A 2026 multi-cohort fMRI study found that a signal often treated as physiological noise tracked nicotine dependence, cue-induced craving, abstinence, and stimulant effects.1 During cigarette cue exposure, systemic low-frequency oscillation amplitude correlated with nicotine dependence at r = −0.32, p = .009.
Research Highlights
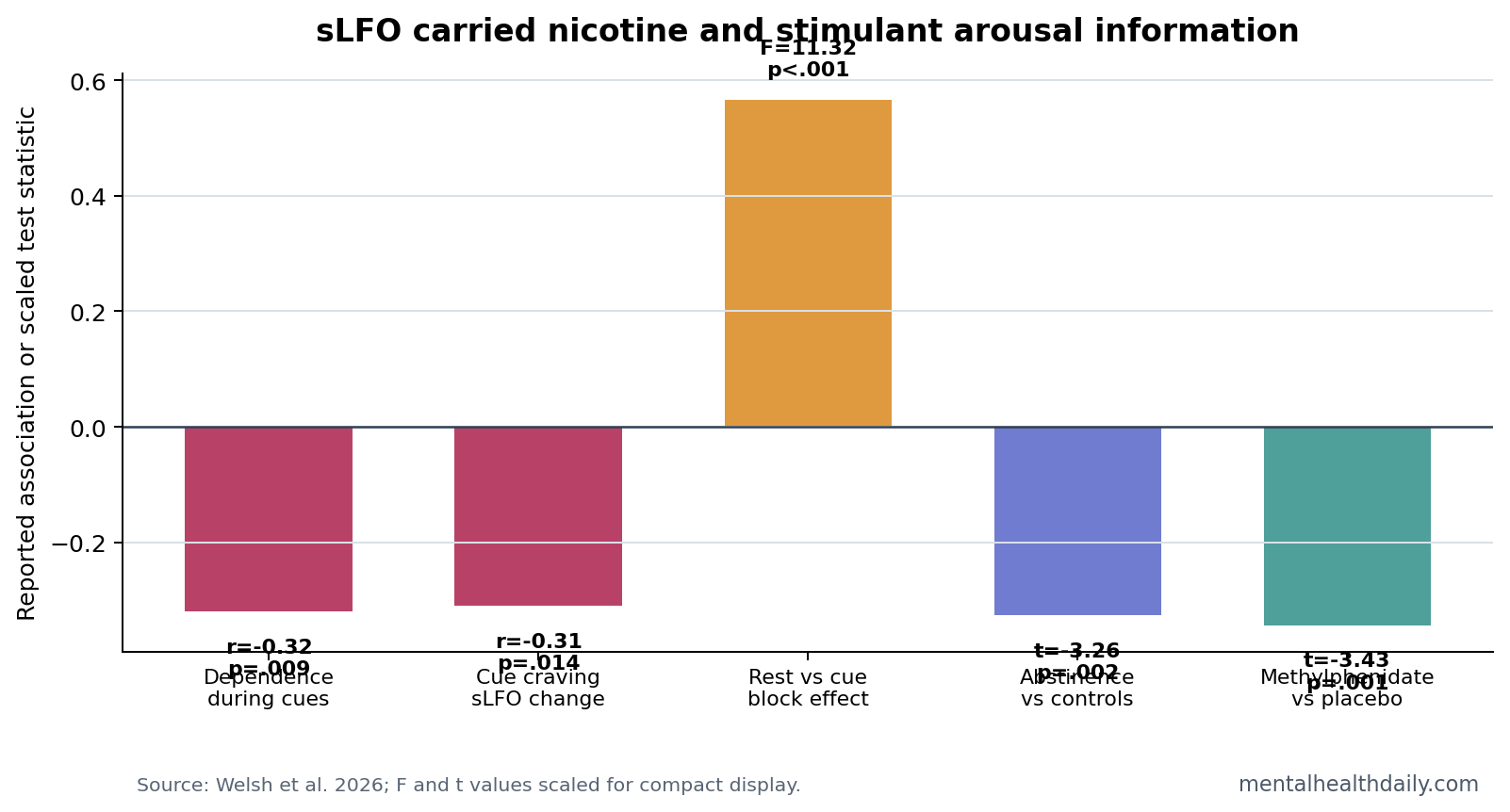
- Dependence tracked cue-period physiology: In 64 smokers, higher average sLFO amplitude during cigarette cue exposure was negatively associated with nicotine dependence, r = −0.32, p = .009.1
- Craving tracked signal change: sLFO change from the first cue block to the last cue block was inversely associated with cue-induced craving, r = −0.31, p = .014.1
- Cues changed the signal: Brainwide average sLFO differed across rest and cue blocks, F(5,63) = 11.32, p < .001.1
- Abstinence and satiety separated: Smokers in abstinence had higher sLFO than controls, t(99) = −3.26, p = .002, and nicotine satiety reduced sLFO, t(64) = −4.51, p < .001.1
- Stimulants pushed the same arousal axis: Methylphenidate reduced sLFO in healthy controls, t(58) = −3.434, p = .001, and sLFO reductions related to task performance.1
Systemic low-frequency oscillation (sLFO) is a slow, brainwide physiological fluctuation visible in fMRI data. It is driven largely by vascular, respiratory, cardiac, and arousal-related physiology rather than by local neuronal firing alone. Lower sLFO amplitude has been interpreted as higher physiological arousal in prior work.
Functional magnetic resonance imaging (fMRI) measures blood-oxygen-level-dependent signal changes. Standard analysis often tries to remove global physiological signals so local brain networks are easier to interpret. Welsh et al. asked whether one of those removed signals contains addiction-relevant information.
Nicotine Dependence Was Lower When Cue-Period sLFO Was Higher
In the cigarette cue-reactivity cohort, 64 individuals who smoked tobacco viewed smoking and neutral cues during fMRI. During cue exposure, average brainwide sLFO amplitude was negatively associated with Fagerstrom Test for Nicotine Dependence scores, r = −0.32, p = .009.1
Plain English: heavier nicotine dependence was linked to lower cue-period sLFO amplitude. If lower sLFO indexes higher arousal, the result fits an addiction model in which smoking cues push dependent users into a stronger physiological arousal state.
The same relationship was not present at rest: sLFO and dependence were unrelated before cue exposure, r = −0.047, p = .71. That context dependence is important because it suggests the signal became informative under drug-cue challenge.
Cue-Induced Craving Tracked the Change Across the Task
Welsh et al. also examined how sLFO changed across the cue-reactivity task. Greater cue-induced craving was associated with a smaller cue-related increase in brainwide average sLFO, r = −0.31, p = .014. The association remained after controlling for first-cue-block sLFO, r = −0.26, p = .04.1
That result links the signal to subjective craving and dependence history. It also clarifies why a single resting-state scan may miss addiction-relevant physiology: the useful signal appeared during cue exposure and across cue blocks.
Abstinence Raised sLFO and Nicotine Satiety Reduced It
In a chronic nicotine-use cohort, brainwide average sLFO did not differ between smokers and matched controls at baseline. Under abstinence, smokers showed higher sLFO than controls, t(99) = −3.26, p = .002. During nicotine satiety, sLFO decreased significantly, t(64) = −4.51, p < .001.1
This pattern makes the signal harder to dismiss as scanner artifact. Abstinence and nicotine satiety are physiological states with different arousal, withdrawal, and autonomic profiles. The sLFO moved with those states.
Methylphenidate Reduced sLFO in Healthy Controls
Methylphenidate also reduced brainwide average sLFO at rest compared with placebo, t(58) = −3.434, p = .001. During the Multi-Source Interference Task, methylphenidate-related sLFO reductions were associated with reaction-time changes in congruent and incongruent conditions.1
Methylphenidate is a dopamine and norepinephrine reuptake inhibitor used for ADHD and narcolepsy. Its inclusion matters because it tests whether the sLFO tracks psychostimulant arousal outside nicotine dependence. The answer was directionally consistent: stimulant exposure reduced the signal.
This cross-drug pattern is important for interpretation. Nicotine satiety and methylphenidate are not the same pharmacologic state, but both can increase catecholamine-linked arousal. Seeing sLFO move in the same broad direction across nicotine and methylphenidate makes the signal look less like a tobacco-only artifact.
The result also limits the claim. A shared arousal-sensitive signal does not tell researchers whether a person is craving nicotine, responding to a stimulant, changing respiratory pattern, or shifting vigilance unless the task context and behavioral data are known. sLFO gains meaning when it is paired with cue exposure, abstinence status, drug condition, and performance.
Removing “Noise” Can Remove Clinically Relevant Physiology
fMRI researchers often remove global physiological signals to isolate local neural activity. That can be valid for some questions. The Welsh et al. result shows the tradeoff: a signal treated as nuisance can carry information about nicotine dependence, craving, abstinence, satiety, and stimulant exposure.
- For addiction research: sLFO may capture arousal physiology that symptom scales and regional activation maps miss.
- For fMRI methods: preprocessing choices can erase meaningful physiology if the removed signal is never analyzed.
- For biomarker claims: correlation with dependence and craving is useful, but it is not a stand-alone diagnostic marker.
Evidence-strength note: the study used multiple cohorts and converging nicotine/stimulant tests, which strengthens the method argument. The clinical findings are still correlational. sLFO amplitude should be treated as a candidate physiological marker, not proof that the signal causes craving or dependence.
What Addiction Studies Should Do With sLFO
The immediate use is methodological. Addiction fMRI studies often focus on regional cue reactivity: ventral striatum, medial prefrontal cortex, anterior cingulate, insula, and related control networks. Those regional maps remain useful, but sLFO adds a brainwide physiological layer that can change during the same task.
A stronger future cue-reactivity study would report both layers:
- Regional activation: which addiction-relevant circuits changed during cues, abstinence, satiety, or treatment.
- Systemic physiology: whether sLFO amplitude changed with arousal, craving, withdrawal, or stimulant exposure.
- Behavioral anchoring: whether the physiological signal tracked craving ratings, dependence scores, reaction time, lapse risk, or treatment response.
That combined approach avoids 2 weak extremes. It does not throw away physiology as meaningless noise, and it does not pretend a global fMRI signal is a precise addiction diagnosis.
Why the Resting-State Null Helps the Cue-Reactivity Claim
The dependence correlation was not present at rest, where sLFO and nicotine dependence were essentially unrelated (r = −0.047, p = .71).1 That might look like a weakness, but it actually sharpens the interpretation: nicotine dependence became visible in the physiological signal when the task presented cigarette cues.
Addiction is often state-dependent. A person can look stable at baseline and then show a different physiological profile during withdrawal, cue exposure, stress, drug satiety, or decision pressure. The sLFO result fits that model because cue context made the signal clinically informative.
That also changes how future biomarker work should be designed. A resting scan alone may understate addiction-relevant physiology. A cue-reactivity scan, paired with craving ratings and dependence scores, can test whether systemic physiology changes when drug-related motivation is actually engaged.
The same logic applies to treatment trials. If a medication or behavioral intervention reduces cue-induced craving, researchers can ask whether regional cue reactivity and sLFO both shift. Agreement between subjective craving, task behavior, regional activation, and systemic physiology would be much stronger than any single metric alone.
For readers, the useful correction is that “noise” in brain imaging is sometimes a label for biology that the analysis was not built to study. Breathing, vascular timing, autonomic arousal, and vigilance can interfere with local-network maps, but those same processes can be central to addiction, craving, and withdrawal.
Welsh et al. did not show that sLFO is ready for clinical decision-making. The study showed that deleting systemic physiology by default can hide information that becomes meaningful when the question is nicotine dependence, cue reactivity, or psychostimulant arousal.
That is a methods warning and an addiction-biology clue at the same time.
The next step is replication with cleaner clinical anchors: current smoking intensity, verified abstinence, withdrawal severity, craving change, relapse follow-up, medication status, and respiratory or cardiac measures collected during scanning. If sLFO still tracks cue-induced craving after those checks, the signal becomes much harder to dismiss as generic scanner physiology.
It would also help to compare sLFO with ordinary autonomic measures. Heart rate variability, respiration, skin conductance, pupil size, and subjective arousal could clarify whether the fMRI-derived signal is mostly vascular timing, vigilance, withdrawal physiology, or a broader arousal composite.
Those checks would make the biomarker claim narrower, but much more useful.
Questions About sLFO, fMRI, and Nicotine
Is sLFO brain activity or body physiology?
It is mainly systemic physiology visible inside fMRI data. It can still be clinically relevant because arousal, vascular tone, breathing, and autonomic state are part of brain-behavior biology.
Does this make fMRI useful for diagnosing nicotine dependence?
No. The study found dependence and craving correlations. Diagnosis still comes from behavior, symptoms, use pattern, withdrawal, impairment, and clinical history.
Should fMRI studies always keep the global signal?
No single preprocessing choice fits every question. The practical lesson is to understand what is being removed and, when physiology is relevant, analyze it directly instead of treating it as meaningless noise.
References
- Welsh RC, et al. Functional magnetic resonance imaging signals from systemic low-frequency oscillation in individuals who use nicotine. Biological Psychiatry: Global Open Science. 2026. doi:10.1016/j.bpsgos.2026.100720
- Tong Y, Frederick BD. Tracking cerebral blood flow in BOLD fMRI using recursively generated regressors. Human Brain Mapping. PubMed
- Power JD, et al. The global signal and arousal-related physiology in resting-state fMRI. NeuroImage. PubMed
- Jasinska AJ, et al. Factors modulating neural reactivity to drug cues in addiction: a survey of human neuroimaging studies. Neuroscience & Biobehavioral Reviews. PubMed