A 2026 medRxiv preprint reported that an at-home subcallosal cingulate cortex deep brain stimulation (SCC DBS) recording system could track stable recovery in severe treatment-resistant depression: in 7 analyzable patients, the local-field-potential biomarker predicted weekly recovery states with 0.72 ± 0.16 accuracy.1 The useful claim is not that brain recordings can diagnose depression broadly; it is that a specific SCC DBS signal may help separate core depression recovery from symptom noise during long-term stimulation management.
Research Highlights
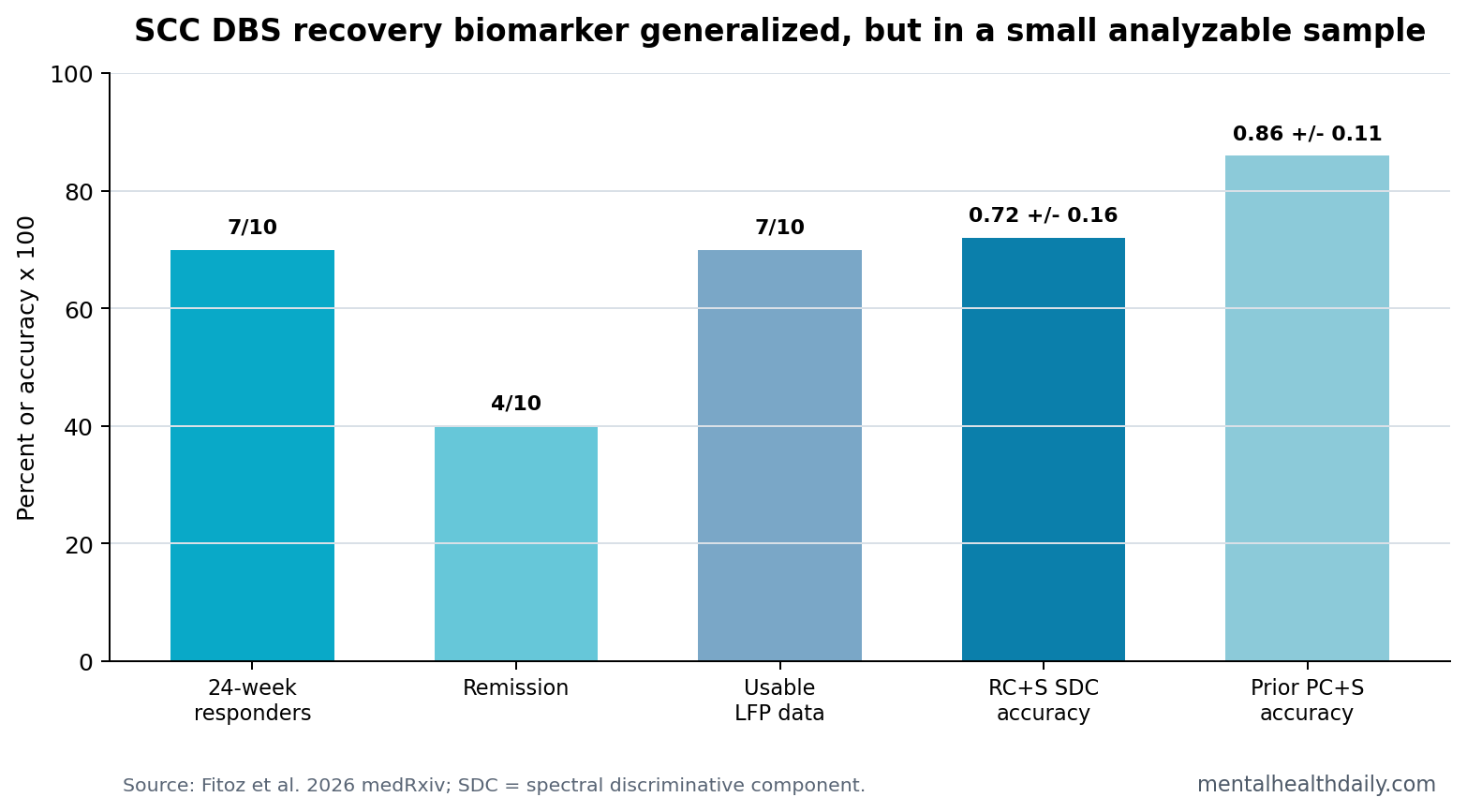
- Recovery-state accuracy was modest: the spectral discriminative component predicted HDRS-defined stable recovery with 0.72 ± 0.16 accuracy in the new RC+S cohort, compared with 0.86 ± 0.11 in the prior PC+S cohort.1
- Clinical response was high: 7 of 10 implanted patients met the 24-week response criterion, and 4 of 10 reached remission by an HDRS score below 8.1
- Usable electrophysiology was narrower: 7 of 10 participants had chronic LFP data available after 3 were excluded for unexplained recording-property shifts.1
- Network integrity tracked timing: lower fractional anisotropy in key SCC-connected tracts correlated with delayed stable response, with rho values from −0.88 to −0.93.1
- Translation remains DBS-specific: the 2026 signal is a management marker for implanted SCC DBS patients, not a general depression test for routine clinics.
Local field potentials are low-voltage electrical rhythms recorded from brain tissue near an implanted electrode. In this study, the signal came from SCC DBS hardware in people already receiving stimulation for treatment-resistant depression, not from scalp EEG or a wearable consumer device.
Treatment-resistant depression means depressive illness that has not improved adequately after multiple standard treatments. SCC DBS is an invasive neurosurgical approach used only in severe, carefully selected cases. The clinical challenge is that rating scales such as the Hamilton Depression Rating Scale (HDRS) can move because of sleep, appetite, anxiety, stress, or temporary life events, even when the depression circuit targeted by DBS is not truly relapsing.
7 of 10 Patients Responded, but Only 7 Had Usable Chronic LFP Data
Fitoz et al. implanted 10 people with treatment-resistant depression using the Medtronic Summit RC+S platform. The system allowed at-home recordings, mood ratings, and video diaries. Compliance was high: average weekly compliance across participants was 93.95%, with a standard deviation of 7.01.1
Clinical outcomes looked strong for such a severe group. Mean presurgical HDRS was 23.93, and mean HDRS fell to 10 by the end of the 6-month observation period. Seven patients met response at the predefined 24-week point, 4 reached remission, and 1 additional patient met response at week 25.
Biomarker denominator: the electrophysiology analysis was smaller than the implanted cohort. Chronic data were analyzable in 7 patients after 3 were excluded because of sudden unexplained shifts in recording properties. That denominator is central to the strength of the claim.
The SDC Biomarker Predicted Stable Recovery With 0.72 Accuracy
The spectral discriminative component (SDC) is a mathematical summary of SCC local-field-potential features. The model was trained previously in a 5-person PC+S cohort and then applied to the new RC+S cohort without retraining. That design is stronger than re-fitting a model to the same small group it is supposed to explain.
Weekly SDC-derived depression vs. stable-recovery states predicted HDRS-derived states with 0.72 ± 0.16 accuracy. The earlier PC+S cohort had 0.86 ± 0.11 accuracy, and the difference between cohorts was not statistically confirmed, U = 25.50, p = 0.22.1
The chart-level read is deliberately cautious. A 72% weekly-state classifier is not a magic depression readout. It is still potentially useful because the relevant decision is narrower: whether an implanted patient appears to be in a stable core-depression recovery state or needs closer clinical review.
The Signal Looked More Specific to Core Depression Than Residual Anxiety
One important result came from moments when the SDC suggested stable response before the HDRS had fully stabilized. In 4 responding participants, the disagreement period had proportionally more HDRS “psychic anxiety” than “depressed mood.” The researchers interpreted this as evidence that the biomarker was closer to DBS-responsive core depression than to residual anxiety symptoms.1
- Depressed mood: more directly aligned with the syndrome SCC DBS is supposed to treat.
- Residual anxiety: may persist after core depression improves and may need psychotherapy, medication, or non-DBS management.
- Clinical use case: a biomarker that does not overreact to every anxiety-heavy HDRS fluctuation could prevent unnecessary stimulation changes.
White-Matter and Functional Connectivity Patterns Matched Response Timing
Network-level treatment: SCC DBS works through a network, not a single isolated point. Fitoz et al. found that lower fractional anisotropy, an MRI-derived measure of white-matter microstructure, correlated with delayed stable response in the left cingulum bundle, right uncinate fasciculus/ventral amygdalofugal pathway, and left forceps minor.
The reported correlations were strong: rho = −0.91, −0.93, and −0.88, all p < 0.001.1
Functional connectivity pointed in a similar direction. Lower SCC connectivity with the left dorsal anterior cingulate cortex, right anterior insula, and left ventromedial prefrontal cortex also correlated with delayed response. White-matter integrity and SCC-cortical connectivity were themselves positively correlated in the corresponding pathways.
Mechanistic interpretation: the biomarker sits inside a larger depression network. Recording a useful local signal may depend partly on whether stimulation engages connected white-matter pathways strongly enough to move the clinical state.
Preprint and Sample-Size Limits Keep This Out of Routine Depression Care
Evidence-strength note: this was a small preprint in an implanted neurosurgical cohort. It can support DBS decision-support development and replication of the earlier 5-person biomarker result. It cannot show that local-field-potential monitoring should guide ordinary antidepressant treatment, diagnose depression, or replace clinical assessment.
Adjacent DBS evidence: Alagapan et al. previously identified the SCC spectral biomarker in a small cohort, and tractography-guided SCC DBS studies have linked response to engagement of specific white-matter pathways.2,3
The 2026 contribution is practical: moving from in-clinic downloads toward repeated at-home recording while testing whether the same signal survives new hardware, a different clinical team, and daily-life variability.
Decision-support standard: the next bar is not a dramatic headline about brain-reading depression. It is prospective evidence that biomarker-informed decisions improve patient outcomes, reduce unnecessary stimulation changes, or catch relapse earlier than expert clinical monitoring alone.
Why At-Home Recording Changes the DBS Biomarker Question
In-clinic electrophysiology can show that a signal exists, but depression recovery unfolds between visits. The 2026 platform moved LFP collection into the patient’s home, paired recordings with repeated mood ratings, and made the system closer to the environment where future DBS management would actually happen.
A biomarker that works during carefully controlled clinic visits may fail when sleep timing, daily stress, stimulation status, and ordinary behavior vary.
The RC+S cohort therefore tested more than replication. It tested whether the same recovery-state concept survived a different device, a different clinical team, and repeated home use. The answer was directionally yes, but not cleanly enough to skip the engineering step. Accuracy was lower than the earlier PC+S estimate, and 3 implanted patients could not be used in chronic electrophysiology analysis because of recording-property shifts.
Operational implication: before SCC DBS biomarkers can guide routine care, the pipeline needs artifact detection, hardware-stability monitoring, and prespecified rules for when a recording channel becomes unreliable. A 0.72 accuracy estimate in 7 analyzable patients is promising only if the system can also explain when not to trust itself.
Residual Anxiety Can Explain HDRS and Biomarker Mismatch
The anxiety finding is clinically important because it prevents a sloppy interpretation of the biomarker. If SCC DBS improves core depression but anxiety persists, a total HDRS score can make the patient look less recovered than the stimulation-responsive syndrome really is. That mismatch is exactly where a brain-state marker could help.
For a patient, the difference is not academic. If residual anxiety drives the score, increasing stimulation may not help and could expose the person to unnecessary programming changes. If core depressive mood is returning, delayed DBS adjustment could prolong relapse. The biomarker’s value depends on whether it can sort those situations better than a clinician reading the rating scale alone.
Clinical boundary: this does not make anxiety secondary or unimportant. It means the intervention target matters. Anxiety after SCC DBS recovery may call for a different treatment lane than DBS programming, while depressive relapse may call for direct stimulation review.
Questions About SCC DBS Depression Biomarkers
Does this biomarker diagnose depression?
No. It was tested in people already implanted with SCC DBS for severe treatment-resistant depression. It tracks recovery-state patterns during DBS management, not whether an unimplanted person has depression.
Why can HDRS and the biomarker disagree?
HDRS includes symptoms such as sleep, appetite, and anxiety. Those can worsen transiently even when core depressive mood has improved. A useful DBS biomarker may help clinicians decide whether the issue is stimulation-related depression recurrence or a different symptom problem.
What would make this clinically stronger?
A larger prospective trial would need to show that using the biomarker to guide DBS adjustments improves outcomes compared with expert clinical management alone, ideally with prespecified thresholds and independent validation.
References
- Fitoz S, et al. Common electrophysiology biomarkers collected at home track stable recovery in subcallosal cingulate deep brain stimulation for treatment-resistant depression. medRxiv. 2026. doi:10.64898/2026.04.13.26350107
- Alagapan S, et al. Cingulate dynamics track depression recovery with deep brain stimulation. Nature. 2023. doi:10.1038/s41586-023-06541-3
- Riva-Posse P, et al. A connectomic approach for subcallosal cingulate deep brain stimulation surgery in treatment-resistant depression. Molecular Psychiatry. 2018. PubMed
- Crowell AL, et al. Long-term outcomes of subcallosal cingulate deep brain stimulation for treatment-resistant depression. Biological Psychiatry. PubMed