
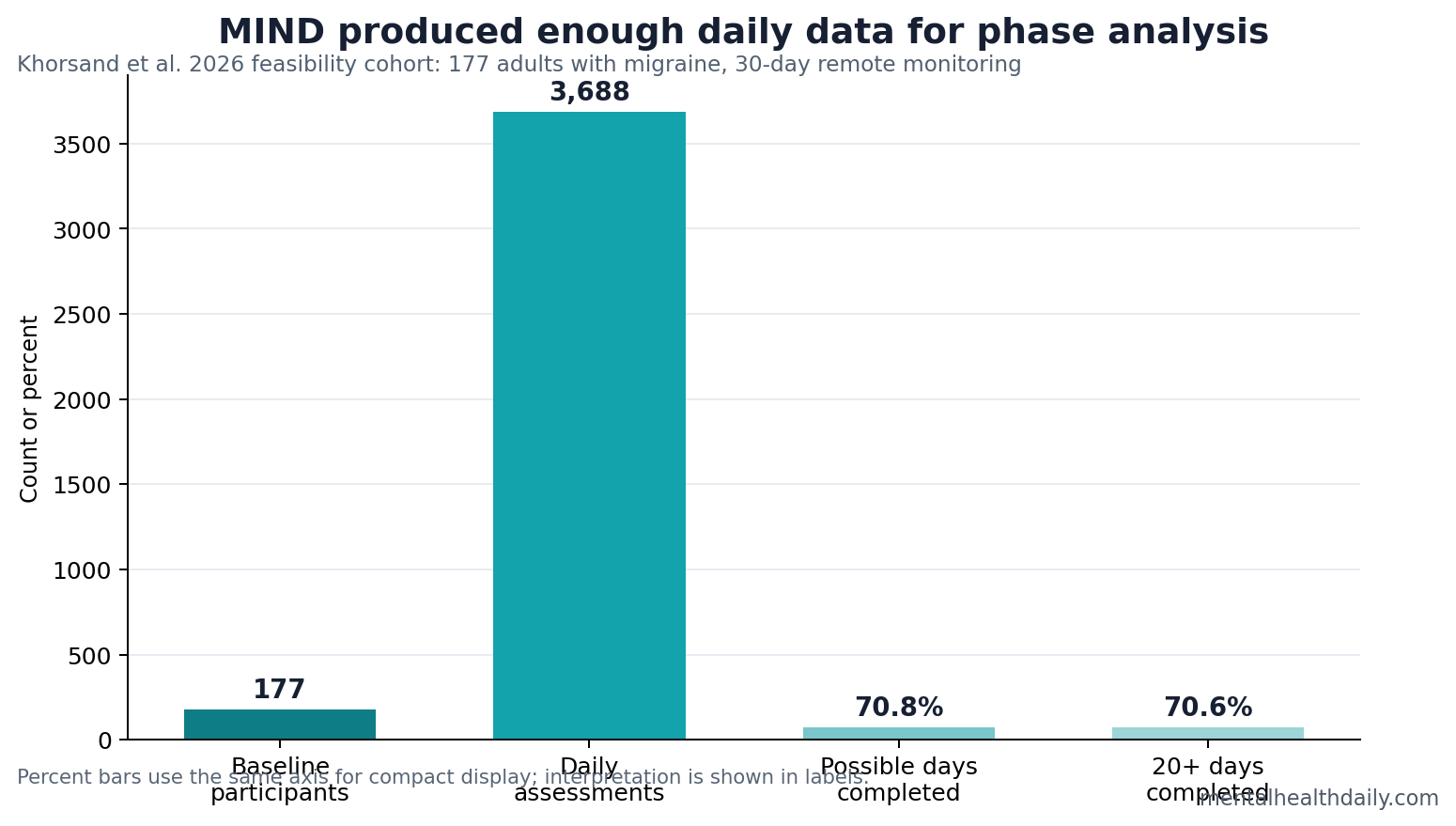
The MIND migraine feasibility study showed that remote migraine-cognition monitoring can produce a large daily dataset: 177 baseline participants completed 3,688 smartphone assessments, covering 70.8% of possible study days.1 The finding supports digital migraine endpoint infrastructure while leaving treatment effects and diagnostic thresholds untested.
Research Highlights
- Daily monitoring was feasible: Participants completed 3,688 daily smartphone assessments, equal to 70.8% of possible study days.1
- Most participants gave enough data: 70.6% completed at least 20 monitoring days, a practical threshold for within-person migraine phase analysis.1
- The cohort included heavy disease burden: Chronic migraine represented 80 of 177 participants, or 45.2% of the baseline sample.1
- Disability scaled with migraine frequency: Mean MIDAS was 98.57 in chronic migraine vs. 38.71 in low-frequency episodic migraine.1
- Timing still mattered: 24.0% of completed surveys were finished within 1 hour of availability, and 36.2% within 2 hours.1
Digital phenotyping means measuring symptoms, behavior, or cognitive performance repeatedly through phones or wearable devices. In migraine, that approach fits the disease because attacks fluctuate from day to day and because many disabling symptoms happen outside clinic visits.
Khorsand et al. used the MIND study to test whether a decentralized 30-day protocol could collect daily migraine reports and cognitive tasks with enough adherence to support later analyses. The study’s practical question was not whether a treatment worked. It was whether the measurement system was usable.
177 Migraine Participants Entered the Baseline Cohort
The baseline cohort included 177 participants with migraine, mean age 38.8 years, and 141 of 177 participants were female. Migraine frequency was deliberately broad: 59 participants had low-frequency episodic migraine, 38 had high-frequency episodic migraine, and 80 had chronic migraine.1
Chronic migraine generally means headache on at least 15 days per month, with migraine features on a substantial share of those days. Including that group matters because cognitive disruption and disability may look different in people with frequent headache than in people with occasional attacks.
The Migraine Disability Assessment score, or MIDAS, measures days of lost or reduced function because of headache. Mean MIDAS was 38.71 in low-frequency episodic migraine, 70.28 in high-frequency episodic migraine, and 98.57 in chronic migraine. The cohort therefore included people whose disease burden was high enough to justify repeated functional tracking.
3,688 Daily Assessments Made Within-Person Analysis Possible
The most important number in the feasibility paper is not a p-value. It is the completion volume. Participants completed 3,688 daily assessments, 70.8% of all possible study days, and 70.6% completed at least 20 monitoring days.1
For migraine cognition research, that matters because the scientific unit is often the person-day. A clinic visit can ask whether a person with migraine differs from a control. Daily monitoring can ask whether the same person performs differently on headache days, premonitory days, postdrome days, and non-headache days.
Completion Timing Was Useful, But Not Perfect
Daily symptom capture is most informative when it happens close to the target window. In MIND, 886 completed surveys, or 24.0%, were finished within the first hour after assessment availability. A total of 1,334, or 36.2%, were completed within 2 hours.1
Measurement lag is the delay between when a symptom or task should be recorded and when it is actually recorded. In migraine, lag can blur phase boundaries because headache onset, medication use, sleep, nausea, and cognitive symptoms can change across a few hours.
The timing data do not invalidate the protocol. They define the tradeoff: remote studies can collect far more real-world observations than clinic studies, but the analysis has to account for late entries, missed days, and participant burden.
The Companion Cognition Paper Shows Why Feasibility Matters
A companion MIND analysis used the daily design to compare ictal headache days with nonictal days. It found that brain fog was more likely during headache days, OR 3.39, and that some objective smartphone tasks slowed or lost accuracy during attacks.2
That downstream result depends on the feasibility result. Without enough repeated assessments, migraine phase analysis becomes too sparse to separate attack-related cognitive change from stable between-person differences.
Prior migraine cognition reviews have argued that cognitive symptoms are part of migraine burden, but older clinic designs often struggled to capture timing.3 Electronic migraine diary methods made the timing problem more tractable by collecting data in daily life rather than asking patients to reconstruct the full attack cycle weeks later.4
Feasibility Evidence Is Not Clinical Validation
Supported: a 30-day remote protocol collected enough daily data to support migraine phase and cognition analyses in a self-selected cohort with substantial disease burden.
Not supported: a claim that smartphone cognition scores diagnose migraine, replace neuropsychological testing, or prove treatment response. Feasibility data answer whether a measurement system can run; they do not answer whether the endpoint is clinically validated.
Best use: MIND-style monitoring is strongest as a research endpoint and symptom-burden tool. It can show whether cognition changes around attacks and whether future treatments reduce the cognitive burden that pain scores miss.
Adherence Data Define Whether Digital Endpoints Are Trustworthy
A digital endpoint is only as strong as its missing-data pattern. If people complete surveys mostly on easier days, the dataset can undercount severe attacks. If they complete surveys mostly during severe attacks, it can overrepresent disability. MIND’s 70.8% daily completion rate is therefore more than a convenience number; it is part of the endpoint’s credibility.
Missingness pattern: remote migraine studies need to know which days disappear. Missed entries after severe headache, medication sedation, sleep disruption, nausea, or work conflict could bias phase comparisons. A 30-day protocol with at least 20 completed days for 70.6% of participants gives researchers enough repeated observations to model those risks rather than guessing from a clinic visit.
Timing pattern: the 24.0% first-hour and 36.2% first-2-hour completion figures show both feasibility and friction. The study collected enough data for analysis, but a large share of entries still arrived after the earliest window. Future protocols may need shorter tasks, more flexible prompts, or passive timing anchors to reduce lag.
Baseline Disability Makes the Cohort More Than a Convenience Sample
The cohort was not a trivial wellness-app sample. Chronic migraine accounted for 45.2% of baseline participants, and mean MIDAS rose from 38.71 in low-frequency episodic migraine to 98.57 in chronic migraine.1 That gradient means the study captured people whose migraine burden was high enough for cognitive and functional endpoints to be clinically relevant.
High disability also changes the interpretation of adherence. Completing smartphone tasks while dealing with frequent migraine is harder than completing them in a low-burden population. For that reason, the adherence rates are a real feasibility signal for the population most likely to need better functional measurement.
The next step is validation against external anchors: missed work days, medication use, sleep disruption, neuropsychological tasks, and patient-rated cognitive interference. A digital migraine endpoint becomes clinically stronger when it predicts something outside the phone screen.
That validation should also test burden. A task battery that is scientifically elegant but too annoying during migraine will fail in the real world. The best digital endpoint is short enough to complete during symptoms, sensitive enough to detect attack-linked change, and stable enough that treatment trials can interpret movement over time.
MIND’s value is that it supplies a platform for those next tests. The feasibility paper does not settle which cognitive task should win. It shows that enough daily migraine data can be collected to compare tasks, phases, adherence patterns, and patient-reported function inside the same monitoring frame.
That makes feasibility an early gate, not an endpoint. The measurement system first has to run reliably; only then can researchers ask whether the numbers change care.
For MIND, the next credibility test is whether daily cognition scores explain disability that headache counts alone miss.
That test should also account for medication timing, sleep, aura, nausea, photophobia, and work demands. A smartphone cognition score is more useful when it distinguishes migraine-related cognitive disruption from ordinary fatigue or poor testing conditions.
Participant burden remains the practical limiter. A digital endpoint that is too long, too frequent, or poorly timed can create missing data exactly when migraine symptoms are most severe.
Patient feedback should therefore shape prompt timing and task length before a digital endpoint moves into trials.
Questions About MIND and Migraine Digital Testing
What did the MIND feasibility paper prove?
It proved that a remote 30-day migraine diary plus smartphone cognition protocol could collect thousands of daily assessments with usable adherence.
Did the study test a migraine treatment?
No. It was a feasibility and baseline cohort paper, not a randomized treatment trial.
Why does daily testing matter for migraine?
Migraine symptoms vary by phase. Daily testing lets researchers compare headache days and non-headache days within the same person instead of relying only on clinic snapshots.
Could this become a clinical tool?
Possibly, but not from feasibility data alone. Clinical use would require validated thresholds, reliability testing, and evidence that the measurements improve care decisions.
References
- Khorsand B, et al. The MIND study: design, feasibility, and baseline characteristics. medRxiv. 2026. doi:10.64898/2026.04.14.26350866
- Khorsand B, et al. Digital assessment of objective and patient-reported cognitive function in migraine. medRxiv. 2026. doi:10.64898/2026.04.14.26350892
- Vuralli D, Ayata C, Bolay H. Cognitive dysfunction and migraine. Journal of Headache and Pain. 2018. doi:10.1186/s10194-018-0933-4
- Lipton RB, et al. Migraine tracking and real-world symptom capture using electronic diary methods. Headache. 2018. doi:10.1111/head.13365