A 70-person COPD trial found that 12 weeks of app-based rhythm-guided walking plus singing improved shuttle-walk distance by 56.35 m and lowered HADS-anxiety by 2.31 points vs. usual care; rhythm-guided walking without singing did not clearly separate from usual care.1
Research Highlights
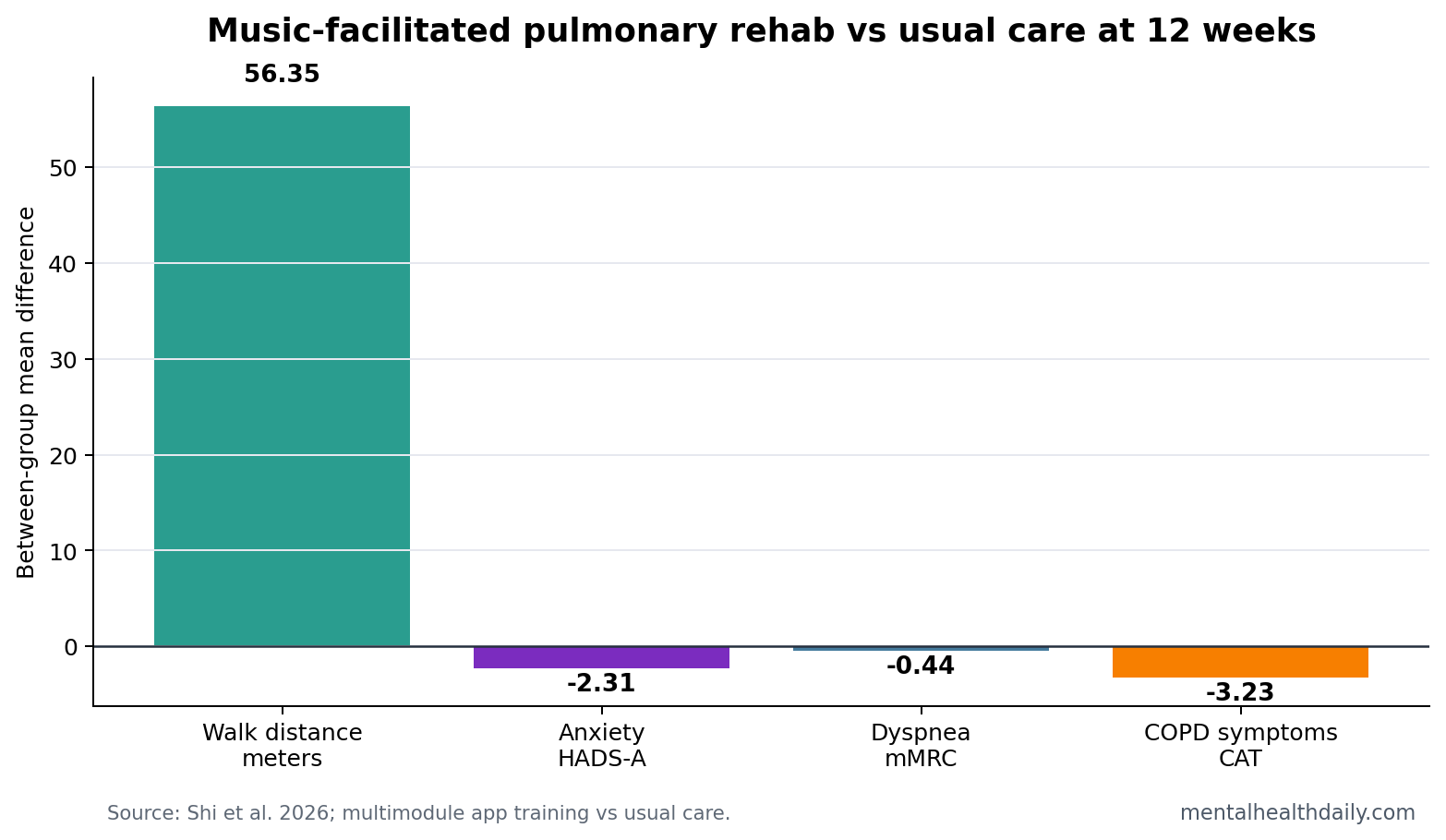
- Combined training beat usual care: the multimodule group improved incremental shuttle walking test distance by 56.35 m vs. usual care at 12 weeks (95% CI 6.66 to 106.04; p = .03).1
- Anxiety moved more than depression: Hospital Anxiety and Depression Scale-anxiety scores were 2.31 points lower vs. usual care (95% CI -3.99 to -0.63; p = .008), while depression was not the headline signal.1
- Walking tempo alone was not enough: the rhythm-guided walking group did not show significant differences from usual care on the primary or secondary outcomes in the 70-person trial.1
- Breathing and symptom burden improved together: the combined program lowered mMRC dyspnea by 0.44 points and COPD Assessment Test scores by 3.23 points vs. usual care.1
- Evidence is promising but small: 55 of 70 randomized participants completed 12-week follow-up, so the result is best read as an early digital-rehab signal, not proof of durable mental-health benefit.1
Chronic obstructive pulmonary disease (COPD) is a progressive respiratory disease that causes airflow limitation, breathlessness, fatigue, and activity restriction. Anxiety is not an unrelated side complaint. Breathlessness can feel threatening, activity becomes avoidant, sleep worsens, and patients can begin to organize daily life around fear of dyspnea.
Pulmonary rehabilitation is structured exercise, education, breathing support, and behavior-change coaching for chronic lung disease. The standard model works, but clinic-based programs are hard to reach for many patients because of travel, staffing, cost, and symptom burden.2
Shi et al. tested a home-delivered version with a narrower question: can a smartphone app make pulmonary rehabilitation more accessible, and does adding music-linked components change symptoms beyond education and walking guidance alone?1
Rhythm-Guided Walking Plus Singing Improved 12-Week Function
The randomized trial assigned 70 adults with COPD in China to 3 groups: multimodule training, rhythm-guided walking, or usual care. The multimodule group used a smartphone app for rhythm-guided walking plus singing training. The walking-only group used the app for rhythm-guided walking. All groups received structured patient education.
Incremental shuttle walking test distance was the primary endpoint. It measures how far a person can walk while speed increases in stages, so it captures exercise capacity more directly than a questionnaire. At 12 weeks, the combined music-facilitated pulmonary-rehab program beat usual care by 56.35 m.
The effect size was modest in standardized terms (Cohen d = 0.30), but the direction was clinically coherent. Dyspnea, symptom burden, anxiety, and inspiratory capacity moved in the same general direction. The trial did not show that the app cured COPD-related distress. It showed that the combined package made enough functional difference to register across several patient-facing endpoints.
- Participants: 70 randomized adults with COPD, mean age 64.3 years.
- Intervention length: 12 weeks of asynchronous home-based app training.
- Primary endpoint: incremental shuttle walking distance at week 12.
- Completion: 55 of 70 participants completed the 12-week follow-up.
Anxiety Improved More Clearly Than the Walking-Only Arm
HADS-anxiety is the anxiety subscale of the Hospital Anxiety and Depression Scale, a symptom measure often used in medically ill populations because it avoids some physical symptoms that overlap with disease burden. The multimodule group scored 2.31 points lower than usual care at 12 weeks.
That anxiety result fits the intervention’s structure. Singing can train breath control, pacing, and confidence with respiratory sensations. Rhythm-guided walking can make activity more predictable. The smartphone app can reduce friction by moving the program into the home. Together, those pieces target the loop in which breathlessness increases fear and fear reduces activity.
The walking-only arm is the calibration point. Rhythm-guided walking alone did not significantly separate from usual care on primary or secondary outcomes. If forced to choose a mechanistic explanation, lean toward the combined package: exercise pacing plus singing-based breathing practice plus education, not rhythm as a stand-alone active ingredient.
Music Is a Rehab Delivery Tool, Not a COPD Anxiety Treatment by Itself
Mechanism: music-assisted pulmonary work can sound softer than the disease warrants, but the practical mechanism is not vague mood enhancement.
- Singing: controlled exhalation, respiratory timing, vocal effort, posture, and tolerance of breath sensations.
- Rhythm-guided walking: exercise pacing through an external cue rather than constant self-monitoring.
Prior pulmonary-rehabilitation guidance already treats exercise and behavior change as central COPD care.2 Singing-for-lung-health studies add a plausible respiratory and confidence pathway, although evidence has generally been smaller and more heterogeneous than conventional rehabilitation evidence.4
Reader-level translation: the 2026 trial is not evidence that listening to music lowers COPD anxiety. The active program required scheduled rehabilitation sessions, walking, singing practice, and education through an app. Music was part of the training architecture.
Small Trial Design Limits the Mental-Health Claim
Evidence-strength note: this was a 70-person randomized trial with a 12-week endpoint. Anxiety was a secondary outcome. The trial can support a short-term signal that multimodule app-based rehabilitation improved anxiety vs. usual care, but it cannot prove durable psychiatric benefit, reduced medication use, fewer exacerbations, or lower hospitalization risk.
The usual-care comparison sharpens interpretation. Structured education was present in all groups, but the multimodule group received more active training time and a more engaging intervention. That is not a flaw; real rehabilitation programs are packages. It does mean the trial cannot isolate singing, rhythm, app design, therapist contact, and adherence as separate causal ingredients.
Attrition leaned against easy certainty. Follow-up completion was lower in usual care than in the active app groups, and only 55 participants completed week 12. A larger trial should test whether the anxiety signal persists, whether people with high baseline anxiety benefit more, and whether digital rehabilitation reaches patients who would not attend clinic-based programs.
Adherence question: the active app groups had more built-in reasons to return: rhythm cues, singing practice, scheduled progression, symptom feedback, and a sense that the program was doing more than giving generic exercise advice. That engagement difference may be part of the treatment effect, but it also means future trials should report session completion, singing adherence, walking minutes, and reasons for dropout by group.
Where This Fits in COPD Mental-Health Care
COPD anxiety care usually has to solve 2 problems at once. The first is fear of breathlessness itself. The second is the behavioral narrowing that follows: less walking, fewer social activities, more symptom checking, and a smaller physical world. A digital rehab program is most useful when it interrupts that narrowing through repeated safe practice.
Best-case role: app-based music pulmonary rehab becomes a reachable first layer for patients who are not attending formal rehabilitation. The program gives them a structured way to move, breathe, sing, and monitor symptoms at home while clinicians decide who needs higher-touch care.
Wrong role: treating the app as a psychiatric replacement. A COPD patient with panic attacks, major depression, trauma symptoms, severe insomnia, or suicidal thinking needs direct mental-health assessment. The trial’s anxiety score improvement is compatible with better breath control and confidence; it is not evidence that the intervention can handle full psychiatric complexity on its own.
A larger pragmatic trial should measure baseline anxiety severity, rescue medication use, attendance, app adherence, exacerbations, and whether the intervention reaches rural or mobility-limited patients who would otherwise receive education only. Those endpoints would separate access benefit from pure treatment effect.
The useful clinical stance is therefore conditional optimism: try the combined rehab logic when access and safety allow, but keep formal anxiety care available for patients whose fear is larger than breathlessness training can explain.
Access benchmark: formal pulmonary rehabilitation is already recommended because it improves exercise capacity and symptom burden, but many patients never reach a clinic-based program.2 A smartphone version should be judged partly by whether it brings structured practice to people who would otherwise receive education alone, with supervised-rehabilitation matching treated as a separate ideal-setting benchmark.
The mental-health angle should stay tied to breathlessness behavior. If the program lowers anxiety by making dyspnea feel more predictable and movement feel safer, that is still clinically useful. It also means the best candidates may be patients whose fear rises during exertion, not patients whose anxiety is independent of COPD symptoms.
Clinicians should also watch for patients who need both tracks. A person can benefit from breathing-linked rehabilitation and still need psychotherapy, medication review, sleep care, or panic-focused treatment. The app signal is strongest as an access and practice tool inside COPD care.
Questions About Music Pulmonary Rehab for COPD Anxiety
Did the trial show that a smartphone app treats anxiety disorder?
No. It showed lower HADS-anxiety scores after a 12-week COPD rehabilitation program. HADS-anxiety is a symptom scale, not a stand-alone anxiety-disorder diagnosis.
Was walking to rhythm enough?
No clear signal. Rhythm-guided walking alone did not significantly beat usual care, while the combined walking-plus-singing program did.
Who should read this result cautiously?
Patients with severe COPD, low digital access, unstable disease, major psychiatric comorbidity, or poor ability to exercise at home were not fully answered by this small 12-week trial.
References
- Shi M, et al. Smartphone App-Based Music-Facilitated Pulmonary Rehabilitation Program Integrating Rhythm-Guided Walking and Singing for Patients With Chronic Obstructive Pulmonary Disease: Multicenter Randomized Controlled Trial. Journal of Medical Internet Research. 2026. https://doi.org/10.2196/81707
- Spruit MA, et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. American Journal of Respiratory and Critical Care Medicine. 2013. doi:10.1164/rccm.201309-1634st
- Adeloye D, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. EClinicalMedicine. 2022. doi:10.1016/s2213-2600(21)00511-7
- Lewis A, et al. Singing for Lung Health: a systematic review of the literature and consensus statement. BMC Pulmonary Medicine. 2016. doi:10.1038/npjpcrm.2016.80