Transcranial direct current stimulation (tDCS) has been pitched as a scalable cognitive-enhancement tool for schizophrenia, where roughly 98% of patients show working-memory deficits, but a 2026 sham-controlled crossover trial from Ke et al. delivered the standard 1.5 mA anodal protocol over the right DLPFC to 27 stable patients and found no detectable benefit over sham.1
Research Highlights
- No significant Session × Time interactions for most working-memory tasks. Anodal tDCS produced no detectable acute improvement on Corsi Block-Tapping Tasks (visuospatial working memory) or Forward Digit Span (verbal working memory) compared to sham.1
- One outlier interaction did not survive post-hoc tests. The Corsi Backward span showed a significant two-way interaction (F(1,26) = 6.011, p = 0.021), but post-hoc analysis showed no significant pre-to-post change in either the anodal or sham condition — consistent with chance.1
- Baseline cognitive capacity did not moderate the effect. Linear mixed-effects models treating baseline scores as a continuous moderator found no significant Session × Time × Baseline three-way interactions (all p > 0.113), failing to support the hypothesis that low-baseline patients would respond differently from high-baseline patients.1
- The sample was powered for moderate-to-large effects relative to sham. n = 27 in a within-subject crossover detects effects around Cohen’s d ≈ 0.5 vs. sham reliably. The null at this sample size narrows the plausible effect of single-session rDLPFC stimulation but does not exclude very small effects.1
- The result fits a tightening literature. Recent meta-analyses of tDCS in schizophrenia and other psychiatric populations report small-to-moderate effects with high heterogeneity; single-session, single-target protocols increasingly look insufficient.2,3
Cognitive deficits in schizophrenia are the strongest predictor of long-term functional outcomes — stronger than positive symptoms (delusions, hallucinations) or negative symptoms (flattened affect, withdrawal).4 Antipsychotic medications produce mild-to-modest cognitive benefit at best.
Cognitive remediation therapy works modestly but is resource-intensive. Non-invasive brain stimulation has been pursued as a faster, scalable alternative for over a decade.
The Ke result lands in a literature where the early enthusiasm has narrowed considerably and the question is no longer whether tDCS produces dramatic acute cognitive gains in schizophrenia (it doesn’t), but whether multi-session, individualized, or network-based protocols might still produce meaningful benefit.
Ke 2026: 27 Stable Patients, Within-Subject Crossover, Sham-Controlled
The trial recruited 27 clinically stable adults with schizophrenia, with each participant receiving both active anodal tDCS and sham stimulation in counterbalanced order on separate days.1
The stimulation protocol:
- Site: right dorsolateral prefrontal cortex (rDLPFC), the standard target for working-memory tDCS protocols.
- Current: 1.5 mA anodal stimulation, in the upper end of the therapeutic-protocol range.
- Duration: 15 minutes per session.
- Sham: brief ramp-up and ramp-down to mimic the cutaneous sensation of active stimulation without sustained current delivery.
Working memory was assessed before and after each stimulation session with two computerized tasks:
- Corsi Block-Tapping Tasks (CBT): a visuospatial working-memory paradigm requiring participants to reproduce sequences of highlighted blocks in forward and backward order.
- Forward Digit Span: a verbal working-memory task requiring repetition of progressively longer digit sequences.
Participants were stratified into high- and low-performance subgroups via a median split on baseline Corsi scores, to test the hypothesis that lower-baseline patients might respond differently from higher-baseline patients — a baseline-dependent effect predicted by some prior literature.
The trial was registered on ClinicalTrials.gov (NCT03872310) before data collection.
Primary Result: No Acute Improvement in Visuospatial or Verbal Working Memory
The pre-specified primary analysis used two-way repeated-measures ANOVA with Session (anodal vs. sham) and Time (pre vs. post) as factors.
The Session × Time interaction is the test of interest — a significant interaction would mean anodal stimulation produced a different change from baseline than sham did.
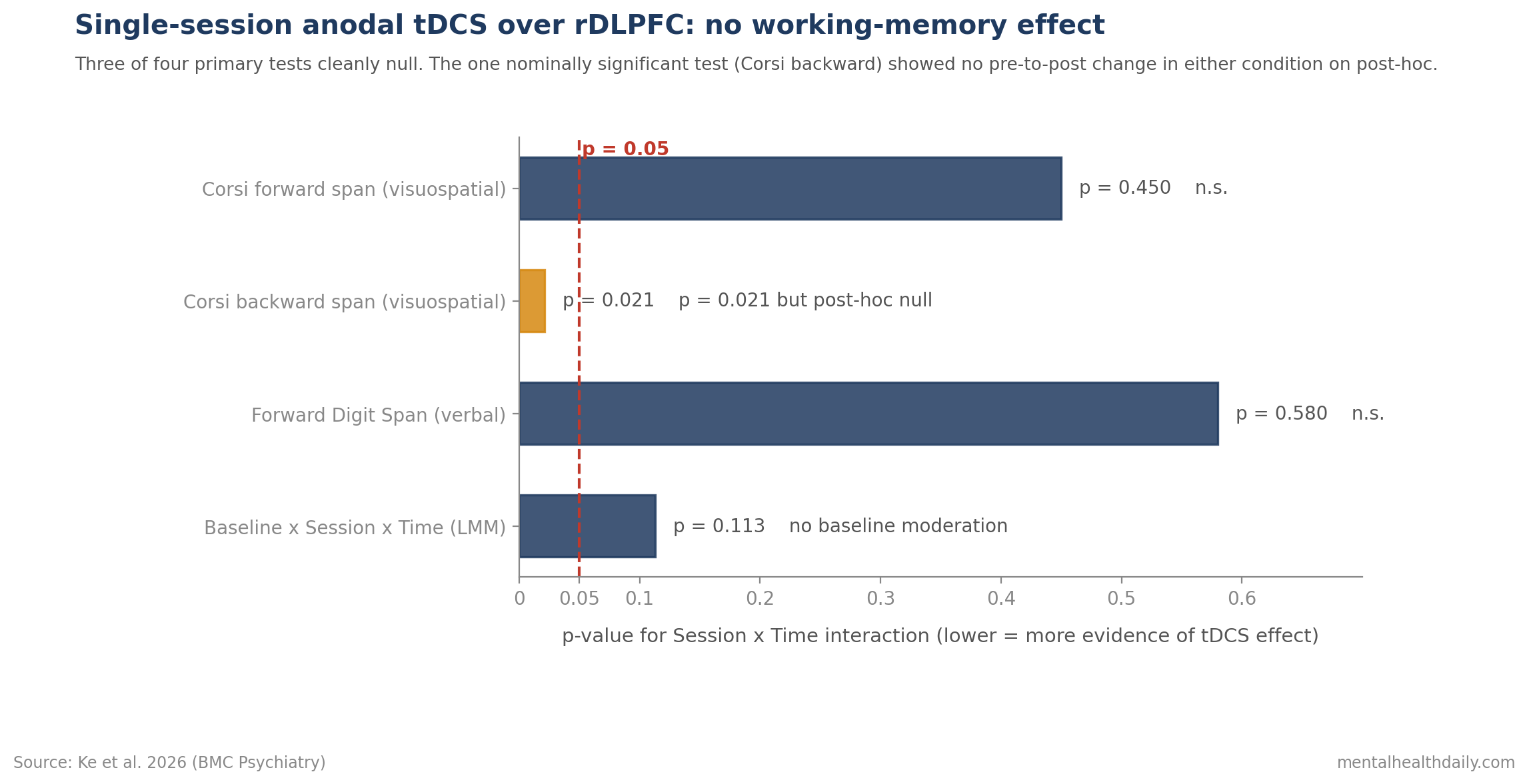
Corsi forward (visuospatial WM): no significant interaction.
Corsi backward (visuospatial WM, executive component): significant interaction at p = 0.021 (F(1,26) = 6.011), but post-hoc tests showed no significant pre-to-post change in either the anodal or sham condition. This is the kind of result that produces a positive omnibus test from random fluctuation rather than a real effect.
Forward Digit Span (verbal WM): no significant interaction.
Across the full task battery, the directional pattern was for tDCS effects to cluster around the null, with no consistent advantage of anodal over sham stimulation.
The Baseline-Moderation Test: Also Null
The pre-specified secondary analysis used linear mixed-effects models (LMM) with baseline performance as a continuous moderator. The hypothesis was that lower-performing participants might benefit more from tDCS than higher-performing ones — a “ceiling effect” account that has been used to explain heterogeneity in prior tDCS studies.
The three-way Session × Time × Baseline interactions across all working-memory tasks were non-significant (all p > 0.113).1
Translation: the data did not support the idea that single-session anodal rDLPFC tDCS works in lower-performing schizophrenia patients but is masked by ceiling effects in higher-performing ones. Both subgroups produced essentially flat dose-response.
The broader literature has the same calibration problem. When small studies report positive tDCS effects in schizophrenia, those effects often disappear or shrink when subgroups are tested directly. The Ke design pre-specified the moderation test and found nothing.
Small tDCS Effects Shrink Across Recent Meta-Analyses
The optimistic narrative around tDCS for cognitive enhancement traces back to a wave of small positive trials in the 2010s. Recent systematic reviews and meta-analyses have tightened the picture in 3 ways:
- Working-memory effects were modest: Hill et al. 2016 meta-analyzed tDCS effects on working memory across healthy and neuropsychiatric populations and reported small-to-moderate effect sizes with substantial between-study heterogeneity.2
- Prefrontal stimulation was parameter-sensitive: Dedoncker et al. 2016 meta-analyzed prefrontal tDCS for cognitive function and similarly found heterogeneous, modest effects highly dependent on stimulation parameters and task design.5
- Single-session protocols looked weakest: The 2025 Safwi review and other recent meta-analyses cited in the Ke paper continued this trend. Single-session, single-target protocols increasingly read as a lower-bound test of tDCS efficacy, with the more durable signals (when present) coming from multi-session paradigms paired with cognitive training.3
Ke et al. therefore fit the direction of the newer evidence: a clean, pre-registered, sham-controlled test of one common single-session protocol found no acute working-memory improvement in schizophrenia.
Single-Session tDCS Is Not a Working-Memory Treatment Yet
- Single-session tDCS is not a clinical intervention for working-memory deficits in schizophrenia. Patients and families considering tDCS should know that one session over the right DLPFC produces no measurable acute cognitive benefit in this population.
- Multi-session paradigms remain the active research question. Repeated-session tDCS combined with cognitive training has produced more consistent (though still modest) effects in some trials. The Ke data say nothing about those protocols.
- Cognitive remediation therapy retains its evidence base. Despite being labor-intensive, structured cognitive remediation produces small-to-moderate effects on cognition and functioning in schizophrenia — an established alternative when scalable interventions are needed.6
- For tDCS researchers: pre-register, sham-control, and report full effect sizes. The Ke design is what good tDCS work in schizophrenia should look like — pre-registered moderation tests, formal power analysis, full reporting of post-hoc null follow-ups.
Dose, Target, Session Count, and Medication Status Remain Open
It tested one site, one dose, one duration, one task battery. Right DLPFC at 1.5 mA for 15 minutes is a common but not universal protocol. Left DLPFC, parietal targets, higher doses, longer durations, and combined-target protocols are not addressed.
It is single-session. Multi-session tDCS produces effects that single-session cannot, both because of cumulative neuroplastic change and because of pairing with cognitive training. The Ke null does not generalize to those paradigms.
The sample is small for detecting subtle effects. With 27 participants in a within-subject crossover, the trial is well-powered for moderate-to-large effects but not for small effects. Effects below approximately Cohen’s d = 0.5 cannot be reliably detected.
The participants were stable and medicated. All were on antipsychotics. Medication status, illness phase, and chronicity may modulate tDCS responsiveness in ways this design did not stratify on.
Offline assessment was used. Working memory was measured before and after stimulation, not during. Online tDCS effects (stimulation paired with task performance) sometimes produce larger acute effects than offline measurement captures.
Questions About tDCS for Working Memory in Schizophrenia
Should patients with schizophrenia try tDCS for cognitive symptoms?
The data do not support single-session tDCS as a clinical intervention for working memory in this population. Anodal tDCS over the right DLPFC produced no acute improvement compared to sham in this trial.1
Multi-session protocols paired with cognitive training are an active research area; whether they produce clinically meaningful benefit is not settled.
Why might tDCS work for some conditions but not for working memory in schizophrenia?
tDCS effects depend on baseline cortical state, network engagement during stimulation, and the specific cognitive process being targeted. Schizophrenia is associated with widespread network-level abnormalities that single-target stimulation may not adequately address.1
The Ke authors suggest that distributed network-based or multi-session approaches are more promising directions than single-session, single-target stimulation.
Is the Corsi Backward effect (p = 0.021) a real signal that more stimulation could amplify?
Probably not. The post-hoc analyses showed no significant pre-to-post change in either the anodal or sham condition.1
That pattern is consistent with random fluctuation producing a positive omnibus test rather than a true difference between conditions. With 4 working-memory tasks tested, one nominally significant result at p = 0.021 is roughly what chance produces.
What treatments do work for cognitive symptoms in schizophrenia?
Cognitive remediation therapy has the strongest evidence base for cognitive improvement in schizophrenia, with small-to-moderate effects on multiple cognitive domains and downstream functional outcomes.6
Antipsychotics produce mild benefit on cognition; some second-generation agents (e.g., lurasidone) may have modest cognitive advantages over alternatives. Exercise-based interventions and clozapine in treatment-resistant cases have additional emerging evidence.
References
- Anodal tDCS over right DLPFC does not improve visuospatial working memory in schizophrenia: a single-session, sham-controlled study. Ke SC et al. BMC Psychiatry. 2026. doi:10.1186/s12888-026-08107-9
- Effects of anodal transcranial direct current stimulation on working memory: a systematic review and meta-analysis of findings from healthy and neuropsychiatric populations. Hill AT, Fitzgerald PB & Hoy KE. Brain Stimulation. 2016;9(2):197-208. doi:10.1016/j.brs.2015.10.006
- Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Lefaucheur JP et al. Clinical Neurophysiology. 2017;128(1):56-92. doi:10.1016/j.clinph.2016.10.087
- Baseline neurocognitive deficits in the CATIE schizophrenia trial. Keefe RSE et al. Neuropsychopharmacology. 2006;31(9):2033-2046. doi:10.1038/sj.npp.1301072
- A systematic review and meta-analysis of the effects of transcranial direct current stimulation (tDCS) over the dorsolateral prefrontal cortex in healthy and neuropsychiatric samples: influence of stimulation parameters. Dedoncker J et al. Brain Stimulation. 2016;9(4):501-517. doi:10.1016/j.brs.2016.04.006
- Cognitive remediation for schizophrenia: an updated meta-analysis of randomized controlled trials. Vita A et al. JAMA Psychiatry. 2021;78(8):848-858. doi:10.1001/jamapsychiatry.2021.0620