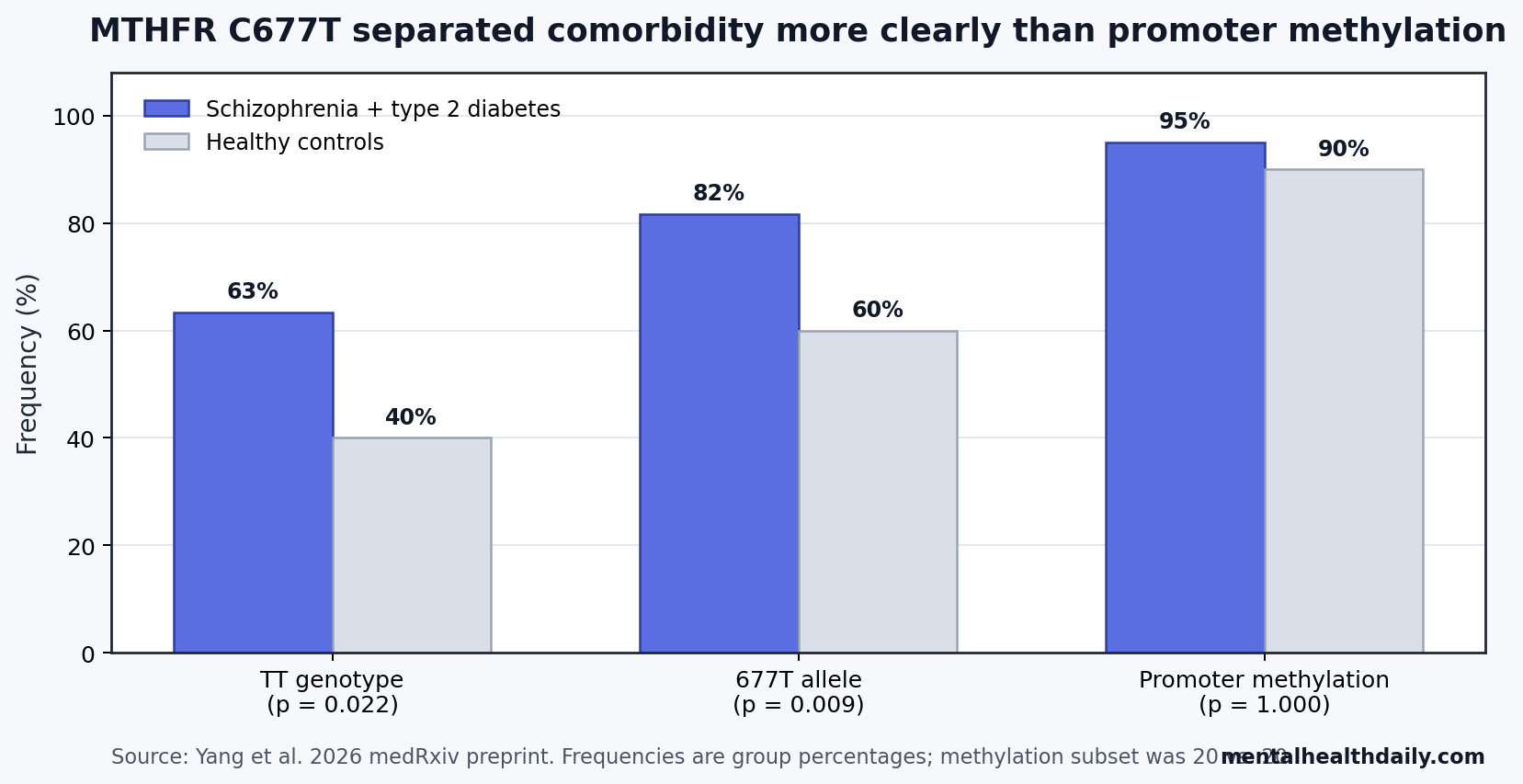
A 2026 Han Chinese case-control preprint linked the MTHFR C677T variant to schizophrenia with type 2 diabetes: the 677T allele appeared in 81.67% of alleles in the comorbid group vs. 60.00% in controls (p = 0.009), while MTHFR promoter methylation was nearly saturated in both groups (95.00% vs. 90.00%; p = 1.000).
Research Highlights
- Genetic signal was the headline: In 120 Han Chinese participants, the MTHFR 677T allele was more frequent in schizophrenia with type 2 diabetes than in controls (81.67% vs. 60.00%; p = 0.009). [1]
- TT genotype was enriched: The comorbid group had 63.33% TT genotype frequency vs. 40.00% in controls, with no CC genotypes observed among 30 comorbid patients. [1]
- Methylation did not separate groups: MTHFR promoter methylation was 95.00% in comorbid patients and 90.00% in controls, with a very wide 95% confidence interval around the estimate. [1]
- Prior evidence fits the direction: Meta-analytic work has separately linked schizophrenia to type 2 diabetes risk and MTHFR C677T to psychiatric or metabolic susceptibility. [2] [3] [4]
- Clinical use is premature: The 2026 result came from 30 people per group, only 20 methylation-tested comorbid cases, and a preprint design that cannot prove causality or justify screening. [1]
Methylenetetrahydrofolate reductase (MTHFR) is an enzyme in one-carbon metabolism, the folate-dependent chemical pathway that helps recycle homocysteine into methionine and supports methylation reactions across the body. The common C677T variant, also called rs1801133, can reduce enzyme activity and raise homocysteine, a sulfur-containing amino acid linked to vascular, metabolic, and neuropsychiatric biology.
The result is narrow and directional: Yang et al. found a stronger allele/genotype signal than a promoter-methylation signal in one comorbid schizophrenia-diabetes cohort. That pattern fits older MTHFR and homocysteine literature, but it does not turn C677T into a diagnostic test for metabolic risk in schizophrenia.
MTHFR 677T Was Enriched in Schizophrenia With Type 2 Diabetes
Yang et al. enrolled 120 Han Chinese participants from Liaocheng Fourth People’s Hospital in Shandong Province between January 2025 and June 2025. The design used 4 equal groups: 30 with schizophrenia, 30 with type 2 diabetes, 30 with schizophrenia plus type 2 diabetes, and 30 healthy controls. [1]
Schizophrenia was defined using DSM-5 criteria, with at least 2 years of illness and stable oral antipsychotic doses for at least 6 months. Type 2 diabetes was defined by fasting plasma glucose of at least 7.0 mmol/L or 2-hour postprandial glucose of at least 11.1 mmol/L, matching standard diabetes thresholds used in the study protocol.
The strongest comparison was the comorbid schizophrenia plus type 2 diabetes group vs. healthy controls:
- TT genotype: 63.33% in the comorbid group vs. 40.00% in controls.
- CT genotype: 36.67% in the comorbid group vs. 40.00% in controls.
- CC genotype: 0.00% in the comorbid group vs. 20.00% in controls.
- 677T allele: 81.67% in the comorbid group vs. 60.00% in controls.
Genotype frequencies differed at p = 0.022, and allele frequencies differed at chi-square = 6.817, p = 0.009. Across all 4 groups, allele frequencies also differed significantly (p = 0.009), with the T allele at 58.33% in schizophrenia only, 76.67% in type 2 diabetes only, 81.67% in the comorbid group, and 60.00% in controls. [1]
Promoter Methylation Was High in Both Groups
Promoter methylation means chemical tagging near a gene’s control region, often reducing how strongly that gene is expressed. In this study, methylation-specific PCR classified MTHFR promoter status as unmethylated only, hemimethylated, or fully methylated.
That epigenetic comparison was much less persuasive than the genotype comparison. Yang et al. tested methylation in 20 comorbid patients and 20 controls, not all 120 enrolled participants.
Combined methylation was 95.00% in the comorbid group and 90.00% in controls (p = 1.000; OR = 0.474; 95% CI 0.039-5.688). Full methylation was numerically higher in comorbid patients, 90.00% vs. 60.00%, but the reported comparison was also nonsignificant (p = 0.781; OR = 0.333; 95% CI 0.027-4.098). [1]
The wide confidence intervals matter because they show how little precision the methylation subset had. A 20-vs.-20 assay can miss moderate effects, especially when methylation is already common in both groups. The safer interpretation is that this specific qualitative assay did not demonstrate a methylation difference, while the genotype signal was clearer.
Yang et al. found a stronger C677T allele/genotype signal than a promoter-methylation signal in the comorbid schizophrenia and type 2 diabetes group.
Folate Metabolism Gives the Finding Biological Plausibility
The MTHFR C677T variant changes the enzyme’s structure and can reduce its activity. Yang et al. cite prior estimates that TT genotype may reduce MTHFR activity by around 75%, while CT genotype may reduce activity by around 34%. [1] Less MTHFR activity can increase homocysteine and disturb folate-dependent methylation chemistry.
That mechanism is plausible because schizophrenia and type 2 diabetes already overlap through several biological routes:
- Homocysteine and schizophrenia: Nishi et al. meta-analyzed blood homocysteine and MTHFR C677T studies in schizophrenia, supporting a folate-homocysteine axis as one candidate pathway rather than a standalone cause. [5]
- Schizophrenia and diabetes risk: Dong et al. reviewed and meta-analyzed schizophrenia and type 2 diabetes risk, giving the comorbidity question a broader epidemiologic base. [2]
- MTHFR and diabetes susceptibility: Meng et al. meta-analyzed MTHFR C677T and type 2 diabetes susceptibility, while Liu et al. reported MTHFR polymorphism associations in a Yunnan Province type 2 diabetes sample. [4] [6]
- Insulin signaling: Zhang et al. reported that homocysteine can impair pro-insulin receptor cleavage and cause insulin resistance through protein cysteine-homocysteinylation, a molecular route that could connect folate metabolism to glucose control. [7]
None of those papers proves that MTHFR C677T causes diabetes in schizophrenia. Together, they make Yang et al.’s result less isolated: the variant sits in a pathway with credible links to homocysteine, methylation biology, vascular function, insulin signaling, and brain chemistry.
The Preprint Cannot Separate Genetic Risk From Treatment and Environment
Schizophrenia plus type 2 diabetes is rarely a pure genetic phenotype. Antipsychotic exposure, diet, activity, smoking, sleep, socioeconomic factors, illness duration, access to medical care, and family history can all shape metabolic risk.
Yang et al. matched or compared age, sex, education, smoking, and drinking history across groups, but the paper did not directly model antipsychotic type, dose, duration, weight trajectory, diet, folate intake, homocysteine concentration, or MTHFR enzyme activity. [1]
Evidence-strength note: this was a small case-control preprint. The result supports association, not causation. It also cannot show whether MTHFR C677T increases diabetes risk after schizophrenia, increases schizophrenia risk among people prone to diabetes, marks a broader ancestry-linked haplotype, or simply travels with unmeasured environmental exposures in this sample.
Population specificity is another limit. MTHFR allele frequencies vary across ancestry groups, and the 2026 cohort came from a single Han Chinese hospital population. A result that holds in northern Han Chinese inpatients may weaken, strengthen, or reverse in other Chinese regions, other ancestries, outpatient schizophrenia cohorts, or first-episode patients with shorter antipsychotic exposure.
Clinical Screening Needs Replication, Not Immediate MTHFR Testing
MTHFR testing already attracts oversized claims in wellness and psychiatric genetics. Yang et al. do not provide the kind of evidence needed for a clinical screening rule. A useful biomarker would need replication in larger cohorts, clear predictive value beyond ordinary metabolic risk factors, and evidence that the test changes care.
For schizophrenia care, the immediate metabolic priorities remain more practical:
- Baseline monitoring: weight, waist circumference, fasting glucose or HbA1c, lipids, blood pressure, and family history before or soon after antipsychotic initiation.
- Medication context: antipsychotic selection and switching decisions should account for metabolic liability, psychiatric stability, and relapse risk.
- Modifiable biology: folate status, B12 status, homocysteine, smoking, activity, and diet are testable or addressable without using C677T genotype as a shortcut.
- Research next step: larger prospective cohorts should test whether C677T predicts incident diabetes after controlling for antipsychotic exposure, body weight, diet, folate, and baseline metabolic risk.
The 2026 preprint is useful because it points to a specific candidate pathway in a clinically important comorbidity. It becomes weaker when treated as a ready-made test. The genetic signal deserves replication; the methylation result mostly says that this assay, in this small subset, did not carry the same signal.
Questions About MTHFR, Schizophrenia, and Type 2 Diabetes
Does this mean MTHFR C677T causes diabetes in schizophrenia?
No. The 2026 study found an association between C677T genotype/allele frequency and the comorbid schizophrenia plus type 2 diabetes group. A case-control design cannot determine whether the variant caused diabetes, contributed to schizophrenia biology, marked another genetic background, or reflected unmeasured clinical factors.
Was promoter methylation completely irrelevant?
The study did not demonstrate a significant promoter-methylation difference. That is narrower than saying methylation is irrelevant. The methylation subset was small, the assay was qualitative, and only one promoter region was tested.
Should people with schizophrenia get MTHFR testing because of this paper?
No. The result is preprint-level association evidence from one 120-person cohort. Routine metabolic monitoring in schizophrenia has much stronger clinical justification than MTHFR testing.
What would make the genetic finding more convincing?
Replication in larger, multi-center cohorts would help most. The strongest next design would follow schizophrenia patients over time, measure antipsychotic exposure and metabolic variables, assay homocysteine and folate status, and test whether C677T predicts new-onset type 2 diabetes beyond standard risk factors.
References
- Yang C, Li R, Wang X, et al. MTHFR C677T polymorphism and promoter methylation in schizophrenia patients with type 2 diabetes mellitus: evidence from a Han Chinese cohort. medRxiv. 2026. doi:10.64898/2026.04.09.26350471
- Dong K, Wang S, Qu C, Zheng K, Sun P. Schizophrenia and type 2 diabetes risk: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2024;15:1395771. doi:10.3389/fendo.2024.1395771
- Zhang YX, Yang LP, Gai C, et al. Association between variants of MTHFR genes and psychiatric disorders: a meta-analysis. Front Psychiatry. 2022;13:976428. doi:10.3389/fpsyt.2022.976428
- Meng Y, Liu X, Ma K, et al. Association of MTHFR C677T polymorphism and type 2 diabetes mellitus susceptibility. Mol Genet Genomic Med. 2019;7(12):e1020. doi:10.1002/mgg3.1020
- Nishi A, Numata S, Tajima A, et al. Meta-analyses of blood homocysteine levels for gender and genetic association studies of the MTHFR C677T polymorphism in schizophrenia. Schizophr Bull. 2014;40(5):1154-1163. doi:10.1093/schbul/sbt154
- Liu Y, Pu G, Yang C, et al. Association analysis of MTHFR (rs1801133 and rs1801131) gene polymorphism towards the development of type 2 diabetes mellitus in Dali area population from Yunnan Province, China. PeerJ. 2024;12:e18334. doi:10.7717/peerj.18334
- Zhang X, Qu YY, Liu L, et al. Homocysteine inhibits pro-insulin receptor cleavage and causes insulin resistance via protein cysteine-homocysteinylation. Cell Rep. 2021;37(2):109821. doi:10.1016/j.celrep.2021.109821