A 2026 medRxiv preprint using parent-cocreated sensory-related outcome measures found that 83% of children and teens improved on at least 1 PROMIS domain during 6 months of bumetanide treatment.1 The result is interesting, but the unmasked single-case design means the strongest claim is about sensitive outcome tracking, not definitive bumetanide efficacy.
Research Highlights
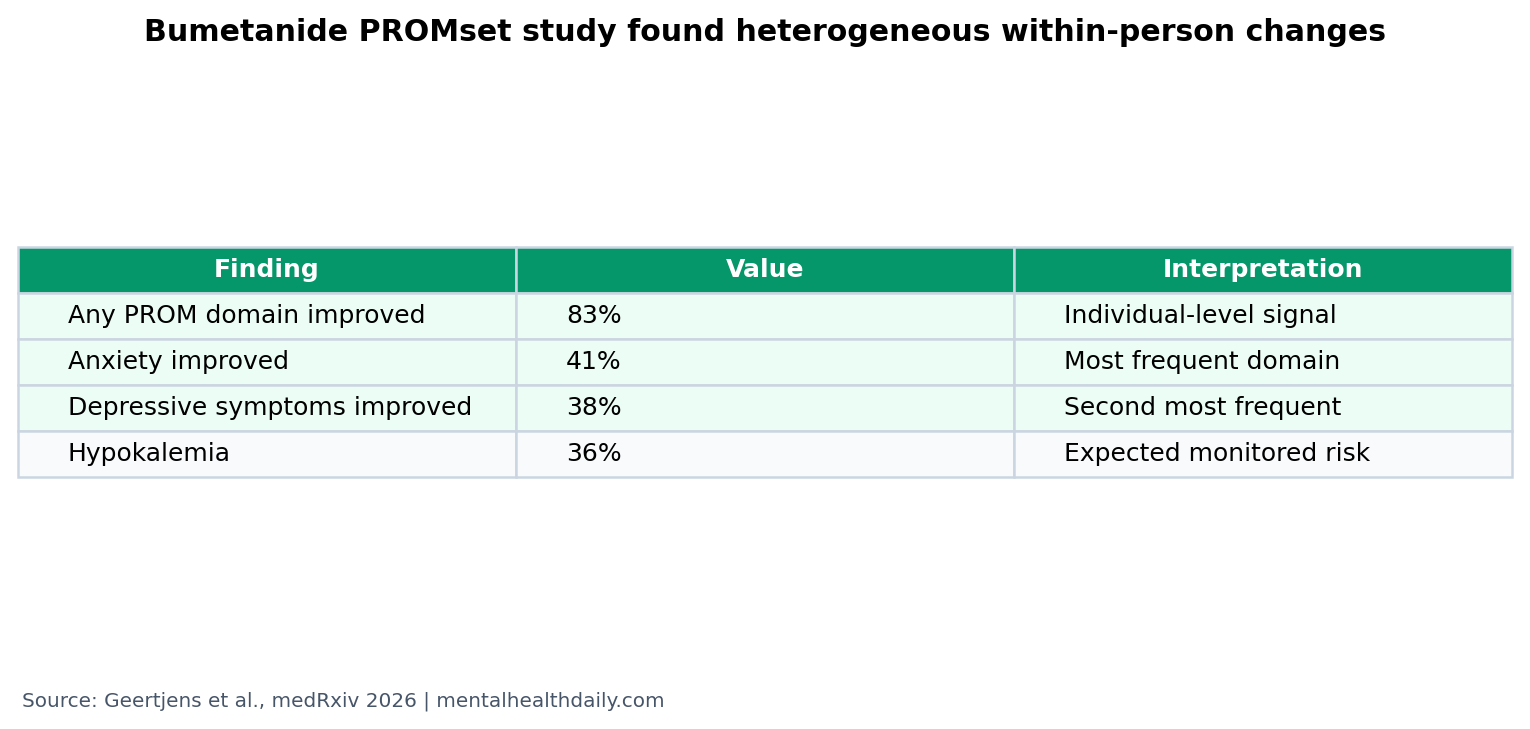
- Most participants had some improvement: among 95 analyzable PROMsets, 83% improved on at least 1 parent-reported domain during bumetanide treatment.1
- Anxiety and mood moved most often: individual-level improvement appeared in anxiety for 41% and depressive symptoms for 38% of participants.1
- Response was heterogeneous: 57% improved on 2 domains and 36% improved on 3 domains, supporting a multi-domain outcome approach.1
- Secondary scales improved too: group-level analyses improved across all conventional secondary outcomes, with historic-placebo superiority for RBS-R and SSP.1
- Safety monitoring remained necessary: expected adverse events included orthostatic complaints (37%), hypokalemia (36%), and increased diuresis (35%).1
Bumetanide is a loop diuretic being repurposed in some neurodevelopmental-disorder research because it blocks NKCC1, a chloride importer. The proposed brain mechanism is that changing neuronal chloride balance may shift GABA signaling, though peripheral diuretic effects remain clinically important.
Sensory reactivity means unusually strong, weak, or disruptive responses to sensory input such as sound, touch, light, texture, or movement. In autism and related neurodevelopmental conditions, sensory reactivity can affect anxiety, sleep, fatigue, social participation, routines, and daily functioning.
83% Improved on at Least 1 Parent-Reported Domain
Geertjens et al. enrolled children and adolescents aged 7 to 19 with atypical sensory reactivity and diagnoses including autism spectrum disorder, ADHD, epilepsy, or tuberous sclerosis complex. Of 113 participants who began intervention, 102 completed the trial and 95 had analyzable PROMsets.1
The primary outcome was a parent-proxy PROMset built from 7 PROMIS domains: anxiety, depressive symptoms, sleep disturbance, fatigue, sleep-related impairment, cognitive function, and peer relationships. During 6 months of bumetanide treatment, 83% improved on at least 1 PROM domain.1
PROMIS means Patient-Reported Outcomes Measurement Information System. In this study, PROMIS item banks measured how symptoms and functioning changed over time from the family perspective.
Anxiety and Depressive Symptoms Were the Most Frequent Individual Gains
Individual-level improvement appeared in 24% to 41% of participants depending on the PROM domain. Anxiety improved in 41%, and depressive symptoms improved in 38%.1
Among participants who improved, effect sizes were often large, with Cohen’s d exceeding 1 in 34% to 56% of individuals across domains.1 That is the argument for repeated individualized measurement: a group average can miss large changes in a subset if different people improve in different domains.
Clinical implication: the study is less about one universal autism symptom score and more about mapping which daily-life domains change for which child.
The Design Was Built to Avoid Signal Loss, Not to Prove Efficacy
Single-case experimental design means participants are measured repeatedly across baseline and intervention phases so each person becomes their own time-series analysis. This study randomized baseline durations from 2 to 12 weeks, then treated participants with bumetanide for 6 months.1
That design can detect individualized change, but it is not the same as a blinded placebo-controlled randomized trial. Participants and families knew treatment was happening, and the study began partly as a post-trial access pathway before expanding to treatment-naive participants.
Evidence-strength note: this was an unmasked preprint without concurrent placebo control. It can show that PROMsets detect changes during treatment; it cannot by itself prove those changes were caused by bumetanide rather than time, expectation, measurement effects, regression, family adaptation, or nonspecific care.
Phase III Autism Trials Still Limit the Drug Claim
Bumetanide has a long and contested autism-treatment history. Early trials suggested possible benefits, but Fuentes et al. reported 2 randomized phase III studies that did not establish on-label efficacy for children and adolescents with autism spectrum disorder.2
Geertjens et al. do not erase that failure. They shift the question from “does bumetanide improve a conventional group-level autism endpoint?” to “can better sensory-related PROMs and repeated within-person designs detect meaningful response patterns in heterogeneous neurodevelopmental cohorts?”1
That is a narrower and more defensible contribution. It may help future trials choose better endpoints, enrich likely responders, and separate true treatment effects from placebo and expectancy effects.
Adverse Events Were Expected but Not Trivial
Bumetanide is a diuretic, so safety monitoring is part of the intervention. Common expected adverse events included orthostatic complaints (37%), hypokalemia (36%), increased diuresis (35%), headache (20%), and dehydration (15%).1
Hypokalemia means low blood potassium. It can matter medically because potassium helps regulate muscle and heart electrical activity. The study used potassium supplementation and laboratory monitoring, which is exactly why unsupervised use is the wrong inference.
One serious adverse event, a hip fracture after a sports incident, was considered probably unrelated. Most expected adverse events were mild to moderate and resolved, but the monitoring burden is part of the real-world treatment equation.1
Outcome Design May Be the Larger Finding
Ben-Ari’s NKCC1/GABA rationale explains why bumetanide attracted neurodevelopmental interest.3 The BUDDI protocol laid out the single-case design logic for bumetanide across neurodevelopmental disorders.4 This 2026 preprint gives that approach a larger proof-of-concept dataset.
The most useful next trial would combine the strengths of both worlds: individualized PROMsets and repeated measurement, plus concurrent placebo control, blinding, biomarker or responder stratification, and prespecified criteria for clinically meaningful change.
Supported: sensory-related PROMsets captured within-person changes during bumetanide treatment in a heterogeneous neurodevelopmental cohort.
Not supported: treating bumetanide as proven effective for autism, ADHD, epilepsy, or tuberous sclerosis complex on the basis of this preprint alone.
Parent-Reported Outcomes Need Placebo Protection
The parent-cocreated outcome approach is a strength because it asks about domains families actually notice. It is also exactly why placebo protection matters. Parent reports can be sensitive to real change, but they can also be influenced by hope, treatment access, extra monitoring, clinician contact, and the relief of having a plan.
Useful sensitivity: weekly PROMIS item banks can catch changes in sleep, fatigue, anxiety, mood, peer functioning, and cognition that a broad autism severity scale might miss.
Needed specificity: the same sensitivity can detect nonspecific improvement. Without a blinded placebo arm, it is difficult to know how much of the observed change belongs to bumetanide itself.
Better responder criteria: future trials should define how many domains must improve, how large the T-score change must be, how long improvement must persist, and whether the change tracks objective markers such as EEG, chloride-related biology, sleep, or sensory-task performance.
The 2026 study points toward a more realistic neurodevelopmental trial model. Heterogeneous children may not improve on the same endpoint. A child whose main sensory-related burden is anxiety may not show the same response pattern as a child whose main burden is sleep-related impairment or peer withdrawal.
That logic supports personalized endpoints, but it also raises the statistical bar. If each participant can improve in a different domain, the analysis needs prespecified rules that prevent the trial from counting any favorable movement as treatment response. Otherwise, flexible outcomes become an easy way to overread noise.
The safety profile also pushes against casual interpretation. A treatment that requires potassium supplementation, laboratory checks, dose adjustment, and monitoring for dehydration is more than a behavioral-support adjunct. Any future efficacy signal has to be large enough, specific enough, and predictable enough to justify that burden in children and adolescents.
For families, the most honest takeaway is cautious. The study supports measuring sensory-related daily-life outcomes more carefully. It does not support starting bumetanide outside supervised medical research or specialist care.
That caution cuts both ways. A negative conventional trial does not prove every child is a nonresponder, and a positive single-case PROMset pattern does not prove the drug caused the response. The next generation of trials has to preserve individualized measurement while adding the controls needed to tell drug signal from expectation and time.
Responder definition is the hard part. A useful autism trial would need to decide in advance whether success means sensory tolerance, anxiety reduction, communication improvement, family burden change, or a broader individualized target. Otherwise, flexible outcomes can become hard to interpret even when families report real improvement.
The safest next design would keep parent-prioritized targets visible while masking treatment assignment and collecting adverse events in the same repeated format. That would protect both signal sensitivity and causal interpretation.
Questions About Bumetanide and Sensory Reactivity
Does this study prove bumetanide works for autism?
No. It was unmasked and lacked concurrent placebo control. It suggests a way to detect individualized change, but it does not overrule negative phase III autism trials.
Why use parent-cocreated PROMsets?
Families often notice changes in sleep, anxiety, fatigue, routines, and sensory tolerance that conventional diagnostic scales may not capture well.
Why did the study include ADHD, epilepsy, and TSC too?
The target was atypical sensory reactivity across neurodevelopmental disorders, not autism alone. That makes the sample more heterogeneous and the efficacy claim less diagnosis-specific.
Is bumetanide safe to try without monitoring?
No. The study included potassium supplementation, physical checks, and laboratory monitoring because diuresis, dehydration, and low potassium are expected risks.
References
- Geertjens LMG, Cristian G, Ramautar JR, et al. Assessing Parent-cocreated Sensory Reactivity Outcomes in Children with Neurodevelopmental Disorders Undergoing Bumetanide Treatment: A Multiple-Baseline Single-Case Experimental Design. medRxiv. 2026. doi:10.64898/2026.04.22.26351464
- Fuentes J, Parellada M, Georgoula C, et al. Bumetanide oral solution for the treatment of children and adolescents with autism spectrum disorder: results from two randomized phase III studies. Autism Research. 2023. doi:10.1002/aur.3005
- Ben-Ari Y. NKCC1 chloride importer antagonists attenuate many neurological and psychiatric disorders. Trends in Neurosciences. 2017;40:536-554. doi:10.1016/j.tins.2017.07.001
- Geertjens L, Cristian G, Haspels E, et al. Single-case experimental designs for bumetanide across neurodevelopmental disorders: BUDDI protocol. BMC Psychiatry. 2022;22:452. doi:10.1186/s12888-022-04033-8