A 2026 study by Bai et al. in Dialogues in Clinical Neuroscience uses Mendelian randomization (MR) — inherited genetic variants as a natural experiment to test causality — and concludes that migraines causally lower cognitive performance in a Han Chinese sample.1 The headline conclusion is plausible; the effect-size numbers in the popular MR shorthand (odds ratios in the dozens, sometimes hundreds) are not.
Research Highlights
- PRS linked migraine genetics to lower MMSE: higher migraine genetic load predicted a 2.31-point lower Mini-Mental State Examination score (95% CI −4.56 to −0.06; p = 0.044), with an instrument just above the weak-instrument cutoff (F = 13.2).1
- 18 SNP instruments drove the design: Bai 2026 ran one- and two-sample MR on the Taiwan Biobank, a Han Chinese cohort, using migraine-associated single-nucleotide polymorphisms as genetic instruments.1
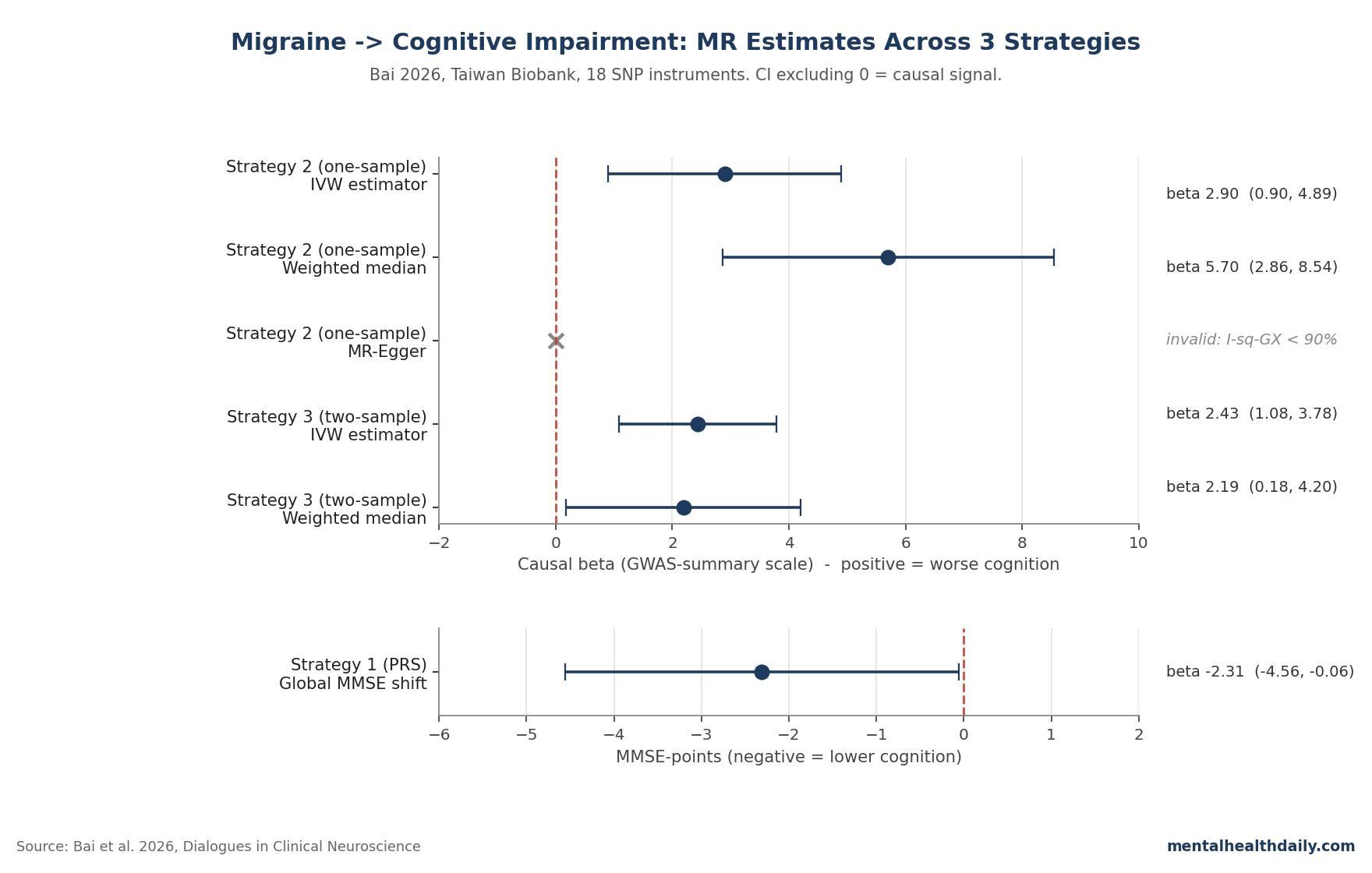
- One-sample MR (Strategy 2): IVW estimator β = 2.90 (95% CI 0.90 to 4.89). The MR-Egger estimator was unusable because I²GX fell below 90%, the standard validity threshold.1,4
- Two-sample MR (Strategy 3): IVW β = 2.43 (95% CI 1.08 to 3.78); weighted median β = 2.19 (95% CI 0.18 to 4.20). Both confidence intervals exclude zero but are very wide.1
- The odds ratios in the abstract (OR up to 18.17 in IVW; up to 298.86 in weighted median) are technically derived but reflect tiny absolute baseline rates; the wide 95% CIs (e.g., 17.46 to 5,115.34) make them unusable as point estimates. The MMSE-shift number is the more interpretable read.1
The migraine–cognition story has been muddied for a decade by registry studies that disagree with each other — some show migraineurs at higher dementia risk, some show no link, and a handful even point the other way.2,3 Bai 2026 brings a new lever to that argument, but the assumptions matter more than the headline.
The validity diagnostic (MR-Egger’s I²GX) failed badly enough that the Egger estimator was discarded. That doesn’t make the causal claim wrong — the IVW (inverse-variance weighted) and weighted-median estimators broadly agree — but it does mean the precise magnitude is uncertain.1,4
Bai 2026: Three MR Strategies on the Taiwan Biobank
The Taiwan Biobank (TWB) has genotyped over 27,000 Han Chinese adults using custom TWB arrays. Migraine diagnoses came from structured questionnaire applying the International Classification of Headache Disorders (ICHD) 2nd edition; cognition was the traditional Chinese MMSE (mean 27.7 ± 2.4).1
Three causal-inference strategies ran in parallel:
- Strategy 1 — PRS as a single instrumental variable. Of 99 migraine-associated SNPs identified at p < 5×10−8, only 18 were available in TWB after linkage-disequilibrium clumping. These were combined into a polygenic risk score and analyzed via two-stage least squares. F-statistic = 13.2 — just above the conventional weak-instrument cutoff of 10.1
- Strategy 2 — one-sample MR with summary GWAS data. SNP-migraine associations were taken from the published European GWASs (Gormley 2016 and others); SNP-cognition associations were derived from the same TWB participants. IVW, MR-Egger, and weighted-median estimators were applied.1,7
- Strategy 3 — two-sample MR with non-overlapping populations. SNP-migraine associations from the IEU OpenGWAS database (European-ancestry samples); SNP-cognition associations from TWB. This is the most defensible by MR convention because it minimizes weak-instrument bias.1,8
What β = 2.43 Means — and Why the Abstract’s ORs Inflate
The two-sample MR result — IVW β = 2.43 (95% CI 1.08 to 3.78) — is the headline number. Translated: each unit increase in the genetically-predicted log-odds of migraine is associated with a substantial shift on the MMSE score axis.
The exact units are awkward because MR estimators on summary GWAS data return scaled coefficients, not direct point-shift predictions. The PRS analysis (Strategy 1) is more interpretable: 2.31 MMSE points lower across the upper PRS tertile, with a confidence interval that barely clears zero (95% CI −4.56 to −0.06).1
The abstract’s odds ratios are a different beast. OR = 18.17 (95% CI 2.46 to 132.95) for one-sample IVW; OR = 298.86 (95% CI 17.46 to 5,115.34) for the weighted median estimator.
Those numbers are mathematically valid given the β coefficients, but the confidence intervals span two orders of magnitude. They reflect the very low baseline prevalence of MMSE-defined cognitive impairment in the analytic subsample, not a real-world claim that migraine multiplies dementia risk by 300x.
The defensible summary stat is the MMSE-point shift, not the OR.
MR-Egger Failed Validity — What That Tells Us About Pleiotropy
Mendelian randomization rests on three assumptions about the genetic instruments: relevance (SNPs predict migraine), independence (SNPs are not confounded with anything that independently affects cognition), and the exclusion restriction (SNPs only affect cognition through migraine).8
The third assumption — no horizontal pleiotropy, where an instrument SNP affects the outcome through a different pathway — is the weak link in essentially every MR study. Migraine is a tough case because migraine GWASes consistently flag SNPs in vascular and neuronal-regulation pathways that can affect cognition independently.7,9
MR-Egger regression is the standard sensitivity check. It can produce unbiased estimates even when most instruments are pleiotropic — provided its I²GX diagnostic clears about 90% (one-sample) or 91% (two-sample) per Minelli 2021’s simulation work on biobank-scale data.10
In Bai’s analysis, I²GX fell well below 90%, and the MR-Egger estimator was discarded. The authors lean on the weighted median estimator instead, which gives unbiased estimates as long as fewer than 50% of the SNPs are invalid — a weaker assumption than IVW’s “all instruments valid” demand, but still an assumption.4
Pleiotropic loci: 3 migraine-without-aura SNPs (mapping to TRPM8, PHACTR1, and MMP16) showed clear horizontal pleiotropy. PHACTR1 is a coronary artery disease and cervical artery dissection risk locus — vascular pathways that can affect cognition independently.11
Bai interpreted this as genetic overlap with cardiovascular and psychiatric disease, but it limits how confidently one MR can claim causality.
Where Bai 2026 Sits in the Broader Migraine–Cognition Literature
The non-MR literature is mixed. A 2022 meta-analysis by Gu et al. found migraineurs had significant cognitive deficits, especially in language, plus elevated all-cause dementia risk.5 Islamoska et al. followed 1.6 million Danish adults and linked mid- to late-life migraine diagnosis to subsequent dementia diagnosis (HR around 1.5).6
Cutting against those: the 2005 Gaist Danish twin study found no long-term cognitive effect of migraine,12 the Jelicic Maastricht Aging Study found no cognitive impact in older migraineurs,13 and a 2012 analysis of the Women’s Health Study by Rist et al. found no faster cognitive decline in migraineurs over 9 years — a notable null in a well-powered cohort.14
Bai is the first MR study to use MMSE cognition as the outcome in a Han Chinese population. Across the full literature, some causal contribution of migraine to cognitive decline is plausible and now triangulated by both observational and MR evidence.
Whether the magnitude is small (consistent with the null cohort studies) or larger (consistent with registry data) remains unsettled. The popular framing — “migraine causes cognitive impairment, MR proves it” — is too strong. A calibrated read is narrower: migraine probably contributes modestly to cognitive decline, and 1 MR now points in the same direction as the registry signal.
Limitations of the Bai Analysis
Five caveats deserve weight:
- The Han Chinese sample limits generalizability. Most large migraine GWAS data — including the SNP-migraine associations Bai used as instruments — come from European-ancestry samples. Trans-ethnic SNP effect sizes can shift, and the authors themselves call for replication in South Asian, African, Hispanic, and Oceanic populations.1,15
- Cognitive assessment is MMSE-only. The traditional Chinese MMSE is validated in this population but is famously insensitive to mild executive dysfunction. The Montreal Cognitive Assessment (MoCA) and trail-making tests would have caught more variance in the upper-end cognitive range where most migraineurs sit.1
- The PRS instrument is borderline weak. F-statistic = 13.2 just clears the cutoff of 10, but biobank-scale MR typically wants F > 50. A weak instrument biases one-sample MR toward the confounded estimate — the wrong direction for a clean causal test.8
- MR-Egger was unusable, leaving weighted median as the sole pleiotropy-robust estimator. Weighted median assumes < 50% of instruments are invalid; if more are pleiotropic (which the PHACTR1, TRPM8, MMP16 results suggest), even weighted median can’t fully clean the estimate.4
- The strategy-2 odds ratios are wildly imprecise. OR of 298 with a 95% CI of 17 to 5,115 is technically positive, but the point estimate carries almost no information. The MMSE-shift coefficient is the only estimator with a meaningful effect-size interpretation.
Migraine Risk Supports Treatment, Not Dementia Panic
If you have migraine and are worried about long-term cognitive decline, the calibrated answer has three layers.
- The directional signal is consistent. Cohort studies (some of them), meta-analytic synthesis, and now MR all point the same way: migraine probably contributes modestly to cognitive decline risk.5,6
- The magnitude is genuinely uncertain. Effect-size estimates range from null (Rist 2012, Gaist 2005) to modest (Islamoska 2020 HR around 1.5) to the wide-CI MR estimates here. Anyone telling you migraine multiplies dementia risk by an order of magnitude is overstating the data.14,12
- Migraine prophylactic medications are not the bigger worry. Topiramate causes reversible psychomotor slowing; valproate and some antidepressants used in prophylaxis have similar profiles. The cognitive concern in migraine is the migraine itself, not standard prophylaxis — and untreated migraine has its own cognitive interictal cost. Treat the migraine.16
Cardiovascular fitness, sleep, hearing protection, depression treatment, and hypertension control remain the highest-yield cognitive-reserve levers. Migraine status modestly raises the stakes.
Reader Questions on the Migraine–Cognition MR Study
Does this study prove migraines cause cognitive decline?
It strengthens the causal case but doesn’t close it. Two of three MR strategies returned significant positive estimates pointing the same direction as the observational literature, but the MR-Egger pleiotropy check failed and the magnitudes have very wide confidence intervals. “Probably contributes modestly” is closer to what the data support than “causes.”1,5
What did MR add beyond older registry studies?
It uses a method (MR) that is harder to fool with confounding. Registry studies of migraineurs have a built-in problem: people with migraines differ from people without them on dozens of variables (sleep, stress, medication exposure, healthcare-seeking) that independently affect cognition. MR sidesteps most of that — though it introduces its own assumptions, which Bai’s analysis only partially satisfied.1,8
Does it apply to people who aren’t Han Chinese?
Not directly. The migraine SNPs were drawn from European-ancestry GWASes; the cognition data are from a Han Chinese biobank. The signal might generalize, or population-specific genetic architecture might shift the magnitude. The Bai authors explicitly call for replication in South Asian, African, Hispanic, and Oceanic populations.1,15
Should anyone change migraine treatment based on this study?
No. The study confirms a biological link the field had already inferred from observational data. It doesn’t recommend specific prophylactic strategies or change first-line treatment. If anything, it weakens the worry that migraine prophylaxis itself is the cognitive culprit — the migraine is.1,16
References
- Migraines and the association of cognitive impairment: a one- and two-sample mendelian randomization analysis. Bai C-H, Fan H-Y, Lin H-A, Lin S-F. Dialogues in Clinical Neuroscience. 2026;28(1):107–118. doi:10.1080/19585969.2026.2636459
- Migraine and risk of dementia: a nationwide retrospective cohort study. Chuang C-S, Lin C-L, Lin M-C, Sung F-C, Kao C-H. Neuroepidemiology. 2013;41(3-4):139–145. doi:10.1159/000353559
- Cognitive aging in migraine sufferers is associated with more subjective complaints but similar age-related decline: a 5-year longitudinal study. Martins IP, et al. Journal of Headache and Pain. 2020;21(1):31. doi:10.1186/s10194-020-01100-x
- Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Bowden J, Davey Smith G, Haycock PC, Burgess S. Genetic Epidemiology. 2016;40(4):304–314. doi:10.1002/gepi.21965
- Association between migraine and cognitive impairment. Gu L, Wang Y, Shu H. Journal of Headache and Pain. 2022;23(1):88. doi:10.1186/s10194-022-01462-4
- Mid- to late-life migraine diagnoses and risk of dementia: a national register-based follow-up study. Islamoska S, et al. Journal of Headache and Pain. 2020;21(1):98. doi:10.1186/s10194-020-01166-7
- Meta-analysis of 375,000 individuals identifies 38 susceptibility loci for migraine. Gormley P, et al. Nature Genetics. 2016;48(8):856–866. doi:10.1038/ng.3598
- Avoiding bias from weak instruments in Mendelian randomization studies. Burgess S, Thompson SG, CRP CHD Genetics Collaboration. International Journal of Epidemiology. 2011;40(3):755–764. doi:10.1093/ije/dyr036
- Shared genetic basis for migraine and ischemic stroke: a genome-wide analysis of common variants. Malik R, et al. Neurology. 2015;84(21):2132–2145. doi:10.1212/wnl.0000000000001606
- The use of two-sample methods for Mendelian randomization analyses on single large datasets. Minelli C, et al. International Journal of Epidemiology. 2021;50(5):1651–1659. doi:10.1093/ije/dyab084
- A genetic variant associated with five vascular diseases is a distal regulator of endothelin-1 gene expression. Gupta RM, et al. Cell. 2017;170(3):522–533.e15. doi:10.1016/j.cell.2017.06.049
- Long-term effects of migraine on cognitive function: a population-based study of Danish twins. Gaist D, et al. Neurology. 2005;64(4):600–607. doi:10.1212/01.wnl.0000151858.15482.66
- Does migraine headache affect cognitive function in the elderly? Report from the Maastricht Aging Study (MAAS). Jelicic M, van Boxtel MP, Houx PJ, Jolles J. Headache. 2000;40(9):715–719. doi:10.1046/j.1526-4610.2000.00124.x
- Migraine and cognitive decline among women: prospective cohort study. Rist PM, Kang JH, Buring JE, Glymour MM, Grodstein F, Kurth T. BMJ. 2012;345:e5027. doi:10.1136/bmj.e5027
- Transethnic genetic-correlation estimates from summary statistics. Brown BC, Ye CJ, Price AL, Zaitlen N. American Journal of Human Genetics. 2016;99(1):76–88. doi:10.1016/j.ajhg.2016.05.001
- Topiramate: effects on cognition in patients with epilepsy, migraine headache and obesity. Sommer BR, Mitchell EL, Wroolie TE. Therapeutic Advances in Neurological Disorders. 2013;6(4):211–227. doi:10.1177/1756285613481257