A 2026 Australian co-design study found that 70 of 73 surveyed health professionals, plus all 5 people with lived experience and all 6 carers interviewed, described outpatient care after eating-disorder hospital discharge as inadequate.
Research Highlights
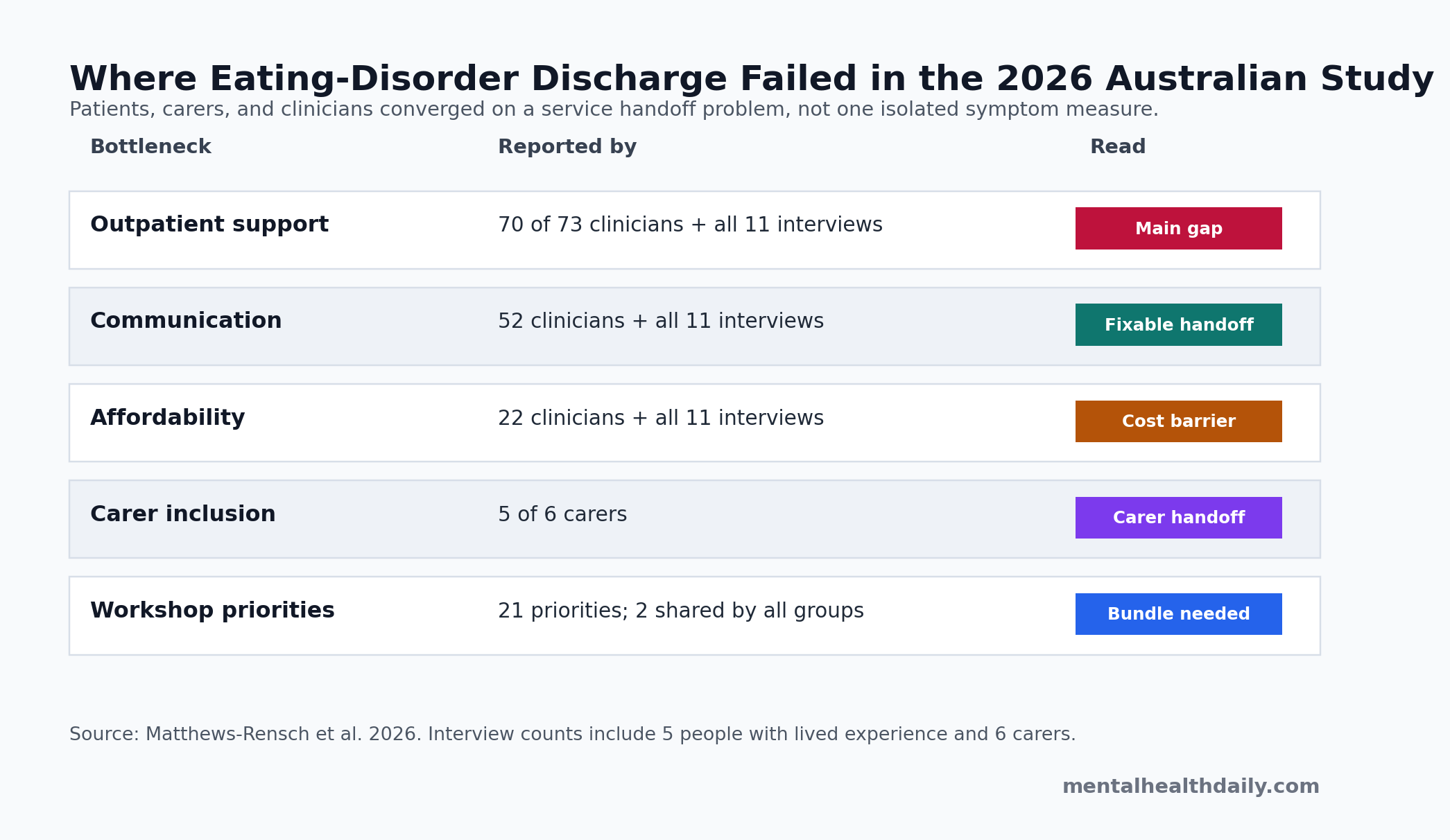
- Outpatient care was the main gap: 70 of 73 surveyed health professionals and all 11 interviewed patients/carers said care after hospital discharge could be inadequate.
- Communication failed early: 52 health professionals plus all 5 people with lived experience and all 6 carers described discharge communication from or within inpatient services as a serious problem.
- Costs followed patients home: all 11 interview participants and 22 surveyed health professionals raised financial strain, even when subsidized outpatient appointments were available.
- Carers became the default system: 5 of 6 carers felt excluded from inpatient treatment or discharge planning while still being expected to take over support immediately after discharge.
- The evidence is service-design evidence: the study used 5 lived-experience interviews, 6 carer interviews, 73 clinician surveys, and 7 workshop participants, so it maps discharge failures rather than proving any single intervention works.
Eating-disorder hospital discharge is the handoff from inpatient medical or psychiatric stabilization to outpatient care, primary care, day programs, family support, peer support, or no meaningful support at all. For anorexia nervosa and related eating disorders, that handoff is not a paperwork detail; it is the point where 24/7 structure disappears and the person has to eat, rest, travel, pay bills, attend appointments, manage relapse pressure, and rebuild autonomy outside the ward.
Matthews-Rensch et al. studied that handoff in Australia using interviews, clinician questionnaires, and workshops. The headline result is blunt: patients, carers, and clinicians described a gap between life-saving inpatient care and the actual home environment people return to.
70 of 73 Clinicians Said Outpatient Care Could Be Inadequate
The 2026 study used experience-based co-design, a service-design method that brings patients, carers, and staff into the same problem-mapping process. Stage 1 included interviews with 5 women who had lived experience of adult eating-disorder admission and discharge, interviews with 6 carers, and questionnaires from 73 health professionals. Stage 2 used workshops with 2 people with lived experience, 2 carers, and 3 health professionals.
The study sample was small on the patient and carer side, but the pattern was not subtle. Every interviewed patient and carer, and 70 of 73 surveyed health professionals, described outpatient care after discharge as potentially inadequate. Participants pointed to 3 linked failures:
- Availability: stepped-down services were described as limited, waitlisted, or unavailable after hospital discharge.
- Intensity: ordinary appointments could not always replace 24/7 inpatient structure, meal support, monitoring, and psychological containment.
- Navigation: patients and families often had to search across fragmented websites, referrals, private clinicians, and public systems while the eating disorder was still active.
Evidence-strength note: this design can identify recurring service failures and priorities for a future model of care. It cannot show that a discharge navigator, home meal support, peer worker, or day program reduces relapse, readmission, or mortality.
Discharge Communication Was a 52-Clinician Problem
Communication problems were one of the most concrete findings. All 11 interviewed patients and carers, along with 52 surveyed health professionals, raised communication from or within inpatient services as a serious problem.
The reported failures were ordinary enough to be operationally fixable: delayed discharge summaries, incomplete summaries, missing input from the inpatient multidisciplinary team, information not reaching every outpatient clinician, and incorrect details that then had to be fixed during appointments that should have been used for care.
Discharge planning means more than telling the patient to see a general practitioner or outpatient therapist. In this setting it has to name the eating plan, medical monitoring, psychiatric risk plan, dietetic support, meal-support logistics, carer role, contingency thresholds, and who owns the next step if the person deteriorates.
That is why a weak discharge summary can become a clinical problem. If the outpatient team receives vague or late information, the first post-discharge visit turns into reconstruction work. If carers are not included, the people expected to supervise meals, transport, and crisis decisions may not know what the hospital expected them to do.
Carers Were Excluded and Then Handed the Work
Carer involvement was one of the clearest practical contradictions. Five of 6 carers said they felt excluded from inpatient treatment and discharge planning once the patient was legally an adult. At the same time, carers were expected to take over daily support once the person returned home.
The gap is especially sharp in anorexia nervosa because illness severity can impair judgment around food, weight, risk, and medical need. The study described carers being left to manage meal support, transport, treatment research, family strain, work disruption, and their own exhaustion with limited guidance.
Carers were not asking to replace autonomy with surveillance. The better reading is that discharge planning needs a consent-aware carer role: what the patient agrees to share, what carers need to know to keep the transition workable, and what clinicians should not outsource to families without training or backup.
Clark Bryan et al. found a similar pattern in a 2022 UK qualitative study of 23 patients and 20 carers leaving intensive anorexia treatment. Patients needed continuity and support for recovery ambivalence; carers needed involvement, information, and a more supportive transition process. The Australian study is narrower and more local, but it lands in the same place: the family often absorbs the discharge gap.
Money and Geography Made the Handoff Unequal
Affordability was not a side concern. All 11 interviewed patients and carers raised financial strain, and 22 surveyed health professionals flagged out-of-pocket expenses. Participants described the cost of therapy, dietetic appointments, medical visits, transport, supplements, unpaid leave, reduced work hours, and private options when public services were unavailable or delayed.
Regional access added another layer. Interviewed regional participants described difficulty attending services, and some participants reported interstate travel for care they considered appropriate. That makes “follow up as an outpatient” a weak instruction when the outpatient service is distant, unaffordable, waitlisted, or not matched to eating-disorder severity.
Models-of-care evidence: Pehlivan et al. reached a compatible systems-level conclusion in a 2022 rapid review of eating-disorder services.
Specialist services, stepped care, and clearer referral pathways may improve detection and care. Many Western health systems still struggle with waitlists, stigma, referral friction, and patchy integration between inpatient, outpatient, and primary-care settings.
Aftercare Trials Still Do Not Give a Simple Fix
The practical temptation is to pick one favored solution: peer workers, care navigators, home visits, digital guided self-help, day programs, or family support. Adjacent evidence says the answer is probably a bundle, not a single add-on.
Giel et al. reviewed randomized post-inpatient aftercare trials for anorexia nervosa and found only 7 randomized controlled trials, with no clear evidence favoring one adult aftercare approach. Low-threshold guided self-help had uptake and dropout problems, mobile approaches were promising but under-tested, and cognitive-behavioral psychotherapy evidence was limited.
ECHOMANTRA and TRIANGLE show the calibration problem:
- Qualitative fit: a 2024 study of the hybrid guided self-help intervention found that patients and carers valued online groups, peer community, and transition tools, but they also wanted more personalization.
- Trial scale: the later TRIANGLE randomized trial included 371 patient-carer dyads across 31 inpatient/day-patient sites and tested digital aftercare augmentation against treatment as usual.
- Practical read: this is the right evidentiary direction, but it still does not turn discharge into a solved problem for every health system.
Franklin et al. tested a narrower family-navigator model after adolescent anorexia hospitalization: 23 navigator patients were compared with 23 historical controls, and navigator patients attended more total scheduled visits and more individual therapy visits. That is encouraging adherence evidence, not proof that a navigator alone prevents relapse.
The Best Discharge Model Looks Like Infrastructure
The Matthews-Rensch study produced 21 workshop priorities. Only 2 were shared across all participant groups: stronger peer/lived-experience support and more holistic, person-centered care. Health professionals also prioritized a dedicated eating-disorder care navigator, and carers pushed for clear, well-communicated discharge plans.
Those priorities can be translated into a practical discharge bundle:
- Before discharge: a written plan that names medical monitoring, meal support, psychological support, dietetic support, emergency thresholds, and the next appointment date.
- At discharge: a consent-aware carer handoff, timely discharge summary, and direct communication with the outpatient clinician or general practitioner.
- After discharge: rapid follow-up, active navigation, peer support, and practical help with meals, transport, and service access.
- Across the system: trained eating-disorder staff, regional access planning, affordable care pathways, and non-tokenistic lived-experience involvement.
Livanou et al. reported similar transition themes in a 2025 co-production study focused on young people moving from child/adolescent to adult eating-disorder services: complexity, carer involvement, separation from familiar services, and coping/self-management needs. The population differs from the Australian adult-discharge study, but the service lesson is aligned. Transition failure is rarely just patient motivation. It is often poor infrastructure at exactly the moment the person needs structure most.
Questions About Eating-Disorder Discharge
Did this study prove that outpatient care causes relapse after discharge?
No. The study did not measure relapse as a clinical outcome and cannot prove causation. It showed that patients, carers, and clinicians repeatedly described the discharge-to-outpatient handoff as fragmented, under-resourced, expensive, and isolating.
Was this only about anorexia nervosa?
All 5 lived-experience interview participants had anorexia nervosa, though 2 reported other eating-disorder diagnoses during their illness course. The broader service problem may apply to other eating disorders, but the patient interview evidence is strongest for anorexia nervosa and medically compromised discharge.
Do digital programs fix the discharge gap?
Digital aftercare can help some patients and carers, especially when it provides structure, skills, and peer contact. The evidence does not support treating digital support as a one-to-one substitute for timely outpatient care, meal support, medical monitoring, and trained clinical backup.
What is the most actionable finding for hospitals?
The first fix is not glamorous: discharge summaries, carer-inclusive planning when consent allows, confirmed outpatient handoff, and rapid follow-up. Those steps do not solve eating-disorder recovery, but they reduce the chance that patients leave 24/7 care into an administrative void.
References
- Matthews-Rensch K, Elwyn R, Jones L, Young A. “Always, always have hope:” persons with lived experience, carers and health professionals’ experiences before and after discharge from hospital for an eating disorder. Journal of Eating Disorders. 2026. doi:10.1186/s40337-026-01621-x
- Giel KE, Behrens SC, Schag K, et al. Efficacy of post-inpatient aftercare treatments for anorexia nervosa: a systematic review of randomized controlled trials. Journal of Eating Disorders. 2021;9:129. doi:10.1186/s40337-021-00487-5
- Clark Bryan D, Macdonald P, Cardi V, et al. Transitions from intensive eating disorder treatment settings: qualitative investigation of the experiences and needs of adults with anorexia nervosa and their carers. BJPsych Open. 2022;8(4):e137. doi:10.1192/bjo.2022.535
- Pehlivan MJ, Miskovic-Wheatley J, Le A, et al. Models of care for eating disorders: findings from a rapid review. Journal of Eating Disorders. 2022;10:166. doi:10.1186/s40337-022-00671-1
- Clark Bryan D, Rowlands K, Macdonald P, et al. Transition support for patients admitted to intensive treatment for anorexia nervosa: qualitative study of patient and carer experiences of a hybrid online guided self-help intervention (ECHOMANTRA). BJPsych Open. 2024;10(3):e81. doi:10.1192/bjo.2023.642
- Treasure J, Rowlands K, Cardi V, et al. Digital augmentation of aftercare for patients with anorexia nervosa: the TRIANGLE RCT and economic evaluation. Health Technology Assessment. 2025;29(31):1-162. doi:10.3310/ADLS3672
- Franklin EV, Black M, Wrobel KA, et al. A family navigator improves post-discharge treatment adherence among adolescents with anorexia nervosa: a pilot study. Journal of Eating Disorders. 2025;13:109. doi:10.1186/s40337-025-01315-w
- Livanou M, Heneghan A, Hill G, et al. Co-producing a transition model of care for eating disorders: lessons learned from a multi-perspective qualitative study with young people, carers and mental health professionals. Journal of Eating Disorders. 2025;13:106. doi:10.1186/s40337-025-01304-z