A 2026 meta-analysis of 4 randomized trials found that GLP-1 receptor agonists reduced obstructive sleep apnea severity by 13.89 apnea-hypopnea events per hour compared with placebo, alongside 12.46 kg more weight loss than placebo.1 The effect looks clinically meaningful for obesity-linked sleep apnea, but high heterogeneity means the result should not be flattened into “GLP-1 drugs replace CPAP.”
Research Highlights
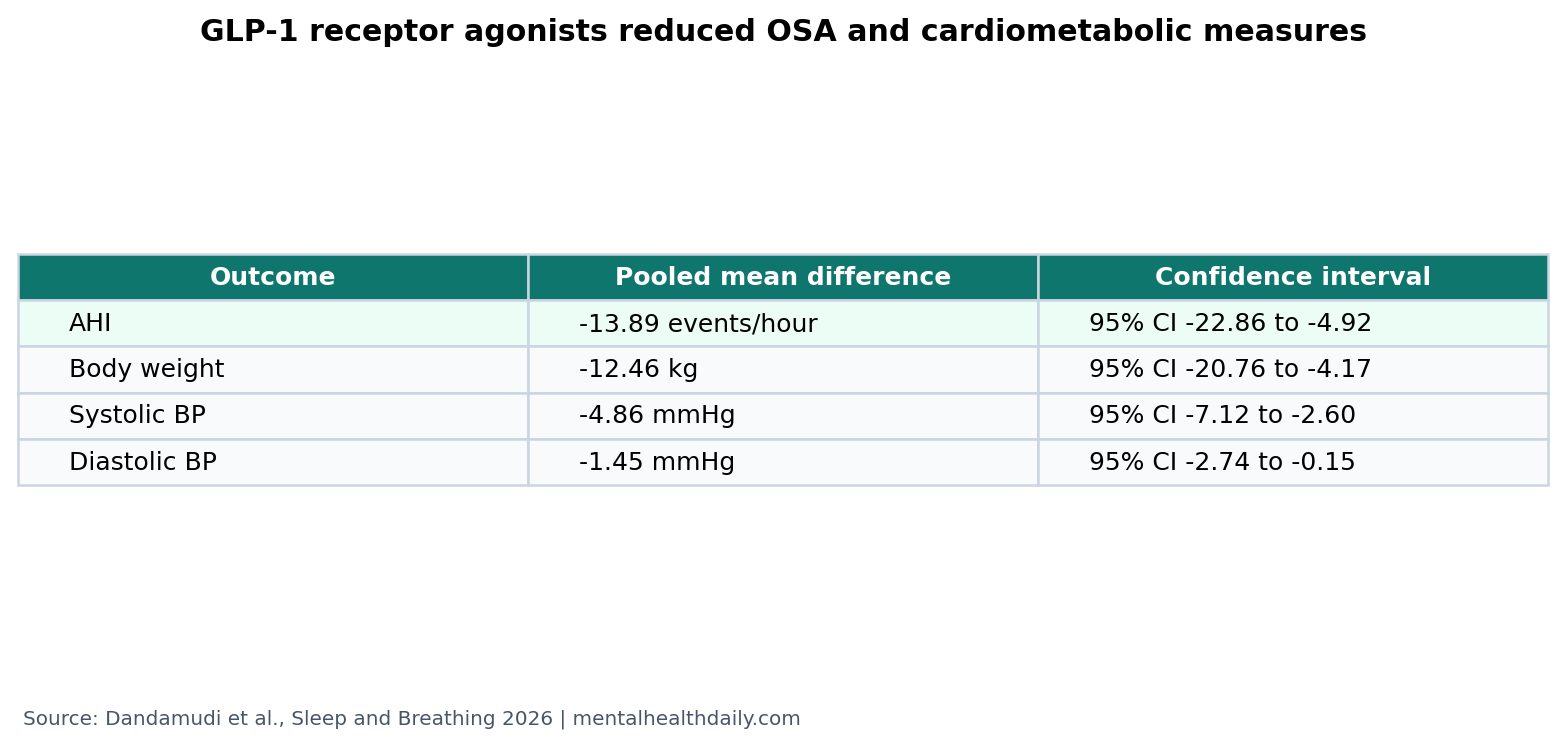
- Sleep apnea severity fell: GLP-1 receptor agonists reduced AHI by 13.89 events/hour (95% CI 4.92 to 22.86 fewer events/hour; p < 0.01).1
- Weight loss was substantial: pooled body weight fell by 12.46 kg more than placebo, likely contributing to airway improvement.1
- Blood pressure also moved: systolic pressure fell by 4.86 mmHg and diastolic pressure by 1.45 mmHg versus placebo.1
- Tirzepatide reduced AHI more than liraglutide: subgroup AHI reduction was 23.80 events/hour for tirzepatide vs. 5.20 events/hour for liraglutide.1
- Certainty is not uniform: AHI heterogeneity was high (I2 = 92.7%), so patient phenotype and drug class probably matter.1
Obstructive sleep apnea means repeated airway collapse during sleep. The main severity metric is the apnea-hypopnea index (AHI), the number of complete or partial breathing interruptions per hour of sleep. AHI is not the whole disease, but it is the central trial endpoint for breathing-event burden.
GLP-1 receptor agonists are incretin-based drugs that increase satiety, reduce food intake, and improve metabolic measures. Liraglutide is a GLP-1 receptor agonist; tirzepatide is a dual GIP/GLP-1 receptor agonist. Their sleep-apnea relevance is mostly through weight loss, though inflammation, fluid shifts, and upper-airway mechanics may also contribute.
AHI Fell by 13.89 Events per Hour Across 4 RCTs
Dandamudi et al. pooled randomized controlled trials comparing GLP-1 receptor agonist therapy with placebo in patients with obstructive sleep apnea. The primary outcome was change in AHI. The pooled mean difference was −13.89 events/hour (95% CI −22.86 to −4.92; p < 0.01).1
Mean difference means the average change in the treatment group minus the average change in the placebo group. A negative AHI mean difference is favorable because fewer breathing interruptions per hour is better.
The size of the AHI drop is clinically relevant. A patient starting near the moderate-to-severe boundary could move meaningfully, and a patient with severe obesity-linked OSA could reduce event burden even if they still need CPAP or another airway-focused intervention.
Weight Loss Is Probably the Main Sleep-Apnea Pathway
Body weight fell by 12.46 kg more with GLP-1 receptor agonists than placebo (95% CI −20.76 to −4.17; p < 0.01).1 That matters because obesity increases upper-airway collapsibility, reduces lung volume, and can worsen pharyngeal fat deposition.
Earlier OSA physiology work has treated obesity as a major driver of airway obstruction, while not the only driver.4 Tongue size, craniofacial anatomy, arousal threshold, neuromuscular compensation, nasal obstruction, alcohol use, sedatives, and sleep position can all shape the actual breathing-event burden.
Clinical implication: GLP-1 drugs make the most sense as OSA therapy when excess weight is a major part of the phenotype. A lean patient with craniofacial narrowing or high loop gain is less likely to match the trial signal.
Tirzepatide Drove a Larger AHI Reduction Than Liraglutide
Subgroup analysis separated liraglutide and tirzepatide. Liraglutide-based interventions reduced AHI by 5.20 events/hour (95% CI −7.89 to −2.51; p < 0.01). Tirzepatide reduced AHI by 23.80 events/hour (95% CI −29.62 to −17.98; p < 0.01), with a significant subgroup difference favoring tirzepatide (p < 0.0001).1
Blackman et al. had already shown that liraglutide 3.0 mg improved OSA severity in adults with obesity.2 Malhotra et al. later showed larger effects for tirzepatide in obstructive sleep apnea and obesity, including AHI reductions and weight loss over 52 weeks.3
Calibrated read: the direction favors tirzepatide, but the evidence comes from subgrouped trial data rather than a large head-to-head meta-analysis. Drug class, baseline AHI, baseline BMI, CPAP use, and trial duration all complicate a simple drug-ranking claim.
Blood Pressure Improved, but Heterogeneity Stayed High
Systolic blood pressure fell by 4.86 mmHg (95% CI −7.12 to −2.60; p < 0.01), while diastolic blood pressure fell by 1.45 mmHg (95% CI −2.74 to −0.15; p = 0.03).1 These are useful cardiometabolic co-benefits, especially because OSA and obesity often travel with hypertension.
AHI heterogeneity was severe (I2 = 92.7%), and body-weight heterogeneity was even higher (I2 = 99.1%). Heterogeneity means the included trials disagreed substantially on effect size. A large average effect can still be real, but the average is less predictive for any one patient when trial results vary widely.
Practical sorting: future OSA trials should report baseline BMI, visceral adiposity, neck circumference, CPAP adherence, oxygen desaturation, sleepiness scores, and whether AHI improvement tracks weight loss or other pathways. AHI alone leaves the responder phenotype unclear.
GLP-1 Drugs Do Not Automatically Replace Airway Treatment
CPAP means continuous positive airway pressure, a device that keeps the upper airway open during sleep. It is still the standard mechanical treatment for many patients with moderate-to-severe OSA. GLP-1 therapy changes metabolic and weight drivers; CPAP directly splints the airway.
Optimal management may include both when the patient has obesity-linked OSA and clinically important breathing events. Weight loss can lower the required pressure, improve symptoms, reduce cardiometabolic risk, or move some patients below a treatment threshold. It does not guarantee that airway collapse disappears.
Supported: GLP-1 receptor agonists reduced AHI, weight, and blood pressure in randomized trials involving OSA and obesity.
Not supported: unsupervised CPAP discontinuation, use in every OSA phenotype, or certainty that semaglutide would match tirzepatide because this meta-analysis was driven mainly by liraglutide and tirzepatide trial data.
Sleep-Apnea Phenotype Should Decide How Much the Result Applies
OSA is a syndrome with multiple routes to the same AHI number. In one patient, airway collapse may be driven mainly by obesity and upper-airway fat. In another, craniofacial anatomy, nasal obstruction, alcohol use, sedative medication, unstable ventilatory control, or poor neuromuscular compensation may dominate.
That distinction changes how to read the GLP-1 result. A large weight-loss drug should help most when weight is a major causal driver. It may help less when body weight is secondary or when sleep apnea persists because of airway anatomy that weight loss cannot fully reverse.
Clinical sorting: the right follow-up test after substantial weight loss is usually repeat sleep measurement, not guesswork. Symptoms can improve while residual AHI remains high enough to need treatment.
High Heterogeneity Should Shape Expectations
AHI heterogeneity of I2 = 92.7% means the trials did not produce one uniform effect size. Some of that disagreement probably reflects drug differences, because tirzepatide produced larger weight loss and larger AHI reductions than liraglutide. Some may reflect baseline severity, CPAP use, diabetes status, trial duration, adherence, and how sleep was measured.
Evidence-strength note: this is randomized evidence, but it is still a 4-trial meta-analysis rather than a large mature drug-class literature. The pooled result supports GLP-1-based therapy as a serious OSA modifier in adults with obesity; it does not pin down which patients can avoid device therapy, which drug dose is best for sleep outcomes, or how durable the AHI change remains after weight plateaus.1
That limitation is especially relevant because OSA biology is mechanical as well as metabolic. Weight loss can reduce neck circumference, pharyngeal fat, and lung-volume loading, but airway anatomy and ventilatory-control traits can keep AHI elevated after large weight change.4 Repeat testing after major weight loss is the evidence-based bridge between the drug response and any CPAP or oral-appliance decision.
The average effect is still useful. It says GLP-1-based therapy can meaningfully reduce OSA severity in the studied populations. It does not say every patient should expect exactly 13.89 fewer breathing events per hour.
Best clinical read: GLP-1 therapy is a disease-modifying weight-loss tool for obesity-linked OSA. It belongs in a phenotype-based plan that can include CPAP, oral appliances, positional therapy, alcohol reduction, medication review, and surgery when appropriate.
That framing also protects patients from overcorrection: effective weight loss can reduce airway burden while residual sleep apnea still needs direct treatment.
Questions About GLP-1 Drugs and Sleep Apnea
Can GLP-1 drugs treat obstructive sleep apnea?
They can reduce AHI in obesity-linked OSA trials. Whether they are enough without CPAP depends on baseline severity, anatomy, symptoms, oxygen desaturation, and repeat sleep testing.
Why did tirzepatide look stronger than liraglutide?
Tirzepatide generally produces larger weight loss than older GLP-1 monotherapy. In the pooled OSA analysis, the AHI reduction was also larger, but trial differences make direct ranking cautious.
Should someone stop CPAP after losing weight on a GLP-1 drug?
No. CPAP changes should be based on symptoms, clinician guidance, and repeat sleep testing. Weight loss can reduce OSA severity without eliminating it.
What outcome matters besides AHI?
Daytime sleepiness, blood pressure, oxygen desaturation, arrhythmia risk, adherence, and quality of life all matter. AHI is central, but it is not the whole clinical picture.
References
- Dandamudi V, et al. Efficacy of GLP-1 receptor agonists in the treatment of obstructive sleep apnea: a systematic review and meta-analysis of cardiometabolic and sleep outcomes. Sleep and Breathing. 2026. doi:10.1007/s11325-026-03681-4
- Blackman A, Foster GD, Zammit G, et al. Effect of liraglutide 3.0 mg in individuals with obesity and moderate or severe obstructive sleep apnea. International Journal of Obesity. 2016. doi:10.1038/ijo.2016.52
- Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the treatment of obstructive sleep apnea and obesity. New England Journal of Medicine. 2024. doi:10.1056/nejmoa2404881
- Schwartz AR, Patil SP, Laffan AM, Polotsky V, Schneider H, Smith PL. Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proceedings of the American Thoracic Society. 2008. doi:10.1513/pats.200708-137mg