A 2026 randomized youth trial found that integrated exposure-based treatment reduced posttraumatic stress disorder symptoms more than supportive counseling, while substance-use changes were smaller and showed no clear treatment-specific advantage.
Research Highlights
- COPE-A reduced PTSD more: youth receiving Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure – Adolescent version had a 17.00-point greater reduction in PTSD-RI total score than supportive counseling from session 1 to session 11.1
- The main separation appeared later: the largest treatment difference occurred from sessions 5 to 11, the phase that included prolonged exposure, with COPE-A producing a 12.95-point larger PTSD-RI reduction than supportive counseling.
- Substance-use change lacked a group advantage: COPE-A showed within-group frequency reduction, but COPE-A and supportive counseling did not differ significantly for substance-use frequency (p = 0.376) or quantity (p = 0.582).
- PTSD change and substance-use change were not tightly linked: early PTSD improvement failed to predict later substance-use frequency reduction (r = −0.12), and early frequency change failed to predict later PTSD improvement (r = 0.03).
- Evidence strength is useful but underpowered: this was a secondary analysis of 49 treated participants, so the PTSD result is more persuasive than the temporal-sequencing correlations.
Posttraumatic stress disorder (PTSD; persistent trauma-related symptoms such as intrusions, avoidance, negative mood, and hyperarousal) and substance use disorder (SUD; harmful or compulsive use of alcohol or other drugs) often reinforce each other. A common theory is self-medication: trauma symptoms increase distress, and substances are used to blunt that distress, at least in the short term.2
Dobson et al. analyzed youth aged 13 to 25 from a randomized controlled trial comparing COPE-A, an integrated exposure-based therapy, with Person-Centered Therapy (PCT; supportive counseling focused on empathy, reflection, and client-led discussion).1 The analysis asked how PTSD and substance-use symptoms changed during treatment and whether improvement in one domain tended to precede improvement in the other.
COPE-A Produced Larger PTSD-RI Reductions by Session 11
The analysis included 49 participants who attended at least 1 session, drawn from 55 randomized youth. Mean age was 19.5 years, with a range of 13 to 25.
Most participants had severe and complex presentations: 87.8% met full-threshold Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition PTSD criteria, the average Clinician-Administered PTSD Scale for Children and Adolescents for DSM-5 score was 35.9, and participants reported a median of 6 traumatic events.
Substance use was also broad rather than single-drug. Cannabis was the most common primary drug of choice at baseline, reported by 51.0%, followed closely by alcohol at 49.0%. Participants reported a median of 4 drugs used in the past month.
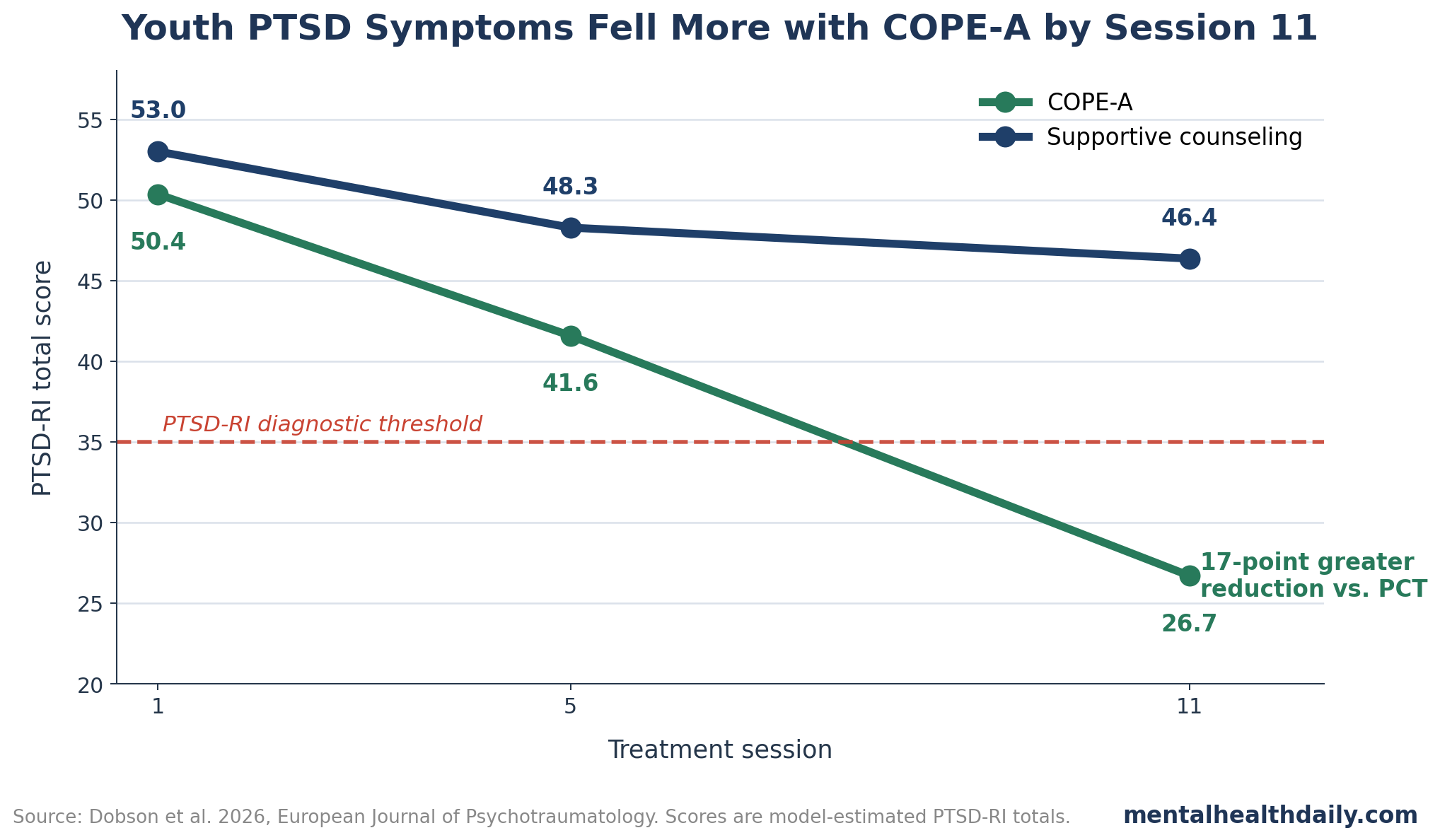
PTSD symptoms were measured with the UCLA PTSD Reaction Index (PTSD-RI; a youth PTSD symptom scale with a total score up to 84). The researchers modeled scores at session 1, session 5, and session 11. COPE-A separated clearly from supportive counseling by session 11:
- COPE-A total PTSD-RI: 50.35 at session 1, 41.58 at session 5, and 26.70 at session 11.
- PCT total PTSD-RI: 53.00 at session 1, 48.28 at session 5, and 46.36 at session 11.
- Overall between-group change: COPE-A had a 17.00-point greater PTSD-RI reduction from session 1 to session 11, 95% confidence interval (CI) −29.50 to −4.46, p < 0.005.
- Later-phase separation: COPE-A had a 12.95-point greater reduction than PCT from session 5 to session 11, 95% CI −24.32 to −1.59, p < 0.05.
The session-11 result also crossed a clinically meaningful threshold. The researchers noted that mean PTSD-RI scores in the COPE-A group fell below the diagnostic threshold of 35 by session 11, while the supportive-counseling group remained above it.
Intrusions, Avoidance, and Negative Mood Changed More Than Arousal
COPE-A stands for Concurrent Treatment of PTSD and SUD Using Prolonged Exposure – Adolescent version. Prolonged exposure is a trauma-focused therapy method that helps patients gradually approach trauma memories and avoided situations in a structured way. In COPE-A, exposure work is combined with cognitive behavioral therapy skills for substance use, motivational enhancement, and relapse-prevention material.
The PTSD cluster results were clinically useful because they showed which symptom domains separated most strongly:
- Intrusions: COPE-A produced a 4.29-point greater reduction than PCT from session 1 to session 11, p < 0.05.
- Avoidance: COPE-A produced a 2.81-point greater reduction than PCT, p ≤ 0.001.
- Negative cognition and mood: COPE-A produced a 7.52-point greater reduction than PCT, p < 0.005.
- Arousal and reactivity: COPE-A improved within group, but the between-group interaction was not significant, p = 0.452.
The later treatment phase carried much of the signal. Intrusion and avoidance scores did not significantly change from session 1 to session 5 in either group, then improved in COPE-A from session 5 to session 11. Negative cognition and mood improved in both COPE-A treatment phases, with a larger later-phase reduction.
This pattern fits adult COPE work and broader evidence on integrated trauma-focused therapy. Mills et al. found that integrated exposure-based therapy reduced PTSD symptoms in adults with PTSD and substance dependence in a randomized JAMA trial.3
Ruglass et al. also found support for concurrent prolonged exposure in full or subthreshold PTSD with substance-use disorders.4 Hien et al. later synthesized psychotherapy and pharmacologic trials for comorbid PTSD, alcohol, and other drug use disorders, finding that trauma-focused approaches were important for PTSD reduction.5
Substance-Use Frequency Improved Modestly Without a Group Advantage
Substance-use outcomes were measured with Timeline Followback (TLFB; a calendar-based interview method for estimating substance use over recent days). The researchers separated frequency from quantity. Frequency captured how often participants used their main substance of concern, while quantity captured the amount used, standardized across substances.
The frequency result had 2 layers. COPE-A showed within-group reductions, but COPE-A and supportive counseling did not significantly differ from each other:
- COPE-A frequency: mean frequency fell from 1.45 at session 1 to 1.20 at session 5 and 1.00 at session 11.
- PCT frequency: mean frequency moved from 1.31 at session 1 to 1.13 at session 5 and 1.21 at session 11.
- COPE-A within-group change: session 1 to session 5 mean difference −0.25, p < 0.05; session 1 to session 11 mean difference −0.45, p < 0.05.
- Between-group frequency comparison: no significant group x time interaction, p = 0.376.
Quantity changed even less. COPE-A quantity moved from 0.81 at session 1 to 0.75 at sessions 5 and 11. PCT quantity moved from 0.81 to 0.74 and 0.73. The group x time interaction for quantity was non-significant, p = 0.582, and models without the interaction found no significant group or time effect.
That distinction between frequency and quantity is important in youth samples with mixed cannabis, alcohol, and other substance profiles. Quantity standardization across substances is mathematically awkward. A smaller number of heavy alcohol episodes, a reduced number of cannabis-use days, and changes in polysubstance combinations can all move risk differently while looking compressed in a single transformed quantity score.
PTSD and Substance-Use Changes Were Weakly Coupled
The analysis also examined temporal sequencing, meaning whether earlier change in one symptom domain predicted later change in another. Because the sample was small and attrition increased over sessions, the researchers used aggregated phase-change scores instead of more complex session-level lagged models.
Within PTSD, symptom clusters tended to improve together during the same phase. Concurrent cluster-change correlations were strong, ranging from r = 0.54 to r = 0.78. Correlation r is a measure of association from −1 to +1; values above 0.5 are usually moderate to strong.
Early-to-later temporal links were much weaker. The only significant negative temporal associations were early-to-later intrusion change, r = −0.43, p = 0.049, and early avoidance change with later negative mood/cognition change, r = −0.47, p = 0.030.
Substance-use frequency and quantity also moved together within the same phase. Quantity and frequency change correlated r = 0.45 from sessions 1 to 5 and r = 0.62 from sessions 5 to 11. Across phases, the only significant temporal substance-use association was a negative association between early quantity change and later quantity change, r = −0.52, p = 0.018.
The PTSD-to-substance-use links were the most clinically relevant part. They were mostly absent:
- Concurrent early phase: PTSD total change was not significantly associated with frequency change, r = −0.04, p = 0.802, or quantity change, r = −0.10, p = 0.586.
- Concurrent later phase: PTSD total change was not significantly associated with frequency change, r = 0.28, p = 0.220, or quantity change, r = 0.07, p = 0.766.
- Early PTSD to later substance use: PTSD change from sessions 1 to 5 was not significantly associated with later quantity change, r = −0.06, p = 0.784, or later frequency change, r = −0.12, p = 0.616.
- Early substance use to later PTSD: quantity change predicted later PTSD change at r = 0.01, p = 0.980; frequency change predicted later PTSD change at r = 0.03, p = 0.913.
Adult data have been mixed on this point. Back et al. reported symptom improvement patterns in PTSD with alcohol dependence, and Hien et al. found in a NIDA trial that PTSD improvement could affect substance-use outcomes.26
Other work, including Badour et al. in veterans and Peirce et al. in PTSD with substance-use disorders, found weaker temporal coupling.78 The youth trial adds an important data point: PTSD can improve meaningfully during integrated exposure therapy while substance-use improvement remains smaller and less clearly synchronized.
Evidence Strength and Treatment Implications
Evidence strength: moderate for COPE-A reducing youth PTSD symptoms compared with supportive counseling, low-to-moderate for claims about symptom sequencing. The PTSD result came from a randomized treatment comparison and showed a large between-group separation by session 11. The sequencing analysis was secondary, exploratory, and based on 49 treated participants rather than the full randomized sample.
The limitations are practical rather than cosmetic. The study could not use all 16 sessions for sequencing because attrition reduced sample size at later timepoints. Phase-aggregated change scores are less precise than session-by-session cross-lagged models. Substance use was based on retrospective self-report. The sample combined adolescents and emerging adults, and legal access to alcohol in Australia begins at age 18, which may affect substance-use trajectories independently of therapy.
The treatment implication is direct: clinicians should not assume that PTSD improvement automatically produces large substance-use reduction in youth with comorbid PTSD-SUD. COPE-A looked strong for PTSD symptoms and tolerable in the context of ongoing substance use, but additional substance-focused supports may be needed when frequency, quantity, cravings, polysubstance use, or relapse risk remain active.
Questions About Youth PTSD, Substance Use, and COPE-A
How was COPE-A different from supportive counseling in this trial?
COPE-A is an adolescent-adapted integrated therapy for PTSD and substance-use problems. It combines prolonged exposure for trauma symptoms with cognitive behavioral therapy and relapse-prevention material for substance use.
Did COPE-A reduce PTSD symptoms more than supportive counseling?
Yes. COPE-A produced a 17.00-point greater PTSD-RI reduction than supportive counseling from session 1 to session 11, and the COPE-A mean fell below the diagnostic threshold by session 11.
Did substance use improve at the same level as PTSD?
Substance-use frequency decreased within the COPE-A group, but the trial did not find a significant between-group advantage for substance-use frequency or quantity. PTSD improvement was the clearer treatment signal.
Does this mean exposure therapy is unsafe for youth who use substances?
The trial supports the opposite concern being overstated. In this sample, exposure-based integrated treatment reduced PTSD symptoms in youth with ongoing substance use, without evidence that substance-use outcomes worsened relative to supportive counseling.
References
- Temporal Sequencing of Symptom Change in Youth Receiving Treatment for Posttraumatic Stress Disorder and Substance Use: Secondary Findings from a Randomized Controlled Trial. Dobson O et al. European Journal of Psychotraumatology. 2026;17(1):2630609. doi:10.1080/20008066.2026.2630609
- Symptom Improvement in Co-Occurring PTSD and Alcohol Dependence. Back SE et al. Journal of Nervous and Mental Disease. 2006;194(9):690-696. doi:10.1097/01.nmd.0000235794.12794.8a
- Integrated Exposure-Based Therapy for Co-Occurring Posttraumatic Stress Disorder and Substance Dependence. Mills KL et al. JAMA. 2012;308(7):690-699. doi:10.1001/jama.2012.9071
- Concurrent Treatment with Prolonged Exposure for Co-Occurring Full or Subthreshold Posttraumatic Stress Disorder and Substance Use Disorders: A Randomized Clinical Trial. Ruglass LM et al. Psychotherapy and Psychosomatics. 2017;86(3):150-161. doi:10.1159/000462977
- Project Harmony: A Systematic Review and Network Meta-Analysis of Psychotherapy and Pharmacologic Trials for Comorbid Posttraumatic Stress, Alcohol, and Other Drug Use Disorders. Hien DA et al. Psychological Bulletin. 2024;150(3):319-353. doi:10.1037/bul0000409
- Do Treatment Improvements in PTSD Severity Affect Substance Use Outcomes? A Secondary Analysis from a Randomized Clinical Trial in NIDA’s Clinical Trials Network. Hien DA et al. American Journal of Psychiatry. 2010;167(1):95-101. doi:10.1176/appi.ajp.2009.09091261
- Temporal Dynamics of Symptom Change Among Veterans Receiving an Integrated Treatment for Posttraumatic Stress Disorder and Substance Use Disorders. Badour CL et al. Journal of Traumatic Stress. 2022;35(2):546-558. doi:10.1002/jts.22769
- The Effects of Prolonged Exposure on Substance Use in Patients with Posttraumatic Stress Disorder and Substance Use Disorders. Peirce JM et al. Journal of Traumatic Stress. 2020;33(4):465-476. doi:10.1002/jts.22546
- Safety and Efficacy of Exposure-Based Risk Reduction Through Family Therapy for Co-Occurring Substance Use Problems and Posttraumatic Stress Disorder Symptoms Among Adolescents. Danielson CK et al. JAMA Psychiatry. 2020;77(6):574-586. doi:10.1001/jamapsychiatry.2019.4803
- Psychological Therapies for Post-Traumatic Stress Disorder and Comorbid Substance Use Disorder. Roberts NP et al. Cochrane Database of Systematic Reviews. 2016;(4):CD010204. doi:10.1002/14651858.cd010204.pub2