A 124-person study of euthymic bipolar disorder found that patients with early systematic antidepressant treatment history had higher negative affect, attentional impulsivity, non-planning impulsivity, and total BIS-11A impulsivity scores than matched patients without that history.1 The association is clinically cautionary, but the cross-sectional design cannot separate antidepressant effects from delayed bipolar diagnosis or more severe early depression.
Research Highlights
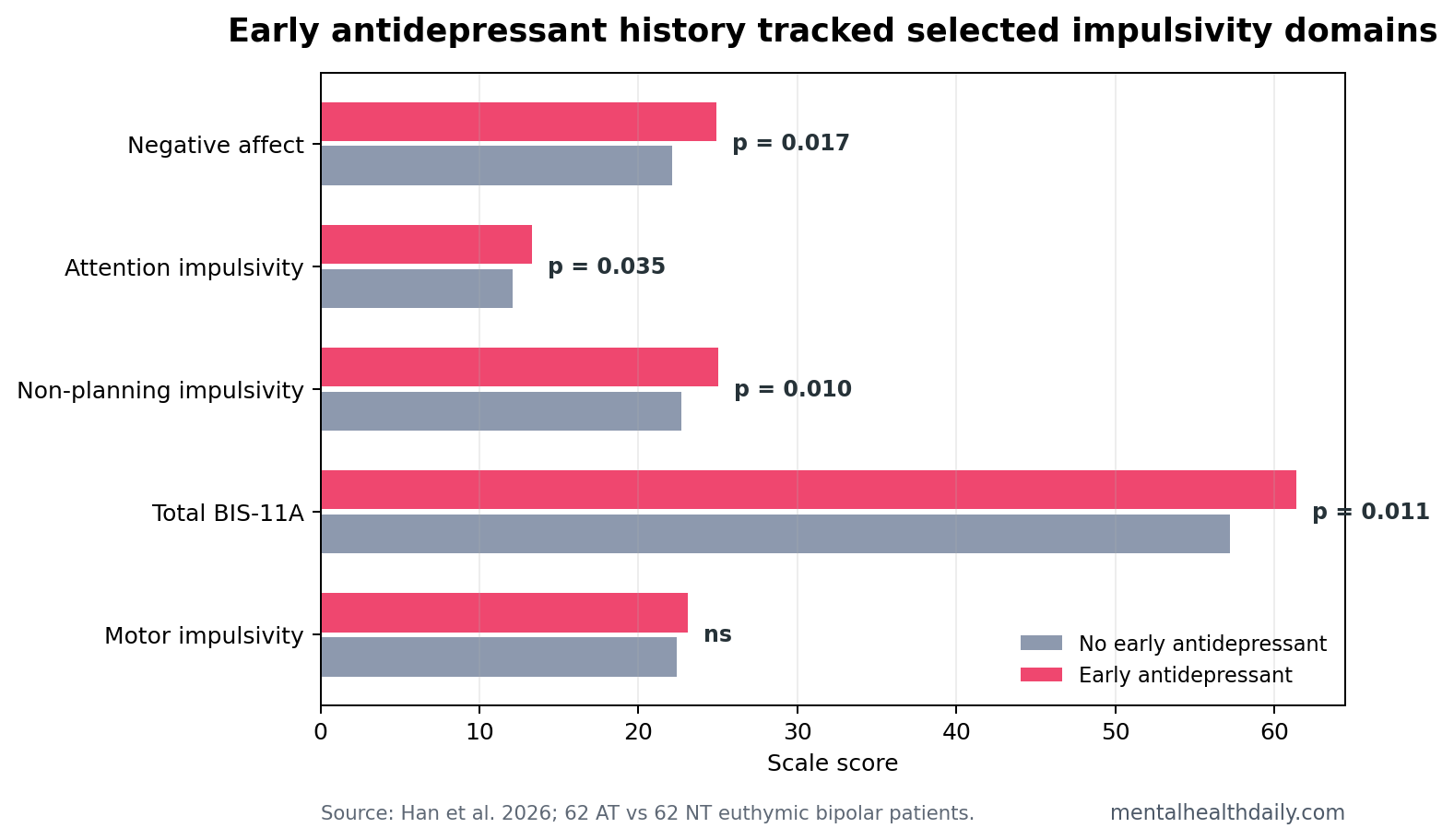
- Negative affect was higher: the early-antidepressant group scored 24.9 ± 6.6 vs. 22.1 ± 6.1 in the no-antidepressant group (p = 0.017).
- Attentional impulsivity increased: BIS-11A attention scores were 13.3 ± 2.9 vs. 12.1 ± 2.8 (p = 0.035).
- Non-planning impulsivity increased: scores were 25.0 ± 4.9 vs. 22.7 ± 4.8 (p = 0.010), with total BIS-11A 61.4 vs. 57.2 (p = 0.011).
- Motor impulsivity did not separate groups: motor scores were 23.1 vs. 22.4 and not statistically significant (p = 0.156).
- Mediation was not confirmed: negative affect correlated with antidepressant history at r = 0.216, but affect did not explain the antidepressant-impulsivity association in mediation models.
Euthymic bipolar disorder means bipolar disorder during a clinically stable period without current mania or major depressive severity. In Han et al., euthymia required Montgomery-Asberg Depression Rating Scale and Young Mania Rating Scale scores below 7 for at least 4 weeks.1
BIS-11A, the Barratt Impulsiveness Scale, measures impulsivity as self-reported tendencies in attention, motor action, and planning. It is useful for trait-like impulsivity, but it is not the same as a laboratory test of risk-taking or response inhibition.
Early Antidepressant History Tracked Attention and Planning, Not Motor Impulsivity
The study compared 62 Han Chinese euthymic bipolar patients with early systematic antidepressant treatment history against 62 without that history. Systematic treatment meant adequate-dose SSRI or SNRI monotherapy for at least 6 weeks during the early depressive-onset stage before bipolar disorder was recognized.
Group differences were selective. Attentional impulsivity and non-planning impulsivity were higher in the antidepressant-history group, and total BIS-11A was higher. Motor impulsivity did not significantly differ.
Clinical translation: the pattern points more toward difficulty sustaining attention and future-oriented planning than toward motor restlessness or action without movement control.
Negative Affect Was Higher, But It Did Not Mediate the Impulsivity Link
The Positive and Negative Affect Scale showed higher negative affect in the antidepressant-history group: 24.9 ± 6.6 vs. 22.1 ± 6.1. Positive affect did not significantly differ at 16.4 vs. 15.9.
Correlation results looked plausible at first glance. Antidepressant use correlated with negative affect (r = 0.216), attentional impulsivity (r = 0.190), non-planning impulsivity (r = 0.228), and total impulsivity (r = 0.245). But mediation modeling did not support a complete path where antidepressant history increased negative affect and negative affect then explained higher impulsivity.
That distinction changes the interpretation. Negative affect and impulsivity were both elevated, but the data did not show that one statistically carried the other. The association may reflect unmeasured illness severity, diagnostic delay, sleep disruption, mixed features, temperament, or medication history rather than a simple affect-to-impulsivity chain.
Antidepressant Exposure May Also Mark Delayed Bipolar Recognition
Many people with bipolar disorder first present with depression, and manic or hypomanic episodes may appear later. That creates a real clinical trap: early depressive episodes can be treated as unipolar depression, especially before bipolar diagnosis is clear.
Han et al. tried to make the groups comparable by matching age, sex, diagnostic delay, mood-stabilizer use, depressive symptoms, and manic symptoms. Even with those controls, retrospective treatment grouping remains vulnerable to confounding. Patients given early antidepressants may have had more severe, more persistent, or more treatment-seeking depression before bipolar disorder was recognized.
Adjacent evidence explains why the signal is still clinically relevant. Network meta-analysis data show that antidepressants can help bipolar depression but must be balanced against switch risk and other treatment classes.2 Berkol et al. reported manic switching in a substantial subgroup exposed to antidepressants, reinforcing that antidepressant history is not neutral in bipolar illness.3
Impulsivity Remains a Bipolar Outcome Even During Remission
Impulsivity during euthymia matters because risky decisions, self-harm vulnerability, spending, substance use, and treatment nonadherence can persist outside acute mood episodes. Titone et al. found day-to-day links between affect and impulsivity in bipolar disorder, supporting a broader model where impulsivity persists beyond acute mania.4
Evidence-strength note: Han et al. cannot prove early antidepressants caused later impulsivity. The best use of the finding is monitoring. Bipolar patients with a history of early antidepressant monotherapy may deserve careful follow-up for residual negative affect, attention-related impulsivity, planning problems, sleep disturbance, and mixed-state warning signs during euthymia.
The treatment implication is not to avoid every antidepressant in every bipolar patient. It is to avoid casual antidepressant monotherapy when bipolar disorder is plausible, track activation and switching risk early, and ask about impulsivity even after mood scales look quiet.
How to Use the Finding Without Overreading It
The safest clinical use is risk history. Early antidepressant monotherapy in someone later diagnosed with bipolar disorder should prompt a careful look at activation history, mixed symptoms, sleep change, impulsivity, and treatment response. It should not be used as proof that the medication caused every later problem.
Initial presentation: depressive-onset bipolar disorder can look indistinguishable from unipolar depression early on. Family history, early age at onset, episodic sleep reduction, antidepressant activation, mixed irritability, and recurrent brief depressions can raise suspicion, but none are perfect.
Monitoring target: the 2026 paper points to attention and planning domains. Questions about distractibility, unfinished tasks, risky spending, abrupt decisions, driving behavior, substance use, and difficulty delaying rewards may be more informative than asking only whether mood is currently depressed or manic.
Research gap: a stronger design would follow depressive-onset patients prospectively, record antidepressant dose and duration, document emerging hypomanic symptoms, and then compare later bipolar-diagnosed groups on both self-report and behavioral impulsivity tasks.
The article’s practical boundary is narrow: early antidepressant history is a useful marker for follow-up in bipolar disorder. It is not enough to make a causal claim without prospective data.
Inference boundary: the result supports subgroup monitoring rather than retrospective blame. In people later recognized as having bipolar disorder, early antidepressant monotherapy may identify a subgroup whose later euthymic state is not fully captured by mood-scale remission.
Bipolar depression still needs active treatment. The practical question is which treatment plan controls depression while minimizing activation, switching risk, sleep disruption, and residual impulsivity.
Why the distinction matters: a patient can have low mania and depression scores while still reporting distractibility, short planning horizon, emotional reactivity, or decisions that create downstream problems. Those are not the same outcome as relapse, but they can affect adherence, relationships, money, sleep, substance use, and safety planning. That is why the 2026 finding belongs in follow-up conversations rather than in a simple antidepressant-for-or-against argument.
Residual Impulsivity Can Hide Behind Normal Mood Scores
One useful detail in Han et al. is that groups did not differ on current depression or mania scale scores, yet impulsivity and negative affect still separated them.1 That means a patient can look euthymic by standard mood scales while still carrying attention, planning, or affective-instability problems that matter in daily life.
Clinical questions: screening should move beyond “Are you depressed?” and “Are you manic?” In a patient with bipolar disorder and early antidepressant exposure, it is reasonable to ask whether they interrupt tasks, make abrupt purchases, drive aggressively, escalate conflicts, miss sleep after emotional events, or struggle to plan the next week.
Medication context: the study does not say that every SSRI or SNRI exposure is harmful. It says that early systematic monotherapy history identified a subgroup with higher selected impulsivity during euthymia. The management response should be careful longitudinal monitoring, not retrospective blame.
That makes the paper useful despite its design limits. It turns a common clinical history into a follow-up target: depressive-onset bipolar disorder treated early with antidepressants may require attention to impulsivity even after mood symptoms appear controlled.
For research, the missing piece is objective behavior. Self-report impulsivity can be influenced by insight, current affect, personality, and recall. Adding delay-discounting tasks, stop-signal tasks, sleep data, and longitudinal mood tracking would clarify whether early antidepressant exposure predicts measurable decision-making changes or mainly self-perceived impulsivity.
Those additions would also help distinguish medication history from illness trajectory. A patient exposed to antidepressants early may differ from an unexposed patient before the prescription was ever written.
That baseline difference is the central uncertainty in the study, and it is exactly why prospective follow-up with baseline symptom data matters.
Questions About Early Antidepressants and Bipolar Impulsivity
Does this prove antidepressants caused higher impulsivity?
No. The study was cross-sectional and grouped patients by treatment history. Early antidepressant use may mark delayed bipolar diagnosis or more severe early depression.
Which impulsivity domains differed?
Attention and non-planning impulsivity differed, and total BIS-11A differed. Motor impulsivity did not significantly separate the groups.
What should clinicians or patients monitor?
Residual negative affect, sleep disruption, activation, planning problems, risky decisions, and mixed-state symptoms are the practical monitoring targets when bipolar disorder and antidepressant exposure intersect.
References
- Han D, Cui P, Wang M, et al. A cross-sectional study on the impact of early systematic antidepressant therapy on positive/negative affect and impulsivity in euthymic bipolar disorder patients. PLOS One. 2026;21(4):e0346872. https://doi.org/10.1371/journal.pone.0346872
- Yildiz A, et al. Pharmacological treatment of bipolar depression: a systematic review and network meta-analysis. The Lancet Psychiatry. 2023. https://doi.org/10.1016/s2215-0366(23)00199-2
- Berkol TD, et al. Antidepressant use and manic switch in bipolar disorder. Neurosciences. 2019. https://doi.org/10.17712/nsj.2019.1.20180008
- Titone MK, et al. Daily affect and impulsivity in bipolar disorder. International Journal of Bipolar Disorders. 2022. https://doi.org/10.1186/s40345-022-00270-8