Auditory targeted memory reactivation during a 2-hour nap did not improve motor retention in 20 Parkinson’s disease patients or 20 healthy older adults, even though the same cues changed sleep physiology by reducing spindle density and increasing slow-wave density.1
Research Highlights
- First Parkinson’s TMR test: Micca et al. studied 20 Parkinson’s disease patients and 20 healthy older adults after motor sequence learning, then replayed one learned auditory sequence during NREM2/NREM3 sleep in a 2-hour nap.1
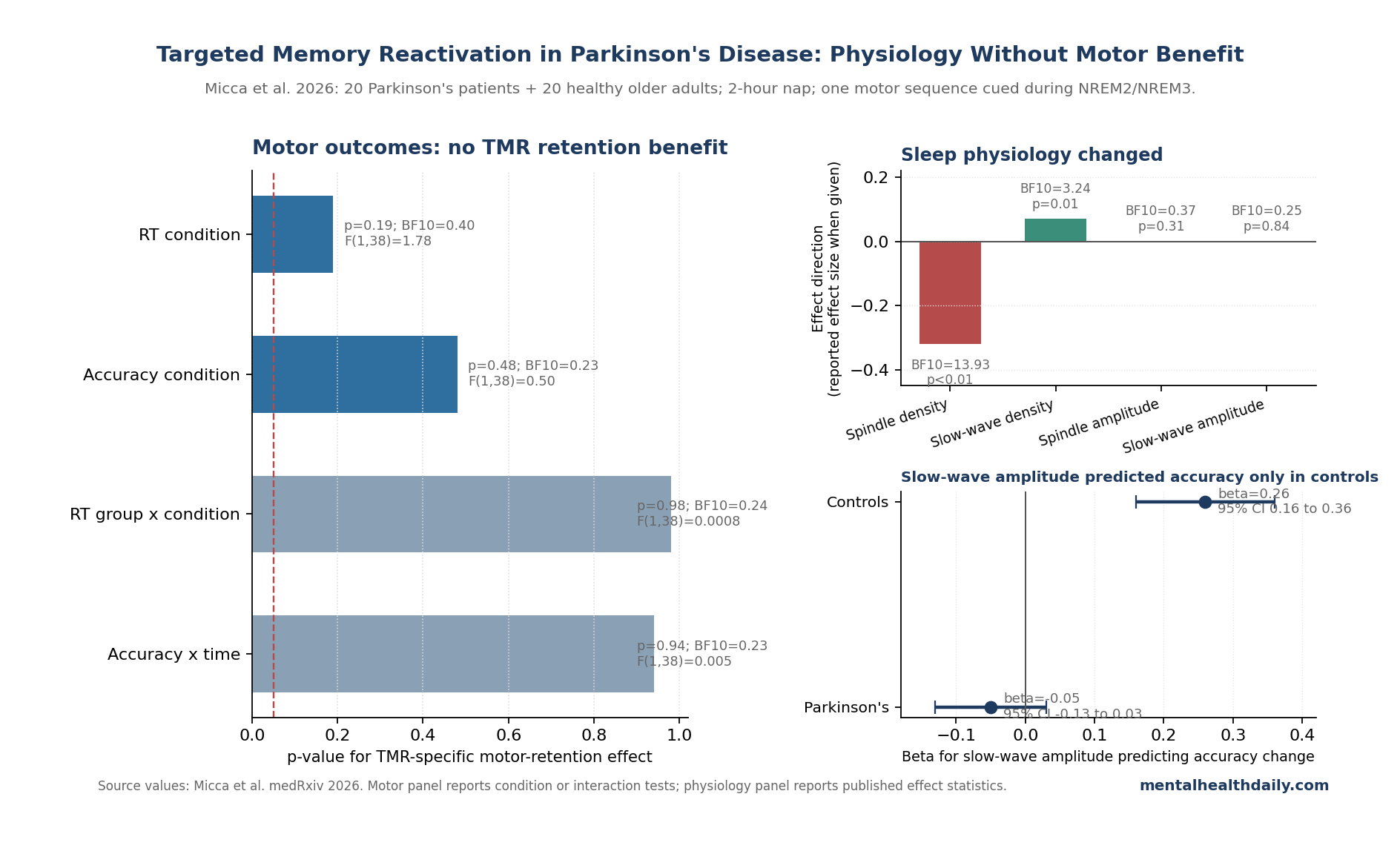
- No motor-retention advantage: the reactivated sequence did not outperform the non-reactivated sequence for reaction time (F(1,38) = 1.78, p = 0.19; BF10 = 0.40) or accuracy (F(1,38) = 0.50, p = 0.48; BF10 = 0.23).1
- Dual-tasking stayed null too: TMR did not improve automaticity immediately after the nap or at 24-hour retention, so the null was not limited to the simple single-task test.1
- Sleep physiology did move: auditory cues reduced spindle density (F(1,34) = 10.49, p < 0.01; BF10 = 13.93) and increased slow-wave density (F(1,31) = 6.87, p = 0.01; BF10 = 3.24).1
- The physiology-behavior link split by group: slow-wave amplitude predicted accuracy change in healthy older adults (β = 0.26, 95% CI 0.16 to 0.36), but not in Parkinson’s disease (β = -0.05, 95% CI -0.13 to 0.03).1
Targeted memory reactivation (TMR) means pairing a sound, smell, or other sensory cue with learning while awake, then replaying that cue during sleep to reactivate the memory trace. The attractive Parkinson’s version is simple: pair a melody with motor-sequence practice, replay the melody during NREM sleep, and see whether the sleeping brain strengthens the trained movement.
The Micca result separates 2 claims that often get blurred. Auditory cues can perturb sleep oscillations in Parkinson’s disease, but this experiment did not show that cueing improves motor learning, 24-hour retention, or dual-task automaticity.
Why Parkinson’s Disease Was a Plausible Target
Parkinson’s disease damages dopaminergic circuits that support motor learning, especially the basal-ganglia loops involved in automaticity and long-term skill retention. Rehabilitation depends on practice, but practice gains do not always consolidate cleanly into durable performance.
Sleep was a reasonable place to look for leverage. NREM sleep contains slow waves, sleep spindles, and hippocampal-cortical replay signals that help stabilize newly learned information.
Earlier TMR studies in younger adults reported motor-memory benefits, and Hu et al. pooled a broader literature showing that cueing during sleep can improve later memory under some conditions.2,3
Older adults and Parkinson’s patients are a harder test. Aging changes slow-wave and spindle timing, Parkinson’s disease alters sleep architecture, and motor rehabilitation involves cortico-striatal circuits that may not respond to cueing the way declarative memory does.
Micca 2026 Tested 2 Sequences During a 2-Hour Nap
Micca et al. enrolled 20 people with Parkinson’s disease and 20 healthy older adults. Participants practiced 2 bimanual serial reaction time task sequences before a nap.
Each sequence was paired with a distinct 8-tone melody during practice.
During the 2-hour nap, researchers replayed only 1 of the 2 melodies during online-scored NREM2 and NREM3 sleep. That created a within-person comparison: the reactivated sequence vs. the non-reactivated sequence.
The study measured several outcomes:
- Immediate retention: performance after waking, 30 to 40 minutes after the nap opportunity.
- 24-hour retention: performance the next day after home sleep.
- Dual-task automaticity: sequence performance while participants also counted visual squares.
- Sleep electrophysiology: spindle density, slow-wave density, amplitude, frequency, and slow-wave/spindle coupling during cue and silence periods.
The Parkinson’s cohort had mild-to-moderate disease severity: median Hoehn and Yahr stage 2 in the ON-medication state, mean MDS-UPDRS III ON score 26.4, and worse subjective sleep than controls. Objective nap time was similar across groups, around 94 minutes of total sleep in both groups.1
TMR Did Not Improve Motor Retention
The behavioral result was not subtle: reactivated sequences did not consolidate better than non-reactivated sequences.
Reaction-time retention improved over time overall, but the improvement was not specific to TMR. The condition effect was not significant (F(1,38) = 1.78, p = 0.19; BF10 = 0.40), and the group-by-condition interaction was effectively absent (F(1,38) = 0.0008, p = 0.98; BF10 = 0.24).
Accuracy showed the same pattern: condition F(1,38) = 0.50, p = 0.48; BF10 = 0.23.1
Dual-task results were also null. The cue did not make the reactivated sequence more automatic immediately after the nap or at 24 hours.
That matters for rehabilitation because Parkinson’s disability is more than about performing a practiced movement in isolation; daily movement often requires maintaining performance while attention is divided.
The Cues Changed Sleep, Not Motor Learning
The sleep data are why the trial should not be read as “TMR did nothing.” The sleeping brain responded to the auditory cues, but the response did not become a behavioral advantage.
During TMR periods, spindle density decreased with strong Bayesian support (BF10 = 13.93; F(1,34) = 10.49, p < 0.01; Cohen’s d = 0.32). Slow-wave density increased with more moderate support (BF10 = 3.24; F(1,31) = 6.87, p = 0.01).
These effects appeared in both Parkinson’s disease and healthy older adults, with no meaningful group interaction.1
Amplitude was different. TMR did not significantly change spindle amplitude (F(1,34) = 1.08, p = 0.31; BF10 = 0.37) or slow-wave amplitude (F(1,31) = 0.05, p = 0.84; BF10 = 0.25).
Phase-amplitude coupling also did not separate cue periods from silence periods, and coupling was not associated with post-nap performance change.
Slow-Wave Amplitude Helped Controls, Not Parkinson’s Patients
The most interesting positive signal was not the main treatment effect. Slow-wave amplitude during TMR periods predicted accuracy improvement for the reactivated sequence in healthy older adults, but not in Parkinson’s disease.
The group-by-slow-wave-amplitude interaction was strong (BF10 = 29.24; F(1) = 22.87, p < 0.01). In healthy older adults, the slope was positive (β = 0.26, 95% CI 0.16 to 0.36).
In Parkinson’s disease, it was negative and not significant (β = -0.05, 95% CI -0.13 to 0.03).1
That pattern makes the mechanistic interpretation sharper. TMR may be capable of engaging a slow-wave-linked consolidation pathway in older adults, but Parkinson’s disease may break the downstream link between cue-evoked slow-wave activity and motor-memory benefit.
Broader TMR Literature Evidence
Young-adult motor-memory TMR studies have often been more optimistic. Antony et al. reported that cueing during sleep improved skill learning, and later work linked successful cueing to slow-wave/spindle coordination.3
Older-adult motor TMR has been less consistent. Nicolas et al. found no behavioral benefit on a motor sequence learning task in healthy older adults, while auditory stimulation still altered slow-wave/spindle coupling.4
The Micca Parkinson’s trial now lands close to that older-adult pattern: physiological modulation without a reliable behavioral payoff.
Parkinson’s sleep-motor work also argues against overreading a single nap result. Lanir-Azaria et al. and Micca et al.’s earlier nap study show that sleep can interact with motor sequence learning in Parkinson’s disease, but that does not establish a single auditory cueing session can rescue retention.5,6
Limits of the Parkinson’s Sleep-Cue Trial
Several caveats keep the result from closing the file on sleep-based rehabilitation:
- Preprint status: the paper is posted on medRxiv and has not been peer reviewed.
- Small sample: 20 participants per group is useful for a first test, but too small for confident moderator analysis.
- Nap design: a 2-hour afternoon nap is not the same intervention as full-night or multi-night TMR.
- ON-medication testing: Parkinson’s patients were tested in their usual medication-on state, which may reduce visible group differences and does not answer overnight OFF-state questions.
- No wake-control group: the trial compared reactivated and non-reactivated sequences during sleep, but did not directly compare sleep cueing with wake cueing.
- Task specificity: the serial reaction time task may not expose the same deficits as gait, balance, handwriting, or other rehabilitation-relevant skills.
The melody design may also matter. The 2 learned sequences used the same tones in different orders, so the cue may have been too similar across memories to create clean sequence-specific reactivation.
What Parkinson’s Rehabilitation Can Take From This
The practical read is narrow and useful: auditory TMR during one nap is not ready as a Parkinson’s motor-rehabilitation add-on. The tested cueing protocol changed sleep biomarkers, but it did not improve the trained movement.
Future trials should probably avoid treating “sleep changed” as the outcome. The harder question is whether a sleep intervention changes gait, balance, handwriting, daily function, or other patient-relevant motor outcomes.
Multi-night cueing, full-night protocols, better-separated auditory cues, OFF-medication testing, and more demanding motor tasks are all reasonable next tests.
For now, Parkinson’s sleep care should stay grounded in established clinical targets: sleep apnea, REM sleep behavior disorder, insomnia, medication-timing sleep disruption, daytime sleepiness, and nocturnal motor symptoms. TMR remains an interesting experimental probe of sleep-memory physiology, not a proven way to strengthen Parkinson’s motor learning.
Questions About TMR, Sleep, and Parkinson’s Disease
How did Micca et al. use targeted memory reactivation during the nap?
Researchers paired each motor sequence with an 8-tone melody during practice, then replayed only 1 melody during NREM2/NREM3 sleep. That made the cued sequence the reactivated memory and the uncued sequence the within-person control.1
Did the Parkinson’s patients fail to learn the task?
No. Parkinson’s patients learned more slowly than healthy older adults during initial acquisition, but both groups improved over time.
The specific failure was that TMR did not make the cued sequence improve more than the uncued sequence.1
Why do slow waves and spindles matter?
Slow waves are large NREM oscillations linked to cortical down-state/up-state cycling. Spindles are 10 to 16 Hz thalamocortical bursts.
Their timing is thought to help coordinate memory replay, but this study shows that changing density is not enough to guarantee better motor retention.1
Does this mean sleep cannot help Parkinson’s motor learning?
No. The result is specific to auditory TMR during a single nap after a serial reaction time task.
It does not rule out ordinary sleep quality, full-night sleep interventions, closed-loop stimulation, or different motor tasks.
Is TMR proven in other populations?
The broader TMR literature contains positive findings, especially in younger adults and some declarative-memory paradigms, but effects vary by age, task, cue type, and sleep physiology.2,3
What is the next Parkinson’s study?
A stronger next test would use larger samples, full-night or multi-night cueing, clearer cue discrimination, OFF-medication measurement, and rehabilitation-relevant outcomes such as gait, balance, or handwriting rather than only finger-tapping sequence retention.
References
- Micca L, Albouy G, King BR, et al. Targeted memory reactivation during sleep modulates spindle and slow wave density, but not motor memory consolidation, in Parkinson’s disease. medRxiv. 2026. doi:10.64898/2026.04.22.26351552
- Hu X, Cheng LY, Chiu MH, Paller KA. Promoting memory consolidation during sleep: a meta-analysis of targeted memory reactivation. Psychological Bulletin. 2020;146(3):218-244. doi:10.1037/bul0000223
- Antony JW, Gobel EW, O’Hare JK, Reber PJ, Paller KA. Cued memory reactivation during sleep influences skill learning. Nature Neuroscience. 2012;15(8):1114-1116. doi:10.1038/nn.3152
- Nicolas J, Carrier J, Swinnen SP, Doyon J, Albouy G, King BR. Targeted memory reactivation in older adults modulates slow wave-spindle coupling but not motor sequence learning. Journal of Sleep Research. 2024;33(2):e14027. doi:10.1111/jsr.14027
- Lanir-Azaria S, Chishinski R, Tauman R, Nir Y, Giladi N. Sleep improves motor sequence learning in Parkinson’s disease. Frontiers in Behavioral Neuroscience. 2024;18:1466696. doi:10.3389/fnbeh.2024.1466696
- Micca L, Gilat M, Borzee P, et al. The effect of a post-learning nap on motor memory consolidation in Parkinson’s disease. NPJ Parkinson’s Disease. 2025. doi:10.1111/jsr.70203