A 2026 ALZAN memory-clinic cohort found that cerebrospinal-fluid alpha-synuclein seed amplification assay detected 19 of 20 Lewy body dementia cases, with 95% sensitivity and 93.5% specificity against non-Lewy-body, non-Alzheimer’s controls.1 The same assay was positive in 32 of 203 Alzheimer’s disease patients, which makes the result a co-pathology warning as much as a diagnostic win.
Research Highlights
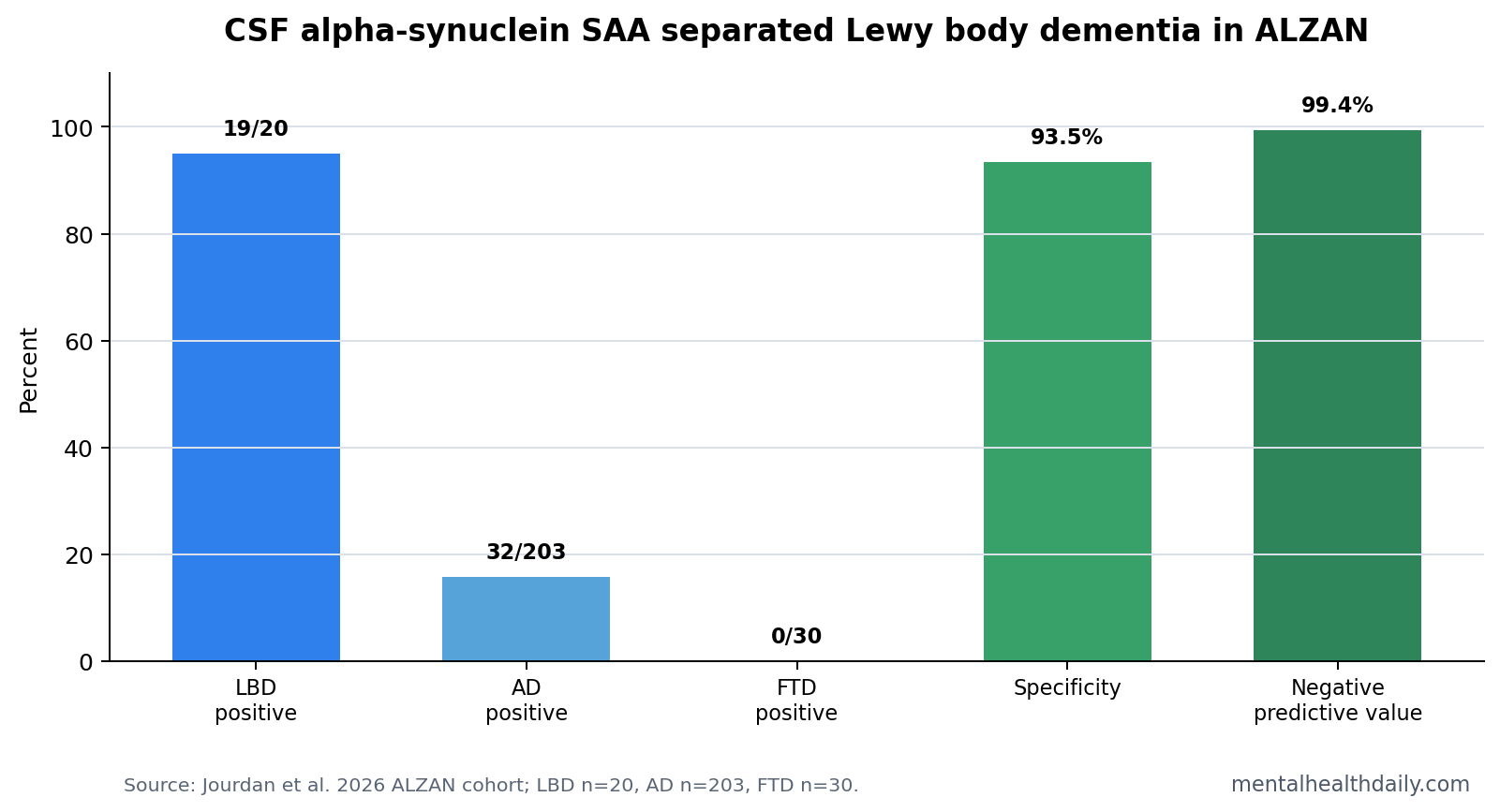
- LBD detection was strong: Alpha-synuclein SAA was positive in 19 of 20 Lewy body dementia patients, giving 95.0% sensitivity.1
- Specificity stayed high: Against a control group excluding Alzheimer’s disease and Lewy body dementia, specificity was 93.5% and the negative predictive value was 99.4%.1
- Alzheimer’s co-pathology was visible: The assay was positive in 32 of 203 Alzheimer’s disease patients, or 15.8%.1
- Blood biomarkers did not replace SAA: Within Alzheimer’s disease, alpha-synuclein-positive patients had lower CSF amyloid-beta 42/40 ratio, 4.6% vs. 5.2%, p = 0.0096, but no broad plasma-biomarker separation.1
- Preprint status limits certainty: The 398-person cohort is clinically useful but still needs peer review, longitudinal follow-up, and neuropathology-linked validation.1
Alpha-synuclein seed amplification assay is a laboratory test that tries to detect misfolded alpha-synuclein by making tiny pathological seeds grow into a measurable signal. In this study, researchers used real-time quaking-induced conversion (RT-QuIC), a method that shakes cerebrospinal-fluid samples with normal alpha-synuclein and flags samples that trigger abnormal aggregation.
The practical question is not whether the assay is interesting. It is whether it adds information in a real memory clinic, where Alzheimer’s disease, Lewy body dementia, frontotemporal dementia, mixed pathology, and nonspecific cognitive complaints often overlap.
Alpha-Synuclein SAA Was Positive in 95% of Lewy Body Dementia Cases
The ALZAN cohort enrolled 398 adults from memory clinics in Montpellier, Nimes, and Perpignan. Clinical diagnoses included 203 Alzheimer’s disease cases, 20 Lewy body dementia cases, 30 frontotemporal dementia cases, and 138 people in an “other” diagnostic group.
Alpha-synuclein SAA positivity separated Lewy body dementia sharply: 19 of 20 Lewy body dementia patients were positive, compared with 0 of 30 frontotemporal dementia patients and 11 of 138 patients in the other diagnostic group. Specificity was 93.5% when Alzheimer’s disease and Lewy body dementia were excluded from the control group.1
Clinical implication: a negative CSF SAA result may be especially useful for ruling against Lewy body dementia in this setting, because the negative predictive value reached 99.4%. That does not make it a stand-alone diagnosis. It makes it a strong biological input when the clinical picture is uncertain.
15.8% of Alzheimer’s Disease Patients Were SAA-Positive
Alzheimer’s disease was not a clean alpha-synuclein-negative comparator. Among 203 Alzheimer’s disease patients, 32 were SAA-positive, the same 15.8% positivity rate seen in the full 398-person cohort.1
That finding fits autopsy literature showing that older patients often carry more than one neurodegenerative pathology. Alzheimer’s disease can coexist with Lewy-body pathology, and mixed biology can blur clinical symptoms, progression patterns, hallucinations, sleep behavior, and cognitive fluctuations.
Within Alzheimer’s disease, SAA-positive patients did not show a clear cognitive split on Mini-Mental State Examination scores, 21.2 vs. 22.1 out of 30, p = 0.2707. Their CSF amyloid-beta 42/40 ratio was lower, 4.6% vs. 5.2%, p = 0.0096. The assay therefore found biological heterogeneity more clearly than it found an independent cognitive phenotype in this cross-sectional snapshot.
Plasma Alzheimer’s Biomarkers Did Not Capture Synuclein Co-Pathology
Plasma phosphorylated tau 217 performed well for Alzheimer’s disease detection in the cohort, with an AUC of 0.902. That is exactly why the SAA result is useful: strong Alzheimer’s blood markers do not automatically measure alpha-synuclein biology.
- Alzheimer’s signal: plasma p-tau217 and CSF amyloid markers captured Alzheimer’s disease biology.
- Synuclein signal: CSF SAA captured misfolded alpha-synuclein seeding activity.
- Mixed-pathology problem: the same patient can have both, so one biomarker family cannot substitute for the other.
Prior Parkinson’s disease work has pushed alpha-synuclein SAA toward biological disease classification.2 The ALZAN data move that question into routine cognitive clinics, where the test may help identify Lewy body dementia and detect synuclein co-pathology inside Alzheimer’s-labeled cases.
Routine-Clinic Performance Still Needs Longitudinal Validation
Evidence-strength note: the study is a multicenter prospective cohort, but it is also a medRxiv preprint and included only 20 Lewy body dementia patients. The result should be treated as promising clinical calibration, not a final diagnostic standard.
The biggest unanswered question is longitudinal. If an Alzheimer’s disease patient is SAA-positive today, does that predict faster cognitive decline, hallucinations, parkinsonism, REM sleep behavior disorder, or a different treatment response? The ALZAN cross-sectional data cannot settle that.
Why follow-up matters: a diagnostic biomarker is more useful when it changes prediction as well as classification. The ALZAN result shows that synuclein biology can be detected inside a memory-clinic workflow, but it does not yet show whether SAA-positive Alzheimer’s disease patients need different monitoring intervals, medication caution, caregiver counseling, or trial stratification.
Clinical Diagnosis Still Determines How the Assay Should Be Used
The assay is strongest when it is used to test a specific clinical uncertainty. Lewy body dementia is often suspected from fluctuating cognition, visual hallucinations, parkinsonism, REM sleep behavior disorder, autonomic symptoms, or neuroleptic sensitivity. In routine memory clinics, those features may be incomplete, late, or hidden by Alzheimer’s disease pathology.
High-value use case: a patient with cognitive impairment and borderline Lewy-body features. A positive SAA result would support synuclein biology and make clinicians look harder for hallucinations, sleep behavior disorder, autonomic symptoms, parkinsonism, medication sensitivity, and caregiver-reported fluctuations.
Lower-value use case: broad screening without a clinical question. The test can detect alpha-synuclein seeding, but it does not say whether the patient has dementia from Lewy bodies, Alzheimer’s disease with incidental synuclein co-pathology, Parkinson’s disease biology without dementia, or another mixed-pathology state.
The ALZAN data also argue against treating plasma p-tau217, GFAP, or amyloid markers as total dementia-biology coverage. Plasma p-tau217 can be excellent for Alzheimer’s disease, but it is not designed to identify Lewy-body pathology. A patient can have an Alzheimer’s-like blood profile and still carry a second neurodegenerative process.
SAA Kinetics May Be Informative, but the Binary Result Is Cleaner
Jourdan et al. also reported assay kinetic parameters among SAA-positive patients. Lewy body dementia patients had a shorter lag phase than Alzheimer’s disease patients, p = 0.0254, and a higher number of positive replicates, p = 0.0018. Fluomax and area did not differ significantly between clinical groups.
Lag phase is the time before the seeding reaction crosses the fluorescence threshold. A shorter lag phase can imply faster or more efficient seeding in the assay, but it is not a direct count of Lewy bodies in the brain. The researchers were careful on this point: kinetic parameters may reflect strain properties, seed concentration, or assay dynamics, not a simple severity scale.
For clinicians and readers, the binary result is currently easier to interpret than the kinetic details. Positive vs. negative SAA has direct diagnostic meaning. Lag phase and positive-replicate count are research-rich but not yet routine decision thresholds.
Mixed Pathology Is the Default Problem in Older Dementia Clinics
Neuropathology rarely respects clean textbook boundaries in older patients. Alzheimer’s amyloid and tau can coexist with Lewy-body pathology, vascular injury, TDP-43 pathology, hippocampal sclerosis, and other age-linked processes. That is why a single diagnosis often underdescribes the biology behind a patient’s symptoms.
The 15.8% SAA-positive rate in Alzheimer’s disease patients should be read through that lens. The better interpretation is biological incompleteness: the Alzheimer’s label may be accurate and still miss synuclein co-pathology in a subgroup.
Practical consequence: if SAA-positive Alzheimer’s disease patients later show hallucinations, fluctuating attention, REM sleep behavior disorder, parkinsonism, or antipsychotic sensitivity, the SAA result may help clinicians connect those symptoms to synuclein co-pathology instead of treating them as nonspecific late-stage dementia noise.
What Would Make SAA Ready for Broader Dementia Workups?
Broader use depends on 3 linked validations. First, laboratories need reproducible cutoffs across sample handling, reagent lots, and analysis pipelines. A seed amplification assay is powerful because it amplifies a pathological process, but that same amplification makes standardization important.
Second, clinicians need prospective outcome data. If SAA-positive Alzheimer’s disease patients develop Lewy-body symptoms more often over 2 to 5 years, the test becomes prognostic. If they do not, the result may still matter biologically but less for near-term clinical planning.
Third, treatment implications need to be explicit. A synuclein-positive result could affect antipsychotic caution, sleep-history collection, autonomic symptom screening, caregiver counseling, and research-trial selection. It should not automatically change Alzheimer’s disease medication or trigger unsupported disease-modifying claims.
Questions About Alpha-Synuclein SAA
Is alpha-synuclein SAA a blood test?
No. This ALZAN analysis used cerebrospinal fluid. Blood biomarkers were measured too, but they did not replace the synuclein-specific CSF assay.
Does a positive result mean Lewy body dementia?
Not by itself. A positive result means alpha-synuclein seeding activity was detected. In this cohort it was very common in Lewy body dementia, but it also appeared in 15.8% of Alzheimer’s disease cases.
What should readers take from the Alzheimer’s subgroup?
The strongest clinical use is mixed-pathology awareness. A patient can meet an Alzheimer’s disease profile and still carry synuclein biology that may affect symptoms and prognosis.
References
- Jourdan A, et al. Integrating alpha-Synuclein Seeding Activity (SAA) into routine practice: insights from the multicenter ALZAN Cohort. medRxiv. 2026. doi:10.64898/2026.04.21.26351389
- Siderowf A, et al. Assessment of heterogeneity among participants in the Parkinson’s Progression Markers Initiative cohort using alpha-synuclein seed amplification. Lancet Neurology. doi:10.1016/s1474-4422(23)00109-6
- Quadalti C, et al. Alpha-synuclein seed amplification assay and Alzheimer’s disease co-pathology. PubMed
- RT-QuIC alpha-synuclein diagnostic validation studies. PubMed