A 2026 first-in-human medRxiv preprint reported that closed-loop subgaleal intersectional short-pulse stimulation shortened stimulated seizures by 52% on average and reduced seizure incidence by 80.9% after 48 hours in 5 high-frequency therapy-resistant epilepsy patients. The signal is promising because it combines responsive seizure detection with electrode strips placed under the scalp rather than electrodes implanted into brain tissue, but the evidence is still small, unblinded, inpatient, and not yet peer reviewed.
Research Highlights
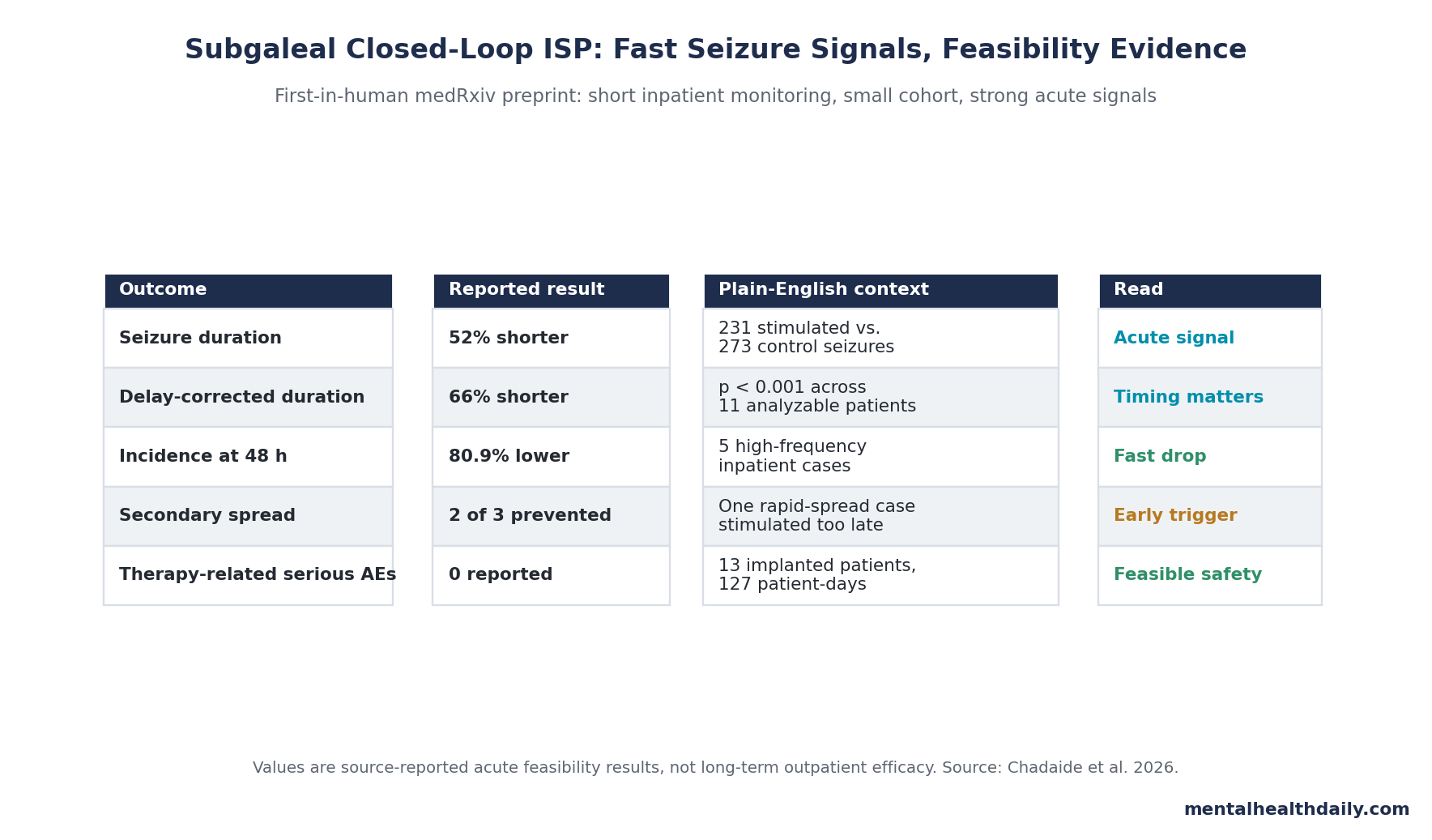
- Seizures were shorter: stimulated seizures were 52% shorter on average, and delay-compensated analyses estimated 66% shortening across 272 baseline vs. 224 stimulated seizures from 11 patients.
- Incidence dropped quickly: in 5 patients with high baseline seizure frequency, seizure incidence fell 55.8% after 24 hours, 80.9% after 48 hours, and 96.0% after 72 hours of treatment exposure.
- Safety looked feasible: 13 implanted patients contributed 2283 hours of video-EEG across 127 patient-days, with 0 serious therapy-related adverse events and 2 unrelated grade 3 events.
- Timing was central: delayed first stimulation tracked longer seizures (r2 = 0.52; p < 0.001), which means the detector and automatic repeat protocol may be as important as the waveform itself.
- Evidence strength remains limited: the manuscript is a 2026 medRxiv preprint, the high-frequency incidence analysis included only 5 patients, and inpatient antiseizure-medication tapering complicates long-term inference.
Intersectional short-pulse stimulation (ISP) is a neuromodulation method that sends ultra-brief, distributed electrical pulses through multiple electrode pairs so the overlapping fields concentrate more strongly near a target brain region. In this study, the electrodes were subgaleal: placed under the scalp but above the skull, avoiding the depth electrodes or cortical leads used by more invasive responsive systems.
Closed-loop stimulation means the device records electrical activity, detects a seizure pattern, and triggers stimulation during the event rather than stimulating on a fixed schedule. That timing difference is central: a device that interrupts a seizure early is trying to shorten or abort the episode, while open-loop devices such as vagus nerve stimulation (VNS) and anterior thalamic deep brain stimulation (DBS) usually work through slower network modulation.
13 Implanted Patients Produced 504 Control and Stimulated Seizures
Chadaide et al. enrolled 15 adults with therapy-resistant epilepsy between November 2021 and September 2025. Two withdrew before implantation, leaving 13 implanted patients and 2283 hours of video-electroencephalography (video-EEG — synchronized seizure video plus brain electrical recordings) across 127 inpatient patient-days.
The study compared each patient’s baseline seizures with seizures treated by the device after seizure detection and stimulation planning. Across the main seizure-duration dataset, researchers recorded 273 control seizures and 231 stimulated seizures. One patient was excluded from analysis because identifiable ictal EEG waveforms were unavailable, and 12 patients completed the experimental protocol.
Device logic: the system used 4 externalized 8-contact subgaleal electrode strips, a 32-channel EEG-processing unit, machine-learning seizure detection, and high-intensity short pulses timed to the prominent seizure frequency. A single stimulation “dose” consisted of 3 repeats of 50-millisecond half-sine pulse trains, with repeat timing adjusted to the seizure oscillation.
Patient comfort: perception limits averaged 8.1 mA with a standard deviation of 3.9 mA, while tolerability thresholds averaged 28.2 mA with a standard deviation of 11.2 mA. Subjective visual-analog-scale discomfort scores tracked stimulation intensity strongly (r2 = 0.81 across 303 observations), which matters because a scalp-adjacent system still has to be tolerable during repeated seizure-triggered use.
Seizure Duration Fell 52%, With Stronger Effects After Timing Correction
Stimulated seizures were 52% shorter on average than control seizures, with substantial patient-to-patient variability. After accounting for the delay between seizure onset and the first delivered stimulation, estimated shortening increased to 66% (p < 0.001; 272 baseline vs. 224 stimulated seizures from 11 patients).
Patient-level mean comparisons pointed in the same direction: raw shortening was 50% with a standard deviation of 25%, and delay-compensated shortening was 61% with a standard deviation of 30% (p = 0.005 for 11 vs. 11 paired mean values). Seizure duration shortened in 10 of 11 analyzable patients; 8 high-frequency patients had statistically significant duration reductions, while 2 lower-count patients showed the same direction without enough events for a strong test.
One patient did not show a duration benefit. That exception is useful rather than embarrassing: it keeps the result in feasibility-trial territory instead of implying a uniform device effect across all seizure networks, electrode positions, detection delays, and stimulation sequences.
Stimulation Timing Looked Like a Dose Variable
Timing behaved like a dose variable: the longer the delay between seizure onset and the first ISP pulse, the less seizure shortening the researchers observed.
First-pulse delay: delayed stimulation made seizures 1.29 times longer relative to the delay itself (r2 = 0.52; p < 0.001; 189 seizures from 5 patients). In plain English, earlier stimulation tracked better seizure termination.
Repeat-pulse delay: when multiple ISP stimuli were delivered during one seizure, seizure durations became 1.4 times longer than the increase in mean stimulation delay (r2 = 0.81; p < 0.001; 189 seizures from 5 patients). The study used manual, semi-automatic, and fully automatic modes, and fully automatic stimulation had the shortest delay.
This is the most clinically interesting engineering point. If a future outpatient device reduces human confirmation delays and repeats stimulation automatically when ictal activity persists, the treatment could perform differently from this inpatient feasibility setup.
Seizure Incidence Fell 80.9% After 48 Hours in 5 High-Frequency Patients
The study’s second cohort focused on patients with relatively high baseline seizure incidence and high-coverage closed-loop stimulation. In those 5 patients, seizure incidence fell progressively during treatment exposure: 55.8% after 24 hours, 80.9% after 48 hours, and 96.0% after 72 hours (median with interquartile ranges of 42.4%, 36.7%, and 19.3%).
Total time spent in seizures moved similarly, with reductions of 89.7%, 98.2%, and 97.5% after 24, 48, and 72 hours. Three high-burden patients had at least 1 full seizure-free day before explantation; the remaining 2 had marked reductions with a trend toward seizure freedom.
Generalization: ISP stimulation prevented secondary generalization in 2 of 3 patients susceptible to spread from focal to bilateral tonic-clonic seizures. In the third case, seizures generalized in less than 5 seconds, while semi-automatic stimulation arrived after 9 and 12 seconds; that case again points to detection speed rather than simply waveform strength.
No Serious Therapy-Related Adverse Events Were Reported
Safety data were reassuring for a first-in-human device trial, but they should be read as feasibility evidence. Researchers observed 50 grade 1 and 26 grade 2 adverse events during 127 experimental days in 13 implanted patients. Two grade 3 events occurred — psychosis related to antiseizure medication tapering and fever due to urinary infection — but both were judged unrelated to the subgaleal implantation or ISP stimulation.
No serious therapy-related adverse events and no grade 4 or grade 5 events were reported. All adverse events resolved spontaneously or with treatment. The adverse-event table described most events as mild, transient, and related to surgical implantation rather than stimulation itself; stimulation-related events were mild.
Evidence-strength note: this was a small proof-of-concept study, not a definitive safety trial. Rare complications, infection risk, hardware durability, outpatient tolerability, psychiatric effects during medication changes, and long-term scalp/skull tissue issues need larger and longer follow-up.
How Subgaleal ISP Fits Against VNS, DBS, and RNS
Approved epilepsy neuromodulation already includes VNS, anterior thalamic DBS, and responsive neurostimulation (RNS). VNS and DBS are usually open-loop approaches: they stimulate on programmed schedules and may reduce pathological synchrony over weeks or months. RNS is closed-loop and records brain activity, but it requires cranial implantation and directly targets a limited number of seizure zones.
Subgaleal ISP is trying to occupy a different design space: more focal and responsive than standard noninvasive scalp stimulation, less invasive than intracranial RNS or DBS, and faster-acting than open-loop palliative neuromodulation. Ryvlin et al. summarized the established options as effective but imperfect palliative therapies; Chadaide et al. tested whether the closed-loop seizure-interruption idea could be moved closer to the skull surface.
The concept is not new from scratch. Berenyi et al. reported closed-loop control of epilepsy by transcranial electrical stimulation in rats in 2012, and Kozak and Berenyi later reported sustained closed-loop seizure control in absence-epilepsy rats. The 2026 preprint is important because it moves that logic into adults with therapy-resistant epilepsy while using a subgaleal electrode strategy.
Why This Preprint Does Not Prove Long-Term Seizure Freedom
The strongest reading is calibrated: the acute seizure-shortening and incidence signals are unusually strong for a first-in-human neuromodulation preprint, but the study does not establish long-term outpatient efficacy.
- Small cohort: 13 implanted patients is enough for feasibility, not for subgroup claims by seizure type, etiology, or localization.
- Short duration: inpatient monitoring lasted days, while epilepsy-device decisions are made over months to years.
- Medication tapering: antiseizure medication reduction during presurgical monitoring can alter seizure incidence and seizure clustering.
- Unblinded annotation: stimulation artifacts meant EEG readers could not be fully blinded to treatment status.
- Detector dependence: the device effect depends on seizure detection, confirmation delay, repeat stimulation rules, and patient-specific sequence planning.
Those limits do not erase the signal. They define the next trial: longer outpatient follow-up, automated detection and repeat stimulation, control periods that separate device effects from inpatient medication changes, and direct comparison against current neuromodulation pathways.
Questions About Closed-Loop Subgaleal ISP for Epilepsy
Is subgaleal ISP the same thing as RNS?
No. RNS is an implanted responsive neurostimulation system that records and stimulates from intracranial leads. Subgaleal ISP uses electrode strips under the scalp and above the skull, aiming to focus short pulses through field intersections while avoiding direct brain implantation.
Does the preprint prove seizure freedom?
No. Three high-frequency patients had at least 1 seizure-free day before explantation, and incidence fell sharply in 5 patients, but the study was too short and small to prove durable seizure freedom.
What would make the evidence stronger?
A larger controlled trial with longer outpatient follow-up, predefined seizure-frequency endpoints, automated stimulation timing, adverse-event surveillance, and comparison against standard neuromodulation options would move the claim from feasibility toward clinical efficacy.
Why is the 80.9% number not the whole story?
The 80.9% reduction was a median incidence change after 48 hours in 5 high-frequency patients. It is a strong early signal, but it comes from a small subgroup during inpatient monitoring rather than a long-term randomized outpatient trial.
References
- Chadaide Z, Fabo D, Szoboszlay M, et al. Closed-loop, subgaleal intersectional short-pulse stimulation for the treatment of therapy-resistant epilepsy in adults. medRxiv. 2026. doi:10.1101/2025.09.27.25334859
- Heck CN, King-Stephens D, Massey AD, et al. Two-year seizure reduction in adults with medically intractable partial onset epilepsy treated with responsive neurostimulation: final results of the RNS System pivotal trial. Epilepsia. 2014;55(3):432-441. doi:10.1111/epi.12534
- Ryvlin P, Rheims S, Hirsch LJ, Sokolov A, Jehi L. Neuromodulation in epilepsy: state-of-the-art approved therapies. Lancet Neurol. 2021;20(12):1038-1047. doi:10.1016/S1474-4422(21)00300-8
- Berenyi A, Belluscio M, Mao D, Buzsaki G. Closed-loop control of epilepsy by transcranial electrical stimulation. Science. 2012;337(6095):735-737. doi:10.1126/science.1223154
- Kozak G, Berenyi A. Sustained efficacy of closed loop electrical stimulation for long-term treatment of absence epilepsy in rats. Sci Rep. 2017;7:6300. doi:10.1038/s41598-017-06684-0
- Chen Y, Lin Y, Zhou D, et al. Transcranial direct current stimulation in the management of epilepsy: a meta-analysis and systematic review. Front Neurol. 2024;15. doi:10.3389/fneur.2024.1462364