A 2026 systematic review of advanced neuroimaging in multiple sclerosis narrowed 600 database records to 12 studies and found the clearest cognition signal in basal ganglia iron-sensitive MRI measures, while thalamic susceptibility was more variable and often tangled with atrophy.
Research Highlights
- Basal ganglia signal was strongest: across 12 studies, elevated susceptibility or iron-related metrics in the putamen, caudate, or globus pallidus were repeatedly linked to impaired processing speed, executive control, or cognitive composite scores.
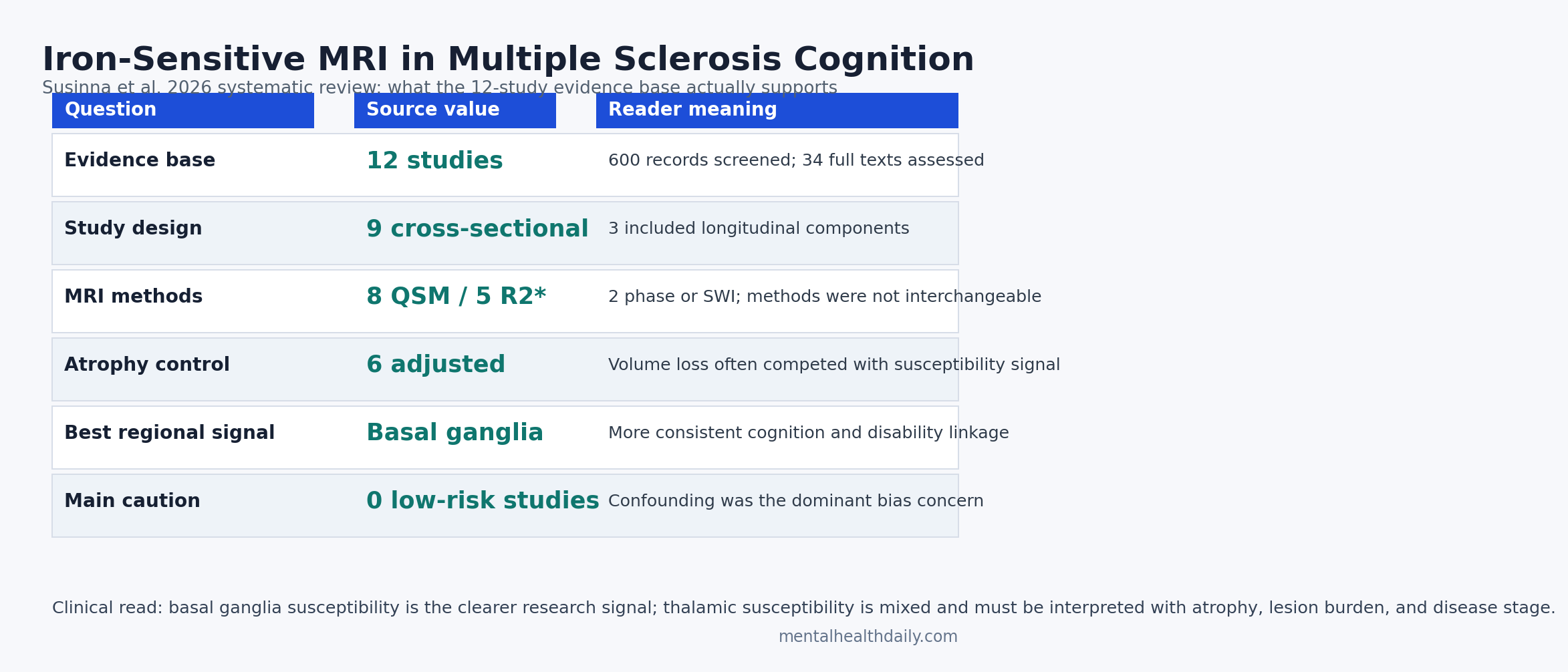
- Search yield was narrow: Susinna et al. screened 600 database records, assessed 34 full-text papers, and included 12 studies that directly connected iron-sensitive MRI metrics with cognition in multiple sclerosis.
- MRI methods varied: 8 studies used quantitative susceptibility mapping, 5 used R2* relaxometry, and 2 used phase or susceptibility-weighted imaging, making direct comparison difficult.
- Thalamic findings were mixed: thalamic susceptibility sometimes tracked disability, especially in progressive disease, but 6 studies had to account for atrophy or volume because tissue loss can dominate the cognitive signal.
- Clinical use is not ready: ROBINS-E ratings found 0 low-risk studies, with confounding rated as the main uncertainty across the observational literature.
Iron-sensitive MRI refers to magnetic resonance methods that pick up local magnetic-field effects produced partly by iron in brain tissue. In multiple sclerosis (MS), the practical question is not whether the brain contains iron; it is whether susceptibility-based scans add useful information about cognitive decline beyond lesions, brain-volume loss, and ordinary clinical disability scales.
Susinna et al. focused on deep gray matter structures because the basal ganglia and thalamus sit inside cortico-subcortical loops that support processing speed, attention, motor efficiency, and executive control. Those are also the cognitive domains MS patients often notice first: slower thinking, weaker multitasking, and more effortful mental switching.
12 Studies Survived Screening From 600 Database Records
The 2026 review followed PRISMA methods and searched PubMed, Scopus, Web of Science, and Embase in October 2025. The search produced 600 records. Deduplication reduced that to 397, title-and-abstract screening narrowed the set further, and 34 full-text papers were assessed for eligibility. The final evidence base was 12 studies.
Included cohorts: sample sizes ranged from 29 to 640 people with MS. Most cohorts included relapsing-remitting MS, with smaller or separate representation of secondary progressive MS, primary progressive MS, and clinically isolated syndrome. Healthy controls appeared in 7 of 12 studies.
Study design: 9 studies were cross-sectional, and 3 included a longitudinal component. That matters because a cross-sectional MRI-cognition association can show that 2 things travel together, but it cannot prove that iron-sensitive signal caused later cognitive decline.
Cognitive testing: processing speed was the anchor outcome, most often measured with the Symbol Digit Modalities Test (SDMT), a quick paper-or-screen task that asks patients to match symbols with numbers. Several studies also tested executive control, verbal learning, visuospatial memory, fatigue, dexterity, walking speed, and visual function.
Basal Ganglia Iron Metrics Tracked Processing Speed and Control
Basal ganglia are deep brain nuclei, including the caudate, putamen, and globus pallidus, that help coordinate movement, motivation, habit learning, response inhibition, and cognitive speed. In MS, these regions are relevant because slowing can be cognitive and motor at the same time.
Susinna et al. found the most reproducible cognitive pattern in basal ganglia susceptibility. Khalil et al. linked increased iron-related measures in the putamen and caudate with worse SDMT performance. Schmalbrock et al. reported that higher 7 T susceptibility in the caudate and anterior putamen correlated with poorer inhibitory control. Fujiwara et al. found that globus pallidus susceptibility related to a lower composite of memory and processing speed, independent of atrophy.
Voon et al. provided the largest adjacent signal. In 640 people with MS, higher deep gray matter quantitative susceptibility mapping values in basal ganglia regions correlated with higher lesion burden, higher disability, slower Nine-Hole Peg Test performance, and lower SDMT scores after adjustment for relevant covariates.
The result should be read as a regional pattern, not a single universal biomarker. Basal ganglia susceptibility seems to mark a disease-burden phenotype in which iron-sensitive signal, lesion load, disability, and slower cognition move in the same direction.
Thalamic Susceptibility Was Harder to Interpret Than Basal Ganglia Signal
Quantitative susceptibility mapping (QSM) estimates how strongly tissue distorts the magnetic field inside an MRI scanner. Iron can increase susceptibility, but QSM is not a pure iron meter. Myelin, calcium, veins, tissue loss, and processing choices can change the signal too.
Thalamic findings were less consistent than basal ganglia findings. Some cohorts found that thalamic volume, myelin-sensitive measures, or broader atrophy explained processing-speed impairment better than susceptibility. Pontillo et al. reported that R1 relaxometry and atrophy were more closely related to SDMT than magnetic susceptibility. Modica et al. found iron-cognition relationships in deep gray matter, but volume often explained more variance.
That does not make the thalamus irrelevant. Cagol et al. reported that thalamic quantitative MRI metrics predicted neurologic and cognitive disability even after accounting for lesion load and atrophy. Williams et al. found lower thalamic susceptibility in secondary progressive MS than in controls, with lower susceptibility related to worse physical, cognitive, and visual disability.
Interpretive key: basal ganglia susceptibility usually reads as a clearer iron-associated burden signal. Thalamic susceptibility is more stage-dependent because thalamic tissue can lose volume, change myelin content, and show different iron dynamics as MS progresses.
Rim Lesions Connect Iron Signal to Chronic Active Inflammation
Paramagnetic rim lesions are MS lesions with a dark rim on susceptibility-sensitive MRI, thought to reflect iron-laden microglia and macrophages at chronically active lesion edges. They are not the same measurement as deep gray matter susceptibility, but they sit in the same biological neighborhood: iron, chronic inflammation, and tissue injury.
Two included studies examined chronic active lesion markers. Dal-Bianco et al. used a 7 T framework and found that patients with iron rim lesions had smaller thalamic volume and slightly worse SDMT performance than patients without rim lesions, although mean neuropsychological z-scores and change over time did not differ significantly.
Marcille et al. studied 159 people with relapsing-remitting MS and found that having at least 1 QSM rim-positive lesion was associated with worse cognitive performance and more structural neurodegeneration as lesion burden increased.
Rim lesions support the biological plausibility of an iron-inflammation-cognition link. They do not prove that deep gray matter iron deposition alone drives cognitive decline. They suggest that susceptibility MRI can flag a more aggressive MS phenotype when chronic active lesions, subcortical volume loss, and cognitive slowing cluster together.
Atrophy Adjustment Separates Biomarker Signal From Brain-Volume Loss
Atrophy means loss of tissue volume. In MS cognition research, atrophy is a major confounder because smaller thalamic, hippocampal, cortical, or whole-brain volumes can explain slower processing speed even when susceptibility measures look abnormal.
Susinna et al. reported that only 6 studies explicitly accounted for volumetric measures or atrophy in statistical models. That is the core calibration point. A scan marker is more clinically interesting when it adds information after lesion load and volume loss are handled. If susceptibility disappears after atrophy adjustment, it may be a proxy for tissue loss rather than an independent cognition biomarker.
- More convincing pattern: susceptibility remains related to SDMT, inhibitory control, or memory after adjusting for regional volume, lesion burden, age, sex, and disease duration.
- Weaker pattern: susceptibility correlates with cognition before adjustment, but thalamic or whole-brain volume explains the result better.
- Clinical gap: cross-sectional associations need longitudinal proof that baseline susceptibility predicts future cognitive decline.
For now, iron-sensitive MRI looks most useful as part of a multimodal imaging profile: lesion burden, atrophy, myelin-sensitive metrics, rim lesions, and deep gray matter susceptibility interpreted together.
Risk of Bias Keeps Iron MRI Out of Routine Cognitive Triage
ROBINS-E assessment rated the included evidence from some concerns to very high risk of bias. No study was rated low risk overall. The main problem was confounding: disease duration, phenotype, treatment exposure, baseline disability, lesion load, and atrophy were not consistently handled across studies.
Method heterogeneity added another layer. Scanner strength ranged from 3 T to 7 T, QSM reconstruction and referencing pipelines differed, and non-QSM methods such as R2* and phase/SWI measure related but non-identical tissue properties. Even the same anatomical label can hide different segmentation choices or partial-volume effects.
Evidence-strength note: this is a cognition-relevant biomarker literature, not a clinical decision rule. The review supports basal ganglia susceptibility as a repeated research signal and thalamic susceptibility as a complicated stage-dependent marker. It does not support ordering iron-sensitive MRI to diagnose cognitive impairment in an individual MS patient.
Questions About Iron MRI and Multiple Sclerosis Cognition
Does iron-sensitive MRI show who has cognitive impairment in MS?
Not reliably enough for individual clinical use. The strongest evidence links basal ganglia susceptibility with processing speed and executive control across research cohorts, but the studies were heterogeneous and observational.
Why does the basal ganglia signal look clearer than the thalamus?
Basal ganglia susceptibility more often moved in the expected direction: higher iron-related signal with worse cognition or disability. Thalamic susceptibility can increase, decrease, or lose interpretability depending on disease stage, atrophy, myelin changes, and progressive MS biology.
Are paramagnetic rim lesions the same as deep gray matter iron?
No. Rim lesions are focal white matter lesions with iron-laden inflammatory cells at the lesion edge. Deep gray matter susceptibility measures subcortical structures such as the caudate, putamen, globus pallidus, and thalamus. Both can reflect iron-related MS pathology, but they are not interchangeable.
What would make iron MRI more clinically useful?
Longitudinal studies with standardized QSM pipelines, consistent cognitive batteries, atrophy adjustment, treatment data, and follow-up cognitive outcomes would matter most. A useful clinical marker has to predict future decline after current disease burden is measured.
References
- Susinna C, Restuccia G, Triolo G, Marafioti G, Cammaroto S, Sessa E, et al. Iron accumulation in multiple sclerosis and implications for cognitive and clinical progression: a systematic review of advanced neuroimaging studies. Journal of Neurology. 2026;273:275. doi:10.1007/s00415-026-13815-z
- De Lury AD, Bisulca JA, Lee JS, Altaf MD, Coyle PK, Duong TQ. Magnetic resonance imaging detection of deep gray matter iron deposition in multiple sclerosis: a systematic review. Journal of the Neurological Sciences. 2023;453:120816. doi:10.1016/j.jns.2023.120816
- Fujiwara E, Kmech JA, Cobzas D, Sun H, Seres P, Blevins G, et al. Cognitive implications of deep gray matter iron in multiple sclerosis. AJNR American Journal of Neuroradiology. 2017;38:942-948. doi:10.3174/ajnr.A5109
- Modica CM, Zivadinov R, Dwyer MG, Bergsland N, Weeks AR, Benedict RHB. Iron and volume in the deep gray matter: association with cognitive impairment in multiple sclerosis. AJNR American Journal of Neuroradiology. 2015;36:57-62. doi:10.3174/ajnr.A3998
- Voon CC, Meineke J, Wiltgen T, McGinnis J, Berg R, Preibisch C, et al. Quantitative susceptibility mapping of deep gray matter in MS: association with clinical scores and brain volume measures. Brain and Behavior. 2025;15:e70988. doi:10.1002/brb3.70988
- Williams T, John N, Calvi A, Bianchi A, De Angelis F, Doshi A, et al. Investigating the relationship between thalamic iron concentration and disease severity in secondary progressive multiple sclerosis using quantitative susceptibility mapping: cross-sectional analysis from the MS-STAT2 randomized controlled trial. NeuroImage: Reports. 2024;4:100216. doi:10.1016/j.ynirp.2024.100216
- Marcille M, Hurtado Rua S, Tyshkov C, Jaywant A, Comunale J, Kaunzner UW, et al. Disease correlates of rim lesions on quantitative susceptibility mapping in multiple sclerosis. Scientific Reports. 2022;12:4411. doi:10.1038/s41598-022-08477-6
- Cagol A, Ocampo-Pineda M, Lu PJ, Weigel M, Barakovic M, Melie-Garcia L, et al. Advanced quantitative MRI unveils microstructural thalamic changes reflecting disease progression in multiple sclerosis. Neurology: Neuroimmunology & Neuroinflammation. 2024;11:e200299. doi:10.1212/NXI.0000000000200299