A 2026 open-label feasibility trial involving 5 Parkinson’s disease patients found that app-randomized levodopa timing was associated with a mean 4.4-point improvement on the Unified Parkinson’s Disease Rating Scale, but the signal missed conventional statistical significance at p = 0.063.1 The narrow conclusion is feasibility: this was a dosing experiment that justified a blinded controlled trial, not proof that artificial intelligence has learned how to optimize Parkinson’s medication.
Research Highlights
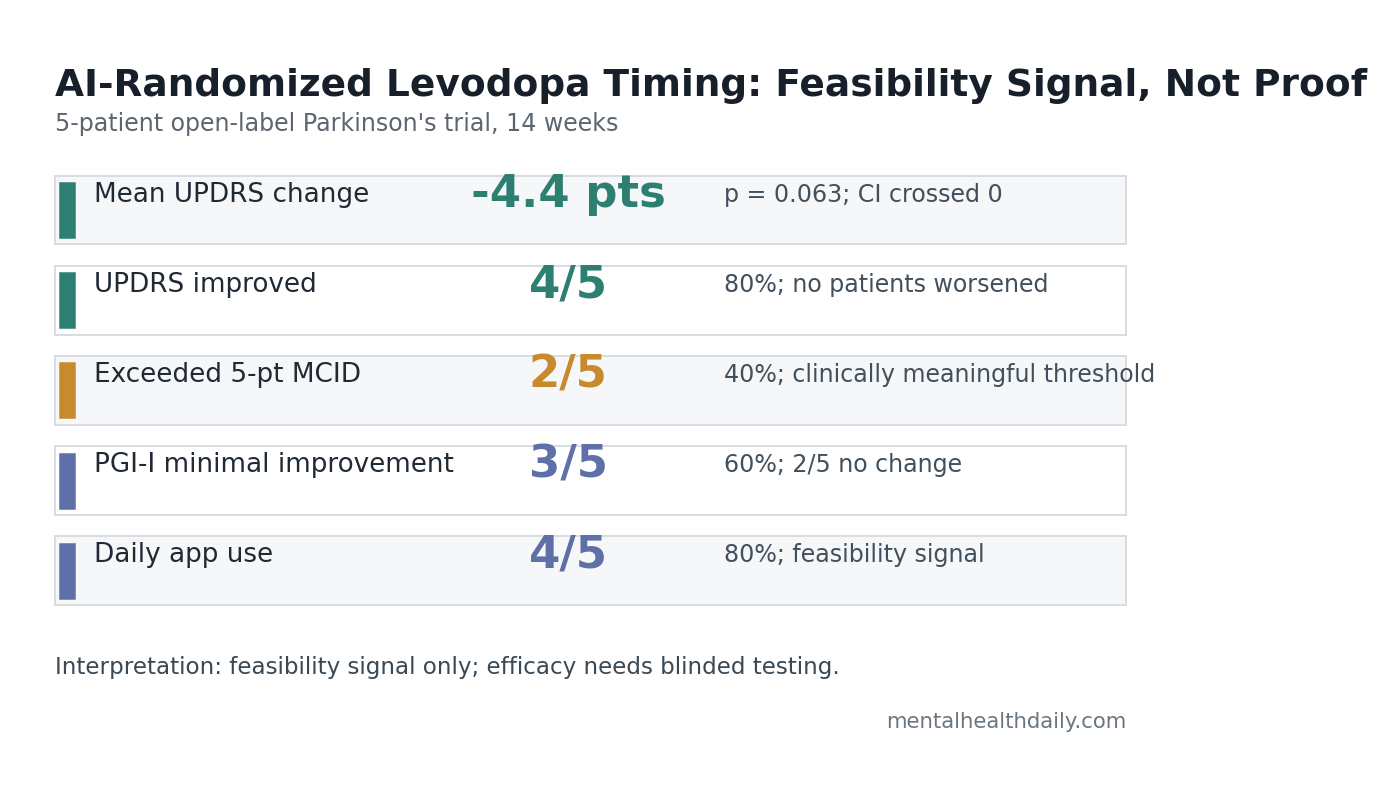
- UPDRS moved in the right direction: mean total score improved 4.4 points over 14 weeks, from 42.6 to 38.2, with p = 0.063 and Cohen’s d = 0.82.1
- Most patients improved, but few cleared the threshold: 4 of 5 patients improved on UPDRS, while 2 of 5 exceeded the 5-point minimal clinically important difference.
- Patient-rated benefit was modest: 3 of 5 patients reported minimal improvement on the Patient Global Impression of Improvement scale, and 2 of 5 reported no change.
- Feasibility looked stronger than efficacy: 4 of 5 patients used the app daily, 5 of 5 completed the 14-week follow-up, and no significant adverse events were recorded.
- Blinded testing is the real gate: the trial had 5 patients, no control group, no blinding, and a confidence interval that crossed zero.
Levodopa is the main dopamine-replacement drug for Parkinson’s disease, and it remains one of the strongest symptomatic treatments in neurology. Long-term dosing is difficult because benefit can wear off before the next dose, sudden OFF periods can appear, and dyskinesias can emerge after years of treatment.2
The Lehmann et al. trial tested a specific idea: instead of asking patients to take levodopa at fixed times, a phone app randomized dose timing inside clinician-approved windows. Daily dose did not exceed the prior prescribed amount, and patients did not take levodopa more frequently than before enrollment.
4.4 UPDRS Points Is a Signal, Not Proof of Efficacy
UPDRS means Unified Parkinson’s Disease Rating Scale, a clinician-rated scale that captures motor and non-motor Parkinson’s burden. In this study, baseline total UPDRS averaged 42.6. After the app-guided intervention, the mean score was 38.2, a 4.4-point improvement.1
That direction is encouraging, but the statistics are not definitive. The 95% confidence interval ran from −0.3 to 9.1 points, and p = 0.063. In practical terms, the data leaned toward benefit but were too small and uncertain to rule in a reliable treatment effect.
Minimal clinically important difference (MCID) is the approximate amount of change likely to feel meaningful to patients or clinicians. Lehmann et al. used a 5-point UPDRS total-score threshold. Only 2 of 5 patients crossed it, even though 4 of 5 moved in the favorable direction.
This distinction keeps the result calibrated. A 4.4-point mean change is not nothing. It is also not a confirmed treatment effect. In an uncontrolled Parkinson’s trial, improvement can come from expectancy, extra monitoring, regression to the mean, natural symptom fluctuation, measurement timing, or a true pharmacologic advantage.
The App Randomized Timing Inside Physician-Set Boundaries
Constrained Disorder Principle (CDP) is the study team’s term for controlled variability inside biological or treatment boundaries. Here, the app did not discover a new dose with deep learning. It used an algorithmic randomization engine to vary levodopa timing within pre-approved windows.
Open-loop algorithm means the system generated schedules without adapting in real time to symptom feedback or biomarkers. The researchers described later levels that might incorporate patient-reported outcomes or biological signatures, but this Parkinson’s study tested the first level: randomized timing, reminders, and adherence monitoring.
The protocol had 2 phases:
- 4-week run-in: patients used the app without changing levodopa dose or administration time.
- 10-week intervention: the app randomized timing inside individualized windows while keeping dose limits under clinician control.
All UPDRS assessments were conducted during ON states, within 1–2 hours of levodopa administration. That reduces timing noise during scoring, but it also means the trial did not directly prove reduced daily OFF time, fewer dyskinesias, or better motor fluctuation control across the full day.
Adherence Was Stronger Than Efficacy Evidence
The feasibility findings were more straightforward than the clinical findings. All 5 patients completed the 14-week follow-up, 4 of 5 used the app daily, and all 5 were reported as adherent by weekly coordinator phone questionnaires.1
Why adherence matters here: Parkinson’s medication timing is behaviorally demanding. Wearing-off management often requires precise timing, multiple daily doses, meal coordination, and rapid recognition of emerging OFF periods.2 A medication app that patients ignore cannot test the biological dosing idea behind it.
Straka et al. reviewed adherence to Parkinson’s pharmacotherapy and found enough practical complexity to make dose-taking behavior part of the clinical problem, not an administrative footnote.4 In that context, 80% daily app use in a 5-person pilot is useful feasibility evidence, even though it says little about efficacy.
No significant adverse events were recorded. That is reassuring but thin. A 5-patient, 14-week trial cannot exclude uncommon harms, worsening dyskinesia in vulnerable subgroups, medication errors, or long-term problems created by variable timing.
Levodopa Response Variability Is a Real Parkinson’s Problem
Variable response to levodopa is not an invented problem. Pitz et al. reviewed pathologically confirmed Parkinson’s disease cases and found that levodopa responsiveness varies across patients, even when the diagnosis is secure.3 That variability gives a biologically plausible reason to test individualized timing systems.
Wearing-off means Parkinson’s symptoms return before the next levodopa dose is due. Pahwa and Lyons described it as a common long-term management problem, with identification and dose adjustment often needed before patients recognize the pattern clearly.2
Lehmann et al. sit at the intersection of those 2 issues: levodopa response varies, and timing matters. The open question is whether bounded randomization is better than careful clinician-guided dose scheduling, extended-release formulations, add-on drugs, or patient education.
Standard clinical optimization can produce larger UPDRS changes than this pilot reported. Lehmann et al. noted that typical levodopa optimization or adjustment strategies can improve UPDRS by 5–10 points, while medication switches or additions may yield 8–15 points. Their 4.4-point signal is therefore supplementary at best unless controlled trials show a clearer advantage.
Earlier CDP Work Does Not Prove Parkinson’s Benefit
Lehmann et al. cited earlier constrained-disorder-principle work in chronic diseases, including an open-label feasibility trial in heart-failure patients with diuretic resistance.5 Those studies support the broader platform idea that variable regimens can be implemented in real patients.
They do not prove Parkinson’s efficacy. Heart failure diuretic response, chronic pain dosing, antimicrobial resistance, and levodopa motor response are different clinical systems. Shared software philosophy is weaker evidence than a blinded Parkinson’s comparator arm.
Evidence-strength note: this Parkinson’s study can support 3 claims: the app could be used by a small group, no obvious safety signal appeared over 14 weeks, and the clinical signal was large enough to justify a better trial. It cannot support claims that AI-guided levodopa timing works, prevents dyskinesia, reduces OFF time, or outperforms standard movement-disorder care.
Practical gate: the next study has to show an advantage over reminders, clinician-guided timing, and ordinary pre-post improvement.
It also needs dose-safety tracking because variable timing could shift nausea, sleepiness, hallucinations, or dyskinesia risk in larger samples.
A Better Trial Would Need a Sham-App Control
The next useful test needs more than a larger open-label sample. The design needs to separate the algorithm from extra monitoring, reminders, expectation, and clinician attention.
A stronger Parkinson’s trial would include:
- Randomization: variable app-guided timing vs. standard timing or sham-app notifications.
- Blinded scoring: independent UPDRS raters who do not know allocation.
- Motor-fluctuation endpoints: daily OFF time, dyskinesia time, rescue-dose use, falls, and patient diaries.
- Longer follow-up: at least 6–12 months to test durability and safety.
- Comparator clarity: whether the app beats ordinary dose optimization, reminders alone, or clinician-guided adjustment.
The current data make that trial reasonable. They do not make the answer obvious. If the future controlled trial shows a similar 4–5 point UPDRS advantage over a credible control arm, the idea becomes clinically interesting. If the advantage disappears under blinding, the pilot will have been a useful false start.
Questions About AI Levodopa Dosing
Did artificial intelligence optimize each Parkinson’s patient’s dose?
No. The study used algorithmic randomization within physician-defined timing and dose boundaries. It did not use adaptive machine learning to discover each patient’s best regimen from real-time outcomes.
Was the 4.4-point UPDRS improvement clinically meaningful?
It was close to the 5-point threshold the researchers used, and 2 of 5 patients exceeded that threshold. The mean result was still statistically uncertain, with p = 0.063 and a confidence interval crossing zero.
Should Parkinson’s patients change levodopa timing based on this study?
No. Levodopa timing changes should be handled with a clinician, especially in patients with dyskinesia, hallucinations, orthostatic hypotension, sleepiness, or complex wearing-off patterns. This trial supports further testing, not self-experimentation.
What result would make this approach more convincing?
A blinded randomized trial would need to show better UPDRS, OFF-time, dyskinesia, or quality-of-life outcomes than reminders or standard dose optimization alone. App use by itself is not enough.
References
- Lehmann H, et al. A feasibility open-label clinical trial utilizing second-generation artificial intelligence based on the constrained-disorder principle in patients with Parkinson’s disease. IBRO Neuroscience Reports. 2026. doi:10.1016/j.ibneur.2026.02.019
- Pahwa R, Lyons KE. Levodopa-related wearing-off in Parkinson’s disease: identification and management. Current Medical Research and Opinion. 2009. doi:10.1185/03007990902779319
- Pitz V, et al. The levodopa response varies in pathologically confirmed Parkinson’s disease: a systematic review. Movement Disorders Clinical Practice. 2020. doi:10.1002/mdc3.12940
- Straka I, et al. Clinical aspects of adherence to pharmacotherapy in Parkinson disease: a PRISMA-compliant systematic review. Medicine. 2018. doi:10.1097/md.0000000000010962
- Gelman R, et al. A second-generation artificial intelligence-based therapeutic regimen improves diuretic resistance in heart failure: results of a feasibility open-labeled clinical trial. Biomedicine & Pharmacotherapy. 2023. doi:10.1016/j.biopha.2023.114334