural neuron proteins that rise when axons are damaged.
- Neuronal-stress protein: UCHL1 is involved in protein turnover through the ubiquitin-proteasome system.
- Glial/inflammatory proteins: CHIT1, CHI3L1, and CHI3L2 are chitinase-family markers linked to glial activation and innate immune activity.
The more interesting claim was not that those known proteins rose again. The preprint argued that 399 differentially expressed CSF proteins formed a broader ALS-specific candidate set, including immune, metabolic, synaptic, and extracellular-matrix signals that could extend beyond generic injury markers.1
Complement Proteins Rose With Worse ALS Stage and Longer Disease Duration
The complement system is part of innate immunity: it tags biological material for clearance, helps coordinate inflammation, and can contribute to synapse removal when activated in the nervous system. In ALS, complement has been studied as both a disease mechanism and a candidate fluid-biomarker pathway.7
Cankar et al. found 17 closely interacting complement-pathway proteins. Of those, 13 were altered in ALS, and 8 were upregulated: C4A, C4B, C5, C7, C8G, C9, CFD, and VSIG4.1
Stage-related findings gave the complement result more clinical interest. ALSFRS-R, the Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised, is a 12-item functional score with a maximum of 48; higher scores mean better function. The preprint stratified patients into ALSFRS-R bins above 40, 31-40, and 0-30, and into disease-duration bins of 2 years or less vs. more than 2 years.
Complement markers moved with those clinical bins:
- C4B: rose across ALSFRS-R and disease-duration stages, with reported comparisons including p = 0.03, p = 0.005, p < 0.0001, p = 0.04, p = 0.004, and p < 0.0001.
- C4A: showed stage-related differences including p = 0.01 and p < 0.0001.
- C1S: showed a reported p = 0.01 stage difference.
- PROS1: showed a reported p = 0.004 difference.
That does not prove complement is driving progression. Cross-sectional CSF data cannot establish temporal causality. It does support a narrower claim: complement activation looked more tied to functional stage and disease duration than a simple diagnostic marker list would suggest.
NEFL Helped Diagnosis but Did Not Track ALSFRS-R in This Cohort
NEFL should not be dismissed. The 2026 preprint’s own machine-learning reference panel using canonical neurodegeneration markers reached ROC AUC 1.00, and the Top5 marker set included NEFL, CHI3L1, CHIT1, ITLN1, and UCHL1.1
The calibration is that a diagnostic signal and a monitoring signal are not identical. In this cohort, 101 proteins correlated with ALSFRS-R and 58 correlated with disease duration, but NEFL was not significantly correlated with either measure.1
That pattern fits the broader fluid-biomarker problem in ALS. Reviews keep treating neurofilament as one of the strongest available markers, but a marker can be useful for prognosis or diagnosis without capturing every disease-stage mechanism or every treatment-response question.2
The 5-Protein Panel Excluded the Obvious Neurodegeneration Markers
The researchers then removed 6 established neurodegeneration and inflammation markers: NEFL, NEFM, CHIT1, CHI3L1, CHI3L2, and UCHL1. After that exclusion, the ALS-specific Top20 model still reached ROC AUC 0.98 and correctly classified 96% of ALS patients. A smaller Top5 panel reached ROC AUC 0.95 and correctly classified 88% of ALS patients.1
The 5 proteins were MB, ITLN1, YWHAG, FCGR3A, and PGAM1.
- MB: myoglobin, a muscle-related protein that may reflect denervation-associated muscle atrophy rather than a brain-only signal.
- ITLN1: intelectin-1, a metabolism-linked protein with possible vascular and neuroprotective relevance.
- YWHAG: a 14-3-3 protein involved in neuronal signaling and stress responses.
- FCGR3A: an immune receptor that can mark antibody-driven innate immune activation.
- PGAM1: a glycolysis enzyme that may reflect metabolic strain and oxidative-pressure responses.
Adjacent proteomics evidence: plasma proteomics is moving in a related direction. Chia et al. reported a plasma proteomics candidate biomarker panel predictive of ALS, while CSF studies such as Dellar et al. and Trautwig et al. keep pointing to inflammation, endoplasmic-reticulum stress, network-level differences, and sporadic-vs.-familial overlap.5,8,9
The shared theme is that ALS biomarkers are becoming panels and pathways, not single magic proteins.
This Is Discovery Proteomics, Not a Ready ALS Test
The strongest version of the finding is also the safest version: this preprint identified candidate ALS CSF protein signatures that deserve validation. It did not produce a clinic-ready diagnostic test.
Evidence-strength note: the study was cross-sectional, posted as a medRxiv preprint, and not yet peer reviewed. Its machine-learning results were internally cross-validated, but they still need external replication, longitudinal testing, and harder differential-diagnosis comparisons against ALS mimics and related neurodegenerative diseases.
Three limits are especially important:
- External validation is missing. AUC 0.95 inside one discovery dataset can fall when the model meets new hospitals, new assay workflows, new ancestry distributions, and messier clinical cases.
- Healthy-control separation is easier than clinical diagnosis. The key 5-protein panel was framed around ALS vs. healthy controls, while real diagnostic use must separate ALS from mimic syndromes, neuropathies, myelopathies, and other motor-neuron presentations.
- Stage markers need longitudinal proof. Complement proteins rising with worse ALSFRS-R or longer disease duration is compatible with progression tracking, but only repeated sampling can show whether a marker changes before, during, or after clinical decline.
Clinically, the useful near-term message is not “order this panel.” It is that future ALS biomarker work should separate 3 layers: generic neuronal injury, ALS-specific disease biology, and stage-sensitive monitoring markers. Cankar et al. made that separation clearer, but validation decides whether it becomes usable.
Questions About ALS CSF Proteomics
Does this mean ALS can now be diagnosed from 5 CSF proteins?
No. The 5-protein panel classified ALS vs. healthy controls with AUC 0.95 in this dataset, but it has not been externally validated and was not tested across the full clinical range of ALS mimics.
Why is CSF used instead of blood?
CSF is closer to the central nervous system, so it can carry brain and spinal-cord protein signals more directly than blood. Blood is easier to collect and better for screening, but CSF can be more informative for discovery-stage neurodegeneration biology.
Why does complement get emphasis?
Complement proteins were altered in ALS, and several also rose with worse ALSFRS-R bins or longer disease duration. That made complement a candidate stage-tracking pathway rather than only a diagnostic difference.
Is NEFL still useful?
Yes. NEFL remains one of the strongest ALS fluid biomarkers, especially as an axonal-injury marker. The caveat is that it is not ALS-specific and did not significantly track ALSFRS-R or disease duration in this cohort.
References
- Cankar N, Qvist FL, Frahm AS, et al. Proteomic profiling of CSF reveals stage-specific changes in amyotrophic lateral sclerosis patients. medRxiv. 2026. doi:10.64898/2026.04.13.26350753
- Irwin KE, Sheth U, Wong PC, Gendron TF. Fluid biomarkers for amyotrophic lateral sclerosis: a review. Molecular Neurodegeneration. 2024;19:9. doi:10.1186/s13024-023-00685-6
- Dellar ER, et al. Data-independent acquisition proteomics of cerebrospinal fluid implicates endoplasmic reticulum and inflammatory mechanisms in amyotrophic lateral sclerosis. Journal of Neurochemistry. 2023. doi:10.1111/jnc.16030
- Oh S, Jang Y, Na CH. Discovery of biomarkers for amyotrophic lateral sclerosis from human cerebrospinal fluid using mass-spectrometry-based proteomics. Biomedicines. 2023;11. doi:10.3390/biomedicines11051250
- Zhou J, et al. Biomarkers in cerebrospinal fluid for amyotrophic lateral sclerosis phenotypes. Annals of Clinical and Translational Neurology. 2023;10:1467-1480. PubMed
- Masrori P, Van Damme P. Amyotrophic lateral sclerosis: a clinical review. European Journal of Neurology. 2020;27:1918-1929. doi:10.1111/ene.14393
- Kjældgaard AL, et al. Complement profiles in patients with amyotrophic lateral sclerosis: a prospective observational cohort study. Journal of Inflammation Research. 2021;14:1043-1053. doi:10.2147/jir.s298307
- Trautwig AN, et al. Network analysis of the cerebrospinal fluid proteome reveals shared and unique differences between sporadic and familial forms of amyotrophic lateral sclerosis. Molecular Neurodegeneration. 2025;20. PubMed
- Chia R, et al. A plasma proteomics-based candidate biomarker panel predictive of amyotrophic lateral sclerosis. Nature Medicine. 2025. doi:10.1038/s41591-025-03890-6