A 2026 medRxiv preprint involving 44 people with chronic post-stroke aphasia found reduced performance on nonverbal false-belief tasks in 23% of participants on the Reality-Unknown task and 36% on the Reality-Known task, with accuracy tied more clearly to cerebral microbleed burden than to aphasia severity.1 The result reframes social-cognitive testing after stroke as a vascular brain-health problem as well as a language-severity problem.
Research Highlights
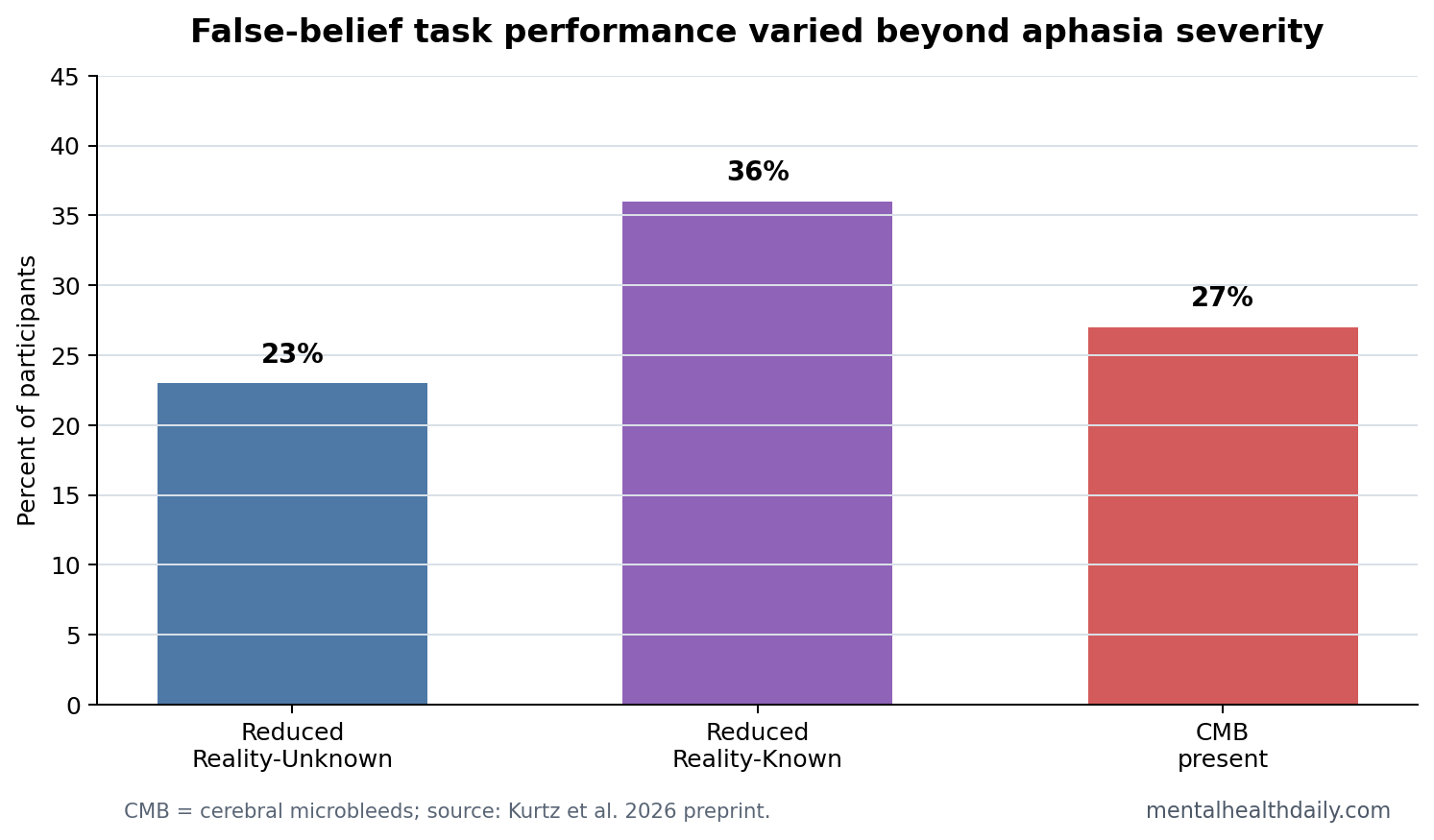
- Low performance was common: Reduced task performance appeared in 23% of participants on Reality-Unknown and 36% on Reality-Known false-belief tasks.1
- Aphasia severity did not explain accuracy: WAB-R Aphasia Quotient scores were not associated with Reality-Unknown accuracy, p = 0.34, or Reality-Known accuracy, p = 0.58.1
- Microbleed count was the strongest vascular signal: Higher cerebral microbleed count predicted lower accuracy on both tasks, Reality-Unknown p = 0.002 and Reality-Known p < 0.001, with q = 0.02 for both.1
- Basal ganglia EPVS also mattered: Higher basal ganglia enlarged perivascular spaces predicted lower Reality-Unknown accuracy after FDR correction, p = 0.01, q = 0.03.1
- Evidence strength is limited: This was a preprint, cross-sectional study with CSVD imaging in a subset, so it can support association but not causality or clinical screening rules.1
Theory of Mind means the ability to infer another person’s beliefs, intentions, or knowledge, including when that person’s belief differs from reality. In stroke research, poor Theory of Mind task performance can reflect social reasoning, executive control, language demands, visual attention, or broader brain health.
Cerebral small vessel disease (CSVD) is damage to small brain blood vessels that can show up on MRI as white matter hyperintensities, lacunes, enlarged perivascular spaces, or cerebral microbleeds. These markers often affect executive function and processing speed, which can matter for social-cognitive tasks.
44 People With Aphasia Completed Nonverbal False-Belief Tasks
Kurtz et al. studied 44 people with chronic post-stroke aphasia due to left-hemisphere stroke. Mean age was 59.07 years, mean education was 15.84 years, and mean Western Aphasia Battery-Revised Aphasia Quotient was 81.84, with a wide range from 31.5 to 100.1
Nonverbal false-belief tasks use silent videos or picture-based scenarios to reduce language demands. The Reality-Unknown task tested spontaneous perspective-taking with lower inhibition demands because participants did not know the object’s original location. The Reality-Known task required self-perspective inhibition because participants knew reality and had to answer from the character’s mistaken belief.
The task split is important. A person can fail a false-belief task because belief reasoning is impaired, because inhibition is weak, because working memory is strained, or because vascular disease reduces the support systems needed to perform the task. The preprint was designed around that ambiguity rather than treating every low score as a pure social-cognition deficit.
Aphasia Severity Was Not the Main Signal
Aphasia severity did not significantly predict task accuracy. WAB-R AQ was not associated with Reality-Unknown performance, p = 0.34, or Reality-Known performance, p = 0.58. That weakens the simple explanation that lower false-belief task performance merely reflects language impairment.
Clinical interpretation: aphasia can still complicate testing and communication, but a nonverbal social-cognition score should not be interpreted only through naming, fluency, or comprehension severity. Other cognitive and vascular variables may be doing real work.
Cerebral Microbleeds Predicted Lower False-Belief Accuracy
Among CSVD markers, cerebral microbleed count showed the clearest association. Microbleeds were present in 9 of 32 participants with available data, or 27%. Higher microbleed count predicted lower Reality-Unknown accuracy, p = 0.002, q = 0.02, and lower Reality-Known accuracy, p < 0.001, q = 0.02.1
Cerebral microbleeds are small deposits of blood-breakdown products visible on susceptibility-sensitive MRI. In this context, they can mark diffuse vascular injury that affects executive systems needed for complex social inference.
Basal ganglia enlarged perivascular spaces also predicted lower Reality-Unknown accuracy after false-discovery-rate correction, p = 0.01, q = 0.03. The Reality-Known association was nominal, p = 0.02, q = 0.06. White matter hyperintensity ratings and total CSVD score were less consistent in this relatively younger stroke sample.
Reality-Known Placed More Demand on Inhibition
The Reality-Unknown and Reality-Known tasks separated 2 versions of belief reasoning. In Reality-Unknown trials, participants had to infer a character’s false belief without directly knowing the object’s true initial location. In Reality-Known trials, participants knew the object’s actual location and had to suppress their own knowledge to answer from the character’s perspective.
Reality-Unknown: lower performance suggests difficulty using another person’s belief to infer reality, but the task reduces self-perspective conflict.
Reality-Known: lower performance can reflect belief reasoning plus inhibition, working memory, and cognitive flexibility. The higher low-performance rate, 36% vs. 23%, fits the added executive burden.
That design makes the vascular finding plausible. Cerebral microbleeds and basal ganglia enlarged perivascular spaces are not social-reasoning modules. They are vascular injury markers that can disrupt distributed cognitive control systems. A task that requires perspective shifting and inhibition would be expected to suffer when those systems are compromised.
The Result Calibrates Theory of Mind After Aphasia
Older lesion work often emphasized right-hemisphere involvement in Theory of Mind, while aphasia studies sometimes suggested that nonverbal belief reasoning could be preserved despite severe language impairment.2,3 Kurtz et al. add a more granular middle position: some people with aphasia perform poorly, but the poor performance may reflect vascular burden and executive support systems as much as a primary loss of belief reasoning.
Rehabilitation implication: the wrong interpretation leads to the wrong target. If poor performance is read as a language artifact, social cognition may be ignored. If it is read as pure Theory of Mind impairment, vascular cognitive burden may be missed.
Preprint Status Should Lower Certainty, Not Interest
The medRxiv label matters. The paper has not been certified by peer review, and the MRI subset was smaller than the behavioral sample. Results should be treated as hypothesis-strengthening rather than practice-changing.
Still, the signal is coherent. Aphasia severity failed to explain task accuracy, while microbleed count survived false-discovery-rate correction across both tasks. That pattern is specific enough to justify replication rather than dismissal.
A stronger next study would add lesion-network mapping, direct executive-function tasks, depression and fatigue measures, hearing and vision checks, and real-world social participation outcomes. That would show whether false-belief task accuracy predicts daily communication problems or only laboratory task performance.
What Clinicians Should Not Infer From One Low Score
A low nonverbal false-belief score should not automatically be labeled as impaired empathy, impaired social motivation, or inability to understand other people. The task is cognitively dense even when language demand is reduced. A participant must watch the scene, remember object movement, track another person’s belief, inhibit competing knowledge in Reality-Known trials, and select the correct response.
Testing implication: social-cognition assessment after stroke should pair task scores with aphasia profile, executive-function testing, lesion data, vascular markers, mood, fatigue, and real-world communication reports. A single task cannot tell which component failed.
Research implication: the most interesting finding is the dissociation between aphasia severity and task accuracy. If replicated, it means social-cognitive rehabilitation for aphasia should not be reserved only for people with severe language impairment. Some people with milder aphasia may still struggle with perspective-taking tasks because broader vascular injury affects the support systems needed to perform them.
That also changes how family complaints should be interpreted. If relatives report that a person with aphasia seems less able to follow conversational intent, sarcasm, misunderstanding, or another person’s perspective, the problem may sit across language, executive control, and vascular cognitive injury. A narrow fluency score will not capture that full burden.
What This Preprint Can and Cannot Support
Supported: in this 44-person aphasia sample, nonverbal false-belief task performance was variable, aphasia severity did not explain accuracy, and higher cerebral microbleed count was associated with lower accuracy on both tasks.
Not supported: a clinical rule that microbleeds cause Theory of Mind impairment or that false-belief tasks should diagnose social-cognitive disorder in aphasia. The study was cross-sectional, preprint-stage, and partially limited by missing MRI marker data.
Best next test: larger longitudinal aphasia cohorts should combine nonverbal social-cognition tasks, executive-function measures, lesion mapping, CSVD markers, and real-world communication outcomes.
Clinically, the important question is whether a low false-belief score predicts conversation repair, misunderstanding, caregiver conflict, or social withdrawal after stroke. A laboratory task becomes useful only when it helps explain daily communication beyond language severity alone.
Microbleed burden also points to whole-brain vulnerability. Social-cognition rehabilitation may need to account for vascular cognitive impairment, attention, and inhibition rather than treating aphasia as the only barrier.
That broader assessment can prevent mislabeling a vascular-executive problem as poor effort.
Questions About Aphasia and Theory of Mind
Does aphasia itself damage Theory of Mind?
Sometimes task performance is reduced, but this preprint argues against a one-factor explanation. Aphasia severity was not the predictor; vascular burden was more informative.
Why use nonverbal tasks?
Nonverbal tasks reduce language demands so researchers can test belief reasoning, inhibition, and perspective-taking without requiring complex spoken responses.
Should this change clinical care now?
No. The evidence is not ready for clinical decision-making. It does support adding social cognition and vascular brain health to the research agenda for aphasia recovery.
References
- Kurtz J, Billot A, Falconer I, Small H, Charidimou A, Kiran S, Varkanitsa M. Mental-state reasoning or downstream vascular burden? Theory of Mind task performance in post-stroke aphasia. medRxiv. 2026. doi:10.64898/2026.04.14.26350532
- Apperly IA, Samson D, Chiavarino C, Humphreys GW. Frontal and temporo-parietal lobe contributions to Theory of Mind. PubMed
- Siegal M, Varley R. Neural systems involved in Theory of Mind. PubMed
- Charidimou A, et al. Cerebral small vessel disease and microbleeds in cognitive impairment. PubMed