Dementia rates in the US, UK, Netherlands, Sweden, France, and several other high-income countries have been falling for decades, despite population aging. The standard explanation — improved cardiovascular care, more education, and less smoking in later-born cohorts — is real but incomplete.
Research Highlights
- Dementia incidence has been falling about 13% per decade in Western cohorts — documented across multiple high-income meta-analyses, but the mechanism behind the decline has been disputed for years.2
- The Fjell 2026 analysis of ~219,000 adults followed for up to 30 years finds a “double dividend”: later-born cohorts enter old age with higher memory and decline more slowly. Each decade of later birth adds 0.54 words to memory level and shaves 0.07 words/year off the rate of decline.1
- The biggest gains are concentrated in the worst decliners. Quantile regression shows the cohort effect is roughly twice as large at the 10th percentile (the people most likely to cross the dementia threshold) as at the median.1
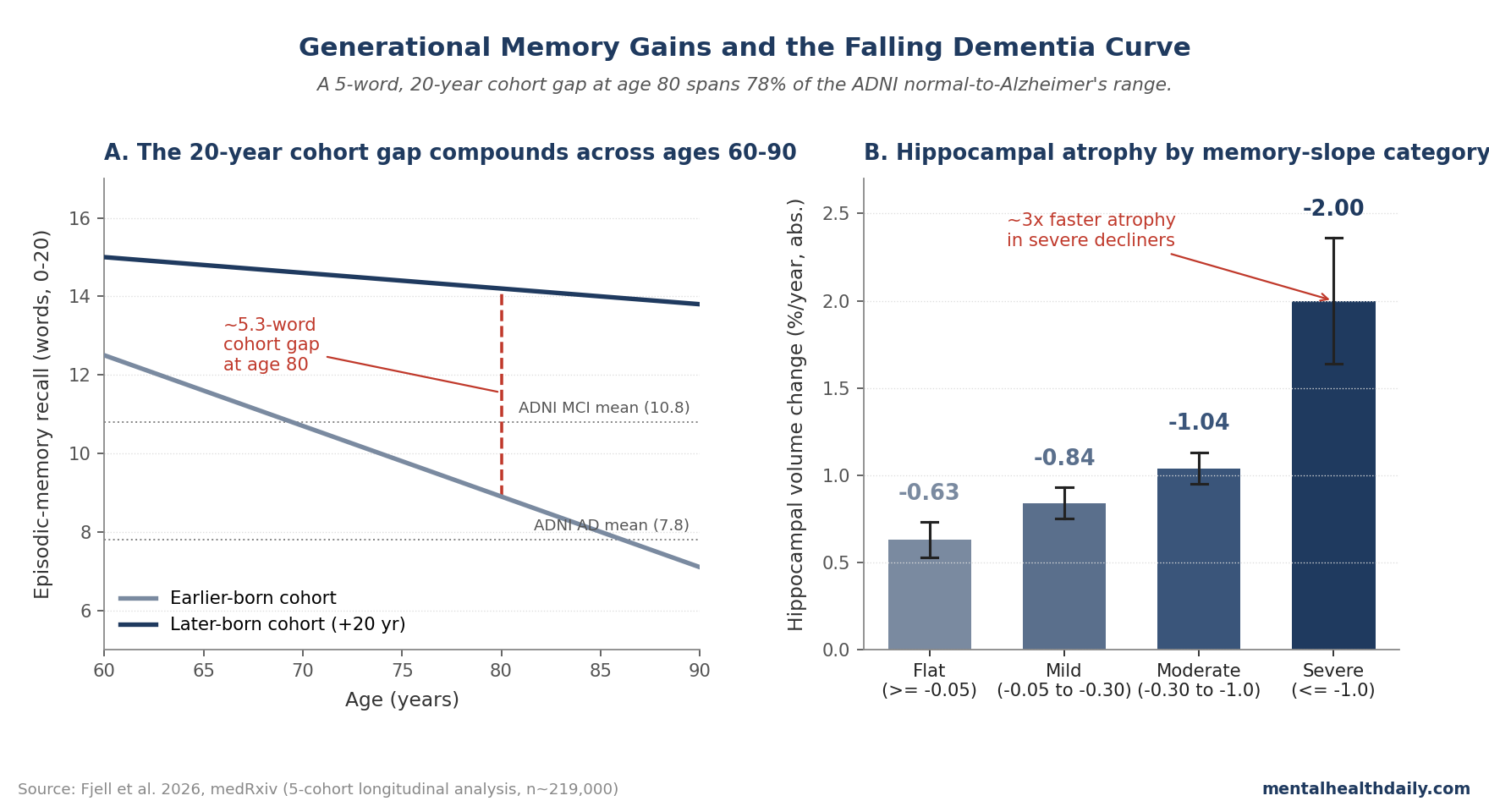
- The 5-word cohort gap at age 80 is clinically large. It represents 78% of the gap between cognitively normal and Alzheimer’s-diagnosed adults in ADNI, and matches the magnitude of the observed dementia-incidence drop.1
- Memory-slope groups tracked hippocampal atrophy. Severe decliners lost hippocampal volume at −2.00%/year vs. −0.63% in flat decliners — about 3x faster — tying the cohort effect to a real neurodegenerative gradient rather than a measurement artifact.1
The Lancet Commission frames roughly 45% of dementia as potentially modifiable through lifestyle and environmental change,3 and most coverage attributes the falling rates to changes operating within old age. A 2026 analysis by Fjell et al. reframes the question.
Using ~783,000 episodic-memory assessments across five major longitudinal cohorts in Europe and the US, it shows that later-born adults are entering their 70s and 80s with materially better memory than earlier-born adults at the same age — and once there, they lose memory more slowly. Both effects compound, and the combined cohort advantage at age 80 is large enough to plausibly account for the entire observed dementia-incidence decline.1
Later-Born Cohorts Had Higher Memory and Slower Decline
The 2026 study pooled five longitudinal cohorts: the Health and Retirement Study (HRS, US), the English Longitudinal Study of Aging (ELSA), the Survey of Health, Aging and Retirement in Europe (SHARE, ~30 countries), the Irish Longitudinal Study on Aging (TILDA), and the Longitudinal Aging Study Amsterdam (LASA).1 All used comparable verbal episodic-memory measures (10-word list, immediate and delayed recall) repeated across waves, allowing per-person trajectories.
The headline analysis tracked two summary statistics per participant: a memory level estimate at mid-age, and a memory slope — the rate of change in words recalled per year — computed via Theil-Sen regression (the median of all pairwise slopes, which resists outliers). After adjustment for age and study, two cohort effects emerged consistently:
- One decade of later birth was associated with 0.54 additional words of memory level (95% CI 0.49–0.59, p < 0.001).1
- One decade of later birth was associated with a 0.070 word/year shallower decline rate (95% CI 0.063–0.077, p < 0.001).1
These effects are additive over time. Two cohorts born 20 years apart would, on the model’s projection, differ by roughly 2.5 words at age 60 and ~5.0 words at age 80 — the level gap (47% of the total) gets reinforced by the slope advantage (53%) as the later-born cohort accumulates fewer years of fast decline.1
Why 5 Words at Age 80 Is Clinically Large
To anchor the cohort gap to dementia thresholds, Fjell calibrated the memory measure against the Alzheimer’s Disease Neuroimaging Initiative (ADNI) reference data. On the same 0–20 word-recall metric used throughout the paper, ADNI mean scores were 14.2 words for cognitively normal (CN), 10.8 for mild cognitive impairment (MCI), and 7.8 for Alzheimer’s disease (AD).1 Diagnostic discrimination was excellent (AUC 0.959 for CN vs. AD).
The 20-year cohort advantage of 5.0 words spans 78% of the CN–AD gap and exceeds the gap between CN and the pooled MCI+AD group.1 Translated literally: a person born in 1940 who scored at the MCI boundary in their late 70s would, if instead born in 1960, be expected to score in the cognitively normal range at the same age.
The documented incidence trend — pooled across studies in the US, UK, and Western Europe — is roughly a 13% per-decade reduction in age-standardized dementia incidence between 1990 and 2015, corresponding to about 7 fewer dementia diagnoses per 1,000 person-years among 75–79 year-olds.2 Wolters et al.’ 2020 individual-participant meta-analysis put the per-decade incidence reduction at 13%, the same figure Fjell’s calibration matches.4
The Gain Is Concentrated Among the Worst Decliners
The most clinically interesting structural finding is not that average memory has improved. It is that the cohort improvement is disproportionately concentrated in the left tail of the slope distribution, exactly where the people who would otherwise cross dementia thresholds live.
Quantile regression across the full slope distribution showed the cohort effect at the 10th percentile (the most rapidly declining individuals) was roughly twice the median effect: 0.104 words/year per decade of birth at the 10th percentile vs. 0.053 at the median (both p < 0.001).1 The pattern held when participants who died within 2 years of their last observation were excluded, ruling out terminal-decline contamination.
A complementary “bouts” analysis — identifying periods of stable cognition vs. accelerated loss within each person’s trajectory — converged on the same pattern:
- Stable bouts became more common in later cohorts. Each decade of later birth raised the odds of being in a stable period by 64% (OR 1.64, 95% CI 1.59–1.68, p < 0.001).1
- Steep-decline trajectories became less common. Each decade of later birth was associated with 38% lower odds of meeting steep-decline criteria (slope ≤ −1.0 word/year; OR 0.62, 95% CI 0.55–0.70, p < 0.001).1
Later-born cohorts spent more years stable and fewer years in accelerated cognitive loss. The headline 0.07 words/year/decade slope effect, averaged across the population, understates the gain among people who would otherwise drive the largest share of dementia incidence.
Hippocampal Atrophy Tracks the Slope Categories
One reasonable concern about cohort-effect papers is that the apparent improvement could reflect measurement artifacts (better-educated cohorts being more practiced at word lists, for example) rather than meaningful neurobiological change. Fjell addresses this with an independent MRI sub-sample of 1,925 participants with longitudinal hippocampal volume measurements (median follow-up 4.1 years).
Hippocampal atrophy followed a monotone gradient across the memory-slope categories used throughout the paper:1
- Flat decliners (slope ≥ −0.05 words/year): −0.63%/year hippocampal volume change (95% CI −0.73 to −0.53).
- Moderate decliners (−0.30 to −1.0 words/year): −1.04%/year (−1.13 to −0.95).
- Severe decliners (≤ −1.0 words/year): −2.00%/year (−2.36 to −1.64) — about 3x faster atrophy than flat decliners.
The slope categories aren’t statistical fictions. They map onto a real neurodegenerative gradient in a memory-critical brain structure, which strengthens the case that the cohort-related slope shift reflects meaningful biology rather than only test-taking sophistication.
Cognitive impairment classification showed the same pattern. Impairment rates rose from 3.0% among flat decliners to 34.5% among severe decliners.
After adjusting for age, each additional word/year of steeper decline was associated with an 86% reduction in the odds of remaining cognitively normal (OR 0.14, 95% CI 0.12–0.17, p < 0.001).1 Once slope was adjusted for, the cohort signal disappeared (slope-adjusted OR 1.04, 95% CI 0.91–1.20, p = 0.55).
Calibration Limits for Falling Dementia Rates
The dominant narrative attributes the dementia decline to lifestyle and treatment improvements that operate within old age: better blood pressure control, statin uptake, lower smoking rates, treatment of midlife hearing loss, and so on. The 2024 Lancet Commission lists 14 modifiable risk factors covering an estimated 45% of dementia risk.3
That story is not wrong, but it’s incomplete. The Fjell decomposition shows that roughly half of the cohort advantage at age 80 sits in the level component — the memory people arrive in old age with — not in the slope component. Level differences are dominated by early- and midlife conditions: education, childhood health, occupational complexity, perinatal nutrition, and broader cognitive-reserve factors.7 These were locked in decades before the at-risk period.
Several adjacent literatures support this split:
- Cognitive reserve: education, occupational complexity, and cumulative cognitive engagement can raise the threshold at which Alzheimer’s pathology produces symptomatic dementia.7
- Flynn-effect evidence: SHARE, HRS, and twin-study analyses have found cohort gains in later-life cognition that are better explained by environment than genetics.89
- Vascular prevention: better blood pressure, lipid, diabetes, smoking, and exercise profiles plausibly slow the slope component of mixed vascular-Alzheimer’s decline.10
Lifestyle and treatment improvements in old age are real, but Fjell’s decomposition implies they explain only part of the observed decline. The rest sits in the higher cognitive starting point later-born cohorts bring into their 60s and 70s.
Limitations of the Fjell Synthesis
The estimates are upper bounds on cohort effects. Cohort, period, and age effects are mathematically confounded in any longitudinal-cross-sectional dataset. The headline 0.54 words/decade level estimate assumes the period drift across calendar time is zero; if some cohort-looking signal is really a period effect, the cohort component shrinks.
Fjell’s bounding analysis shows the qualitative result — a meaningful cohort advantage — survives across plausible period assumptions, but the precise size is uncertain.
Selective attrition cuts the other way. The main analysis required at least 4 observations per participant to get reliable per-person slopes. People who decline fastest are also most likely to drop out before completing 4 waves, which could bias the slope estimates toward optimism. Inverse-probability reweighting and replication with the ≥2-wave sample reproduced the cohort ordering, but the specific magnitudes could shift.
Verbal memory is one cognitive domain. The paper analyzes word-list recall, the most-validated single predictor of Alzheimer’s-related decline.11 Whether comparable cohort gains exist for executive function, processing speed, and visuospatial domains is an open question, and existing data are mixed — some domains show cohort gains, others show losses.
The “postponement” framing matters. Fjell explicitly notes that the generational advantage shifts dementia onset to higher ages but does not eliminate cumulative cognitive loss. A 1960-born cohort might cross the same impairment threshold roughly a decade later than the 1940-born cohort — valuable, but not a structural elimination of the disease.1
Midlife Reserve and Late-Life Vascular Health Both Shape Dementia Risk
The Fjell paper is not a clinical intervention trial, but it clarifies what individual-level interventions can plausibly target. Education, occupational complexity, midlife cardiovascular health, and broader environmental conditions appear to set the level component of late-life memory. Interventions launched in the 70s can still affect the slope, but they cannot fully recreate the starting reserve built decades earlier.
For most adults, the directly modifiable contributors in adulthood — cardiovascular control, hearing aids, physical activity, depression treatment, sleep, and ongoing cognitive engagement — operate primarily on the rate of decline. Cognitive engagement and education in midlife matter for reserve; cardiovascular and lifestyle work in late life matter for slope. Both compound.
Questions About Falling Dementia Rates
Are dementia rates actually falling, or is that a measurement artifact?
Falling. Multiple individual-participant meta-analyses put the per-decade reduction at roughly 13%.4 Total dementia counts are still rising because populations are aging, but the rate per person at a given age has dropped.
Does this mean dementia is preventable?
Postponable, more accurately. The cohort advantage shifts dementia onset to higher ages but does not eliminate the eventual accumulation of cognitive loss. The 2024 Lancet Commission estimates roughly 45% of dementia could be prevented or delayed through 14 modifiable risk factors,3 which is consistent with Fjell’s framing — the achievable share is large, but not 100%.
References
- Generational gains in memory capacity and stability may account for declining dementia incidence rates in Europe and the United States. Fjell AM et al. medRxiv. 2026 (preprint). doi:10.64898/2026.04.14.26350835
- A Comparison of the Prevalence of Dementia in the United States in 2000 and 2012. Langa KM et al. JAMA Internal Medicine. 2017;177(1):51-58. doi:10.1001/jamainternmed.2016.6807
- Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Livingston G et al. The Lancet. 2024;404(10452):572-628. doi:10.1016/s0140-6736(24)01296-0
- Twenty-seven-year time trends in dementia incidence in Europe and the United States. Wolters FJ et al. Neurology. 2020;95(5):e519-e531. doi:10.1212/wnl.0000000000010022
- The Flynn Effect: A Meta-analysis. Trahan LH et al. Psychological Bulletin. 2014;140(5):1332-1360. doi:10.1037/a0037173
- Trends in the prevalence and mortality of cognitive impairment in the United States. Langa KM, Larson EB, Karlawish JH et al. Alzheimer’s & Dementia. 2008;4(2):134-144. doi:10.1016/j.jalz.2008.01.001
- Cognitive reserve in ageing and Alzheimer’s disease. Stern Y. The Lancet Neurology. 2012;11(11):1006-1012. doi:10.1016/s1474-4422(12)70191-6
- Variations in Cognitive Functioning as a Refined Approach to Comparing Aging Across Countries. Skirbekk V, Loichinger E, Weber D. PNAS. 2012;109(3):770-774. doi:10.1073/pnas.1112173109
- The Flynn effect across subgroups: A study of cognition. Bratsberg B, Rogeberg O. PNAS. 2018;115(26):6674-6678. doi:10.1073/pnas.1718793115
- Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals. Gorelick PB et al. Stroke. 2011;42(9):2672-2713. doi:10.1161/str.0b013e3182299496
- Episodic memory loss is related to hippocampal-mediated beta-amyloid deposition in elderly subjects. Mormino EC et al. Brain. 2009;132(5):1310-1323. doi:10.1093/brain/awn320
- Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050. GBD 2019 Dementia Forecasting Collaborators. The Lancet Public Health. 2022;7(2):e105-e125. doi:10.1016/s2468-2667(21)00249-8
- Flynn effect and its reversal are both environmentally caused. Bratsberg B, Rogeberg O. PNAS. 2018;115(26):6674-6678. doi:10.1073/pnas.1718793115
- Prevalence of Cerebral Amyloid Pathology in Persons Without Dementia: A Meta-analysis. Jansen WJ et al. JAMA. 2015;313(19):1924-1938. doi:10.1001/jama.2015.4668