A 2026 systematic review argues that catatonia should be read as a limbic-cortical circuit syndrome, with motor shutdown tied to brain systems for threat, salience, motivation, and emotional regulation.
Research Highlights
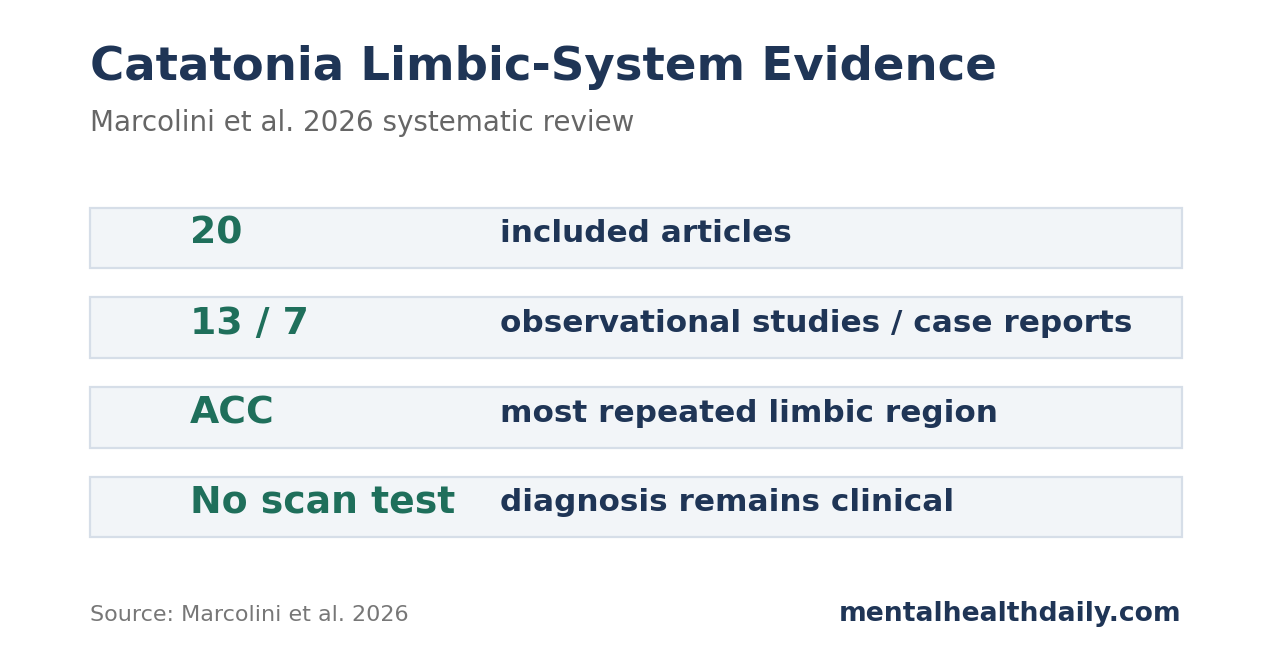
- 20 studies met criteria: the 2026 review screened 1,792 records, assessed 54 full texts, and included 20 articles: 13 observational studies and 7 case reports.1
- Anterior cingulate findings were most recurrent: included studies reported 4 kinds of signal involving the ACC: altered regional blood flow, abnormal gyrification, gray matter reduction, and a deep-brain-stimulation case involving cingulate targeting.
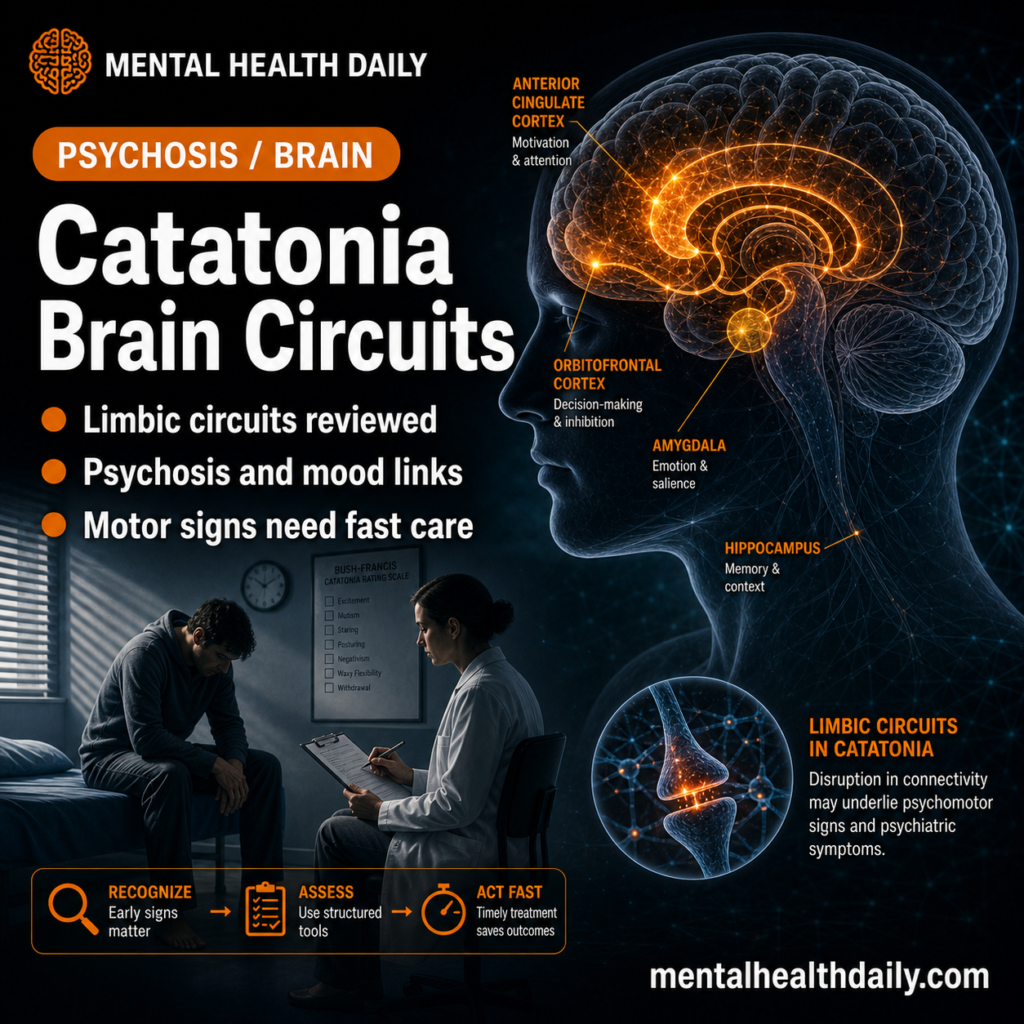
- Catatonia looks circuit-level: limbic findings across 6 regions — amygdala, hippocampus, cingulate cortex, insula, orbitofrontal cortex, and hypothalamus — point toward altered emotion-motor coupling rather than a single lesion.
- Clinical diagnosis still comes first: bedside recognition of at least 3 catatonic signs remains the treatment gateway, especially when patients present with immobility, mutism, posturing, abnormal repetition, or unexplained agitation.
- Evidence strength is preliminary: the 20-study base included small samples, cross-sectional designs, case reports, variable catatonia scales, and mixed diagnoses, preventing firm region-by-symptom mapping.
Catatonia is a neuropsychiatric syndrome in which movement, speech, behavior, and affect can become profoundly dysregulated. It can appear across several settings:
- schizophrenia and other psychotic disorders
- mood disorders
- autism and neurodevelopmental conditions
- medical or neurological illness
- infection, inflammation, or metabolic disturbance
- medication exposure or withdrawal
- malignant catatonia with autonomic instability
Catatonia has multiple causes. Different psychiatric, neurological, medical, metabolic, infectious, inflammatory, and medication-related problems can converge on the same shutdown-like clinical syndrome. The limbic-system argument is that these different routes may disturb shared circuits for threat response, motivation, body state, and motor control.
The standard clinical presentation is motor-heavy, with prominent movement, speech, and behavioral signs:
- stupor or immobility
- mutism
- posturing, rigidity, catalepsy, or waxy flexibility
- negativism
- stereotypy, mannerisms, or grimacing
- echolalia or echopraxia
- agitation that is not driven by obvious external stimuli
The newer limbic-system review adds a mechanistic layer: catatonia may reflect a failure of brain networks that connect emotional threat and bodily salience to motor control.
Catatonia Requires Fast Recognition and Treatment
Catatonia was historically tied to schizophrenia, but current diagnostic systems treat it as a specifier that can occur across psychiatric and medical conditions. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition requires at least 3 catatonic signs from the clinical pattern above.
How often catatonia is found depends on where researchers look and how carefully they screen for it. A meta-analysis by Solmi et al. found catatonia across clinical samples rather than only in schizophrenia; rates varied by diagnosis and by whether studies used structured assessments, chart review, diagnostic labels, or symptom clusters.3
The Bush-Francis Catatonia Rating Scale is widely used, but older and newer studies have not measured catatonia the same way.
Clinically, fast recognition matters more than waiting for a brain-based explanation. Consensus guidance from the British Association for Psychopharmacology emphasizes a practical sequence:2
- Recognize catatonic signs promptly: stupor, mutism, posturing, negativism, abnormal repetition, unexplained agitation, or related symptoms should trigger a structured exam.
- Look for underlying causes: evaluation should include psychiatric, neurological, medical, medication-related, metabolic, infectious, and inflammatory contributors when clinically relevant.
- Use benzodiazepines when appropriate: lorazepam is commonly used as first-line treatment.
- Escalate to ECT when needed: electroconvulsive therapy (ECT; electrically induced therapeutic seizures under anesthesia) is used for severe, malignant, or benzodiazepine-resistant catatonia.
- Prevent complications: untreated malignant catatonia can involve fever, autonomic instability, dehydration, immobility complications, and death.
20 Included Studies Pointed Beyond Motor Cortex
Marcolini et al. searched MEDLINE, Web of Science, PsycINFO, and Scopus without date restrictions for studies linking catatonia to limbic-system structures.1 The review identified 1,792 database records, removed 779 duplicates, screened 1,013 titles and abstracts, assessed 54 full texts, excluded 40, and added 6 studies from reference screening. The final evidence base included 20 articles published from 1986 to 2024.
The included evidence was diverse but thin:
- Study designs: 12 cross-sectional studies, 1 retrospective study, and 7 case reports.
- Sample sizes: enrolled patient counts ranged from 1 to 172.
- Age span: participants ranged from 18 to 65 years.
- Methods: structural magnetic resonance imaging (MRI), functional MRI, perfusion imaging, histology, genetic findings, neuropathology, and psychometric testing.
- Diagnoses: many samples focused on schizophrenia spectrum disorder with catatonia, while some case reports involved neurological or acquired causes.
The review's main contribution is organization. Previous summaries emphasized cortical, basal-ganglia, cerebellar, or broad imaging findings.5 Haroche et al.'s imaging review also showed how scattered the catatonia neuroimaging literature remained.6 Marcolini et al. narrowed the lens to limbic structures: hippocampus, amygdala, anterior and posterior cingulate cortex, insula, orbitofrontal cortex, hypothalamus, and related circuitry.
Anterior Cingulate Cortex Had the Most Repeated Signal
The anterior cingulate cortex (ACC) sits at the junction of affect, motivation, conflict monitoring, autonomic regulation, and action selection. It is anatomically positioned to connect emotional salience with whether the body initiates, withholds, or shifts behavior.
Repeated ACC findings: In the 2026 review, ACC findings appeared across several methods. Walther et al. reported regional cerebral blood-flow differences involving the ACC in catatonic patients compared with non-catatonic patients.1 Hirjak et al. reported increased local gyrification index in the rostral ACC in schizophrenia spectrum disorder with catatonia compared with schizophrenia spectrum disorder without catatonia.
Other studies found reduced ACC gray matter volume compared with healthy controls, and 1 case report described resolution of catatonic motor symptoms after deep brain stimulation targeting the subgenual cingulate region.
How to read the signal: Local gyrification index means the degree of cortical folding in a region. It is often interpreted as a neurodevelopmental or structural marker rather than a moment-to-moment activity measure. Gray matter reduction is also not a clean activity readout; a smaller region can reflect different mixtures of neuron, glial, synaptic, vascular, illness, medication, developmental, or measurement effects.
The ACC pattern is still notable because it fits catatonia's clinical mixture. A syndrome that combines immobility, mutism, withdrawal, fear-like shutdown, conflict, and motivational collapse should involve more than primary motor cortex. The ACC is one plausible bridge between affective load and motor output.
Amygdala, Hippocampus, and Hypothalamus Link Threat, Memory, and Autonomic State
The amygdala is involved in salience detection and threat learning. The hippocampus supports memory, context, and spatial mapping. The hypothalamus helps coordinate autonomic and endocrine body-state responses. Together, these structures make catatonia easier to understand as a whole-body state rather than as an isolated movement disorder.
The review summarized several limbic findings:
- Amygdala: Fritze et al. reported reduced amygdala volume in schizophrenia spectrum disorder with catatonia compared with schizophrenia spectrum disorder without catatonia and healthy controls; Walther et al. later reported decreased right amygdala gray matter volume in catatonia relative to healthy controls.7
- Hippocampus: early postmortem studies reported neuronal loss or disorganization in hippocampal subregions in schizophrenia with catatonic features, while newer imaging work reported reduced hippocampal volume in schizophrenia spectrum disorder with catatonia.
- Hypothalamus: Fritze et al. reported lower anterior-inferior hypothalamus volume in schizophrenia spectrum disorder with catatonia than in non-catatonic schizophrenia spectrum disorder and healthy controls.
- Neuropathology and genetics: case reports and genetic studies included TDP-43 accumulation in limbic regions and WKL1 haploinsufficiency in a pedigree with catatonic schizophrenia, but these findings remain hypothesis-generating.
These findings sit well beside the fear-response model of catatonia. Moskowitz proposed catatonia as an evolutionarily shaped defensive response, sometimes described as a freeze-like state under extreme threat.8 The limbic review does not prove that model, but it gives the model more anatomical plausibility.
Orbitofrontal and Insula Findings Fit Emotion-Motor Uncoupling
The orbitofrontal cortex (OFC) helps evaluate reward, punishment, emotional meaning, and decision value. It is not always listed as classic limbic system anatomy, but it is heavily connected with limbic regions and appears repeatedly in catatonia studies.
Northoff et al. reported orbitofrontal dysfunction during emotional stimulation in akinetic catatonia.9 More recent work found orbitofrontal sulcal-pattern differences and gray matter reductions in catatonia samples. The review interpreted OFC findings as relevant to top-down control: when prefrontal regulation of emotion and action breaks down, basal-ganglia and cingulate systems may shift toward motor inhibition, mutism, or withdrawal.
The insula and posterior cingulate cortex (PCC) had more limited but relevant evidence. The insula integrates interoception, meaning the brain's mapping of internal body states such as pain, nausea, breath, tension, and autonomic arousal.
Parekh et al. reported resting-state functional connectivity and structural abnormalities in acute retarded catatonia, including altered coupling of salience and motor networks.10 In plain terms, circuits that should help identify internal urgency and coordinate action may become poorly synchronized with the systems that initiate movement.
Evidence Is Too Thin for Region-by-Symptom Mapping
The review is strongest as a synthesis and weakest as a causal map. Most included studies were small, cross-sectional, single-center, or case-based. Cross-sectional means the researchers observed people at one point in time; it cannot show whether a brain difference caused catatonia, resulted from catatonia, reflected chronic illness, tracked medication exposure, or represented a stable vulnerability.
The studies also varied in catatonia definitions, scales, diagnoses, imaging protocols, and control groups. Few studies separated acute, chronic, malignant, stuporous, excited, affective-predominant, or motor-predominant catatonia. That makes a precise claim impossible: the literature cannot yet say that amygdala volume predicts fear-loaded catatonia, that ACC gray matter predicts mutism, or that hypothalamic volume identifies malignant autonomic risk.
An evidence-strength note is essential: this systematic review supports a plausible circuit model, not a clinical biomarker. It can justify better mechanistic studies. It cannot diagnose catatonia from a scan, choose benzodiazepine vs. ECT from a limbic finding, or replace urgent bedside treatment.
Practical Implications: Treat the Syndrome, Study the Circuit
The clinical workflow stays grounded in recognition and treatment. Catatonia can be missed when clinicians treat mutism, withdrawal, agitation, or refusal to eat as purely oppositional, psychotic, depressive, autistic, delirious, or behavioral. Structured examination for catatonic signs remains the front door.
The circuit model can improve interpretation after recognition. Limbic-system involvement explains why catatonia can feel emotionally loaded even when a patient is silent, immobile, or externally unresponsive. It also explains why catatonia cuts across diagnoses: different disorders can converge on the same emotion-motor control networks.
For research, the next step is clear enough: large multimodal studies that combine standardized catatonia scales, symptom subtyping, medication and illness-stage data, structural MRI, functional MRI, perfusion imaging, and longitudinal follow-up before and after benzodiazepines or ECT.
Key research question: whether limbic findings normalize with treatment, predict relapse, or separate catatonia subtypes.
Questions About Catatonia Brain Circuits
Is catatonia only a motor disorder?
No. Motor signs define the bedside syndrome, but the 2026 review supports involvement of limbic-cortical circuits that regulate emotion, salience, motivation, body state, and action.
What causes catatonia?
Catatonia can be caused by several routes, including psychotic disorders, mood disorders, autism and neurodevelopmental conditions, neurological disease, medical illness, infection, inflammation, metabolic disturbance, medication exposure, or withdrawal. The practical move is to treat the catatonic state while also looking for the underlying cause.
Can a brain scan diagnose catatonia?
No. Current imaging findings are research signals. Catatonia is still diagnosed clinically through signs such as stupor, mutism, posturing, negativism, waxy flexibility, echolalia, echopraxia, and abnormal agitation.
Which brain region had the strongest evidence?
The anterior cingulate cortex had the most repeated pattern across methods, including blood-flow, gyrification, gray matter, and stimulation-related findings. Orbitofrontal and amygdala findings were also recurrent.
Does limbic involvement change treatment?
Not yet. The practical treatment sequence remains rapid assessment, medical workup, benzodiazepines when appropriate, supportive prevention of immobility complications, and ECT for severe or refractory cases.
References
- Frozen emotions, frozen bodies: a systematic review of limbic system alterations in catatonia. Marcolini F et al. European Archives of Psychiatry and Clinical Neuroscience. 2026. doi:10.1007/s00406-026-02244-8
- Evidence-based consensus guidelines for the management of catatonia: recommendations from the British Association for Psychopharmacology. Rogers JP et al. Journal of Psychopharmacology. 2023;37(4):327-369. doi:10.1177/02698811231158232
- Prevalence of catatonia and its moderators in clinical samples: results from a meta-analysis and meta-regression analysis. Solmi M et al. Schizophrenia Bulletin. 2018;44(5):1133-1150. doi:10.1093/schbul/sbx157
- Structure and neural mechanisms of catatonia. Walther S et al. Lancet Psychiatry. 2019;6(7):610-619. doi:10.1016/s2215-0366(18)30474-7
- Brain mechanisms underlying catatonia: a systematic review. Cattarinussi G et al. Schizophrenia Research. 2024;263:194-207. doi:10.1016/j.schres.2022.11.002
- Brain imaging in catatonia: systematic review and directions for future research. Haroche A et al. Psychological Medicine. 2020;50(10):1585-1597. doi:10.1017/s0033291720001853
- Structural alterations of amygdala and hypothalamus contribute to catatonia. Fritze S et al. Schizophrenia Research. 2024;263:122-130. doi:10.1016/j.schres.2022.05.003
- “Scared stiff”: catatonia as an evolutionary-based fear response. Moskowitz AK. Psychological Review. 2004;111(4):984-1002. doi:10.1037/0033-295x.111.4.984
- Orbitofrontal cortical dysfunction in akinetic catatonia: a functional magnetic resonance imaging study during negative emotional stimulation. Northoff G et al. Schizophrenia Bulletin. 2004;30(2):405-427. doi:10.1093/oxfordjournals.schbul.a007088
- Resting state functional connectivity and structural abnormalities of the brain in acute retarded catatonia: an exploratory MRI study. Parekh P et al. European Archives of Psychiatry and Clinical Neuroscience. 2022;272(6):1045-1059. doi:10.1007/s00406-021-01345-w