A 2026 study involving 118 prostate cancer survivors found the clearest lifestyle-cognition signal around smoking: smokers learned fewer words across repeated verbal-memory trials, while obesity and physical activity produced narrower reaction-time findings and no significant anxiety or depression differences.
Research Highlights
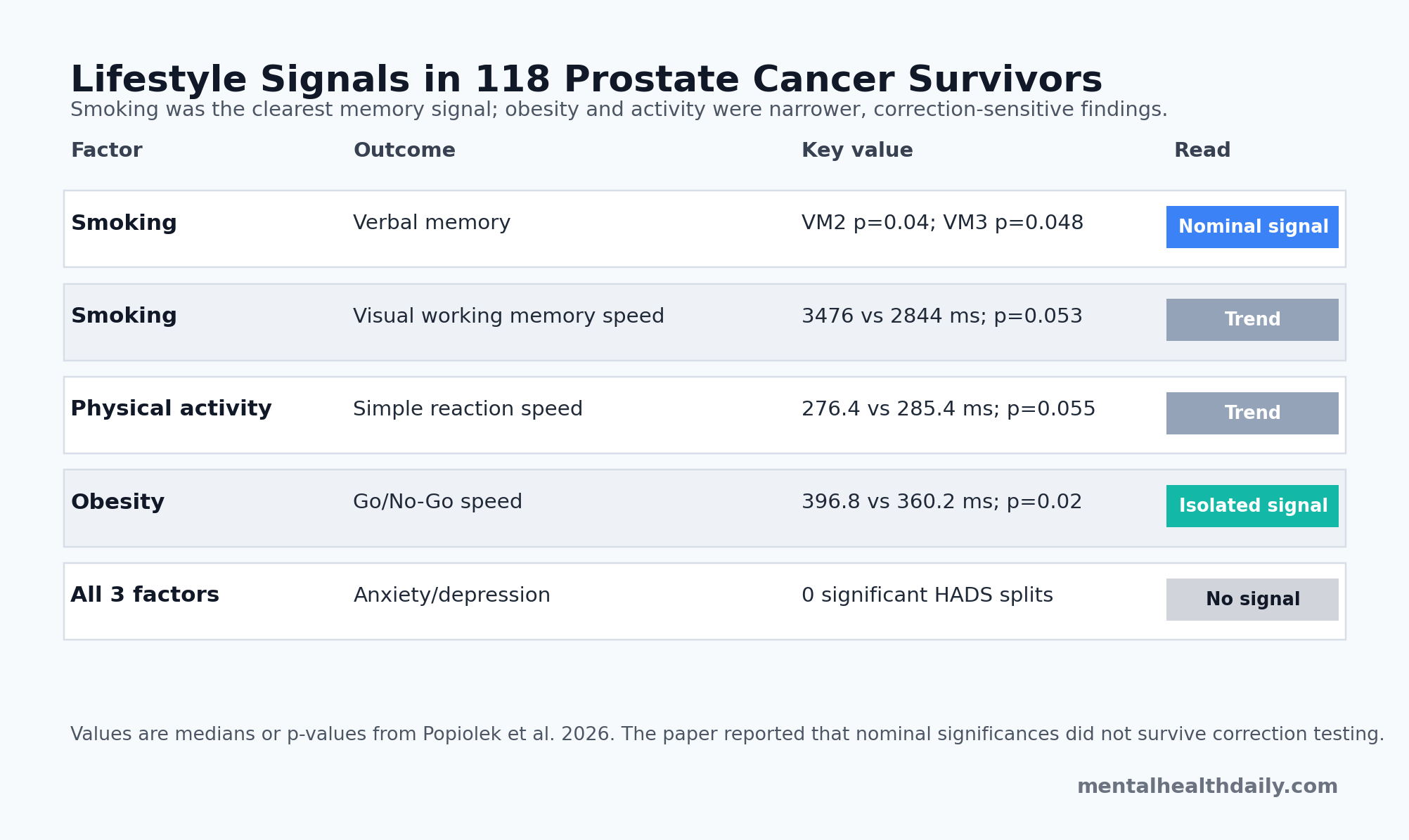
- Smoking tracked verbal learning: in 118 prostate cancer survivors, smokers scored lower on Verbal Memory Test trial 2 (p = 0.04) and trial 3 (p = 0.048), with trial 3 medians of 8 words in never-smokers vs. 7 in smokers.
- Visuospatial speed was weaker: smokers had slower Visual Working Memory Test correct-response times than never-smokers, 3476 ms vs. 2844 ms, but the main smoker/non-smoker comparison was only near-significant (p = 0.053).
- Physical activity was not the broad signal: active men had slightly faster simple reaction times than inactive men, 276.4 ms vs. 285.4 ms, but the comparison remained a trend (p = 0.055) and memory/executive measures did not separate cleanly.
- Obesity showed one reaction-time result: men with obesity had slower Go/No-Go reaction times than men without obesity, 396.8 ms vs. 360.2 ms (p = 0.02), while other cognitive tests were not significantly different.
- Mood scores did not split by lifestyle group: Hospital Anxiety and Depression Scale scores showed 0 significant differences across smoking, physical-activity, or obesity comparisons.
Cancer-related cognitive impairment means problems with memory, attention, processing speed, or executive control that appear before, during, or after cancer treatment. In prostate cancer, the usual suspects include age, surgery recovery, androgen deprivation therapy, sleep disruption, depression, anxiety, vascular disease, inflammation, and the background health behaviors that shape brain and cardiovascular risk.
Popiolek et al. tested a narrower question after radical prostatectomy: among men already treated surgically for prostate cancer, did smoking, exercise frequency, or obesity map onto computerized cognition tests or Hospital Anxiety and Depression Scale scores?
Smokers Recalled Fewer Words Across Repeated Memory Trials
The 2026 cohort included 118 men with histologically confirmed prostate adenocarcinoma, assessed after radical prostatectomy. Median age was 66 years, and median time from surgery was 19 months. Smoking history split the sample into 66 never-smokers, 41 former smokers, and 11 current smokers.
Verbal Memory Test: participants heard a 10-word list and recalled as many words as possible across repeated learning trials. The test measures how efficiently repeated exposure builds short-term verbal learning.
Smokers and former smokers performed worse than never-smokers on the second and third trials. Trial 2 medians were both 7 words, but the distributions differed enough to reach p = 0.04: never-smokers had an interquartile range of 7-8 words, while smokers had 6-8. Trial 3 showed a clearer median split, 8 words in never-smokers vs. 7 in smokers, with p = 0.048.
Later verbal-memory trials leaned in the same direction without crossing the conventional significance line. Trial 4 was 8 vs. 8 words (p = 0.06), and trial 5 was 8 vs. 8 words (p = 0.055), again with lower interquartile ranges among smokers.
Interpretive key: this is not a dementia diagnosis or proof that smoking caused memory loss. It is a small, cross-sectional survivorship signal showing weaker verbal learning among men with smoking exposure.
Current Smoking Looked Worse Than Past Smoking
The smoking result became more pointed when the researchers separated never-smokers, former smokers, and current smokers. Current smokers performed significantly worse on the second verbal-memory trial and had slower Visual Working Memory Test response times.
Visual Working Memory Test: participants saw playing cards in screen locations and later had to identify where those cards had appeared. Correct-response time in the main smoker/non-smoker comparison was 3476 ms among smokers vs. 2844 ms among never-smokers, a near-significant difference (p = 0.053). The current-smoker subgroup analysis reportedly reached significance for slower visuospatial response time.
That pattern fits broader smoking-cognition evidence without requiring overstatement. Smoking can affect vascular health, neurotransmitter systems, oxidative stress, inflammation, and cancer prognosis. Mons et al. reported that long-term cessation was associated with lower cognitive-decline risk in older adults, while Visscher et al. linked smoking to poorer recovery of urinary and sexual function after prostatectomy.
For this specific prostate-cancer cohort, the practical signal is memory first, speed second. Verbal learning separated more consistently than reaction-time measures, and anxiety/depression did not explain the smoking split.
Physical Activity Did Not Reproduce Strong Exercise-Cognition Findings
Physical activity was measured by self-reported frequency of intentional activity per week. In the cohort, 40 men reported no physical activity, 24 reported activity 1 time per week, 22 reported 2-3 times per week, and 32 reported more than 3 times per week.
When the researchers collapsed the sample into active vs. inactive groups, active men had slightly faster simple reaction times: 276.4 ms vs. 285.4 ms. The comparison was close but not significant (p = 0.055), and the broader cognition pattern did not line up behind it.
- Memory: verbal-memory and delayed-recall comparisons did not show significant active-vs.-inactive advantages.
- Executive control: Go/No-Go accuracy and reaction-time measures did not clearly favor active men.
- Mood: HADS anxiety and depression scores did not differ significantly by activity group.
This partially contrasts with adjacent prostate-cancer exercise work. Gaynor et al. found exercise associated with better attention, memory, and executive function in older men receiving androgen deprivation therapy. Fang et al. reported exercise-intervention benefits for social and cognitive functioning in a 2020 meta-analysis of men with prostate cancer.
The discrepancy is plausible. Popiolek et al. measured exercise frequency rather than supervised training, aerobic capacity, resistance dose, intensity, or adherence. Their cohort also had relatively little adjuvant therapy exposure; only 9 men had hormone therapy and 22 had radiotherapy. Exercise may matter most when treatment creates a stronger cognitive stressor, or when exercise is measured with more than a frequency question.
Obesity Produced One Executive-Speed Difference, Not a Global Cognitive Pattern
Body mass index (BMI) estimates weight adjusted for height. In this cohort, median BMI was 27.2 kg/m²; 68 men were overweight, 26 had obesity, and only 24 were in the normal-weight range.
Obesity separated one cognitive measure. Men without obesity had a median Go/No-Go reaction time of 360.2 ms, while men with obesity had a median of 396.8 ms (p = 0.02). The Go/No-Go task measures response inhibition: press for one stimulus, withhold for another, and do so quickly enough that errors and slowing reveal executive-control burden.
Other cognitive measures did not show significant obesity differences. Verbal memory, delayed recall, visual working memory, simple reaction time, anxiety, and depression were not meaningfully different between men with and without obesity.
Evidence-strength note: the obesity finding is isolated. Only 26 men were in the obesity group, and the paper explicitly reported that none of the observed significant findings remained after correction testing. The result is worth following because obesity can affect inflammation, vascular health, insulin signaling, sleep apnea risk, and prostate-cancer progression, but it is not enough to claim that obesity broadly impaired cognition in this cohort.
Mood Symptoms Were Not the Lifestyle Signal
Hospital Anxiety and Depression Scale (HADS) scores did not differ significantly by smoking, physical activity, or obesity. Median anxiety and depression scores were low overall: in the smoker/non-smoker table, HADS-A medians were 2 in never-smokers and 4 in smokers, while HADS-D medians were 2 and 3. Those differences did not reach significance.
That null mood pattern matters for interpretation because cancer-survivor cognition can be confounded by depression, anxiety, fatigue, insomnia, pain, and treatment burden. Jarzemski et al. previously reported cognitive, depression, and anxiety differences among prostatectomy patients with and without adjuvant treatment. In Popiolek et al., the lifestyle split showed up more in selected cognitive tests than in affective symptoms.
Low mood-score separation leaves mood clinically relevant in prostate-cancer survivorship, but this particular sample, with psychiatric disorders excluded and limited adjuvant treatment exposure, did not show strong HADS group differences by lifestyle factor.
Smoking Had the Most Coherent Correction-Sensitive Signal
A defensible ranking starts with smoking rather than a broad lifestyle explanation:
- Smoking had the most coherent signal: verbal-memory learning was lower in smokers across multiple trials, and current smoking looked worse than former smoking in subgroup analysis.
- Obesity had one executive-speed signal: Go/No-Go reaction time was slower in men with obesity, but other cognitive and mood measures did not follow.
- Physical activity was under-measured: a simple frequency variable produced only a reaction-time trend, even though adjacent exercise literature in prostate cancer is more favorable.
- Mood did not explain the pattern: HADS anxiety and depression scores did not differ significantly across lifestyle groups.
Small cross-sectional cohorts are best used as signal finders, not verdict machines. Popiolek et al. point toward smoking as the most actionable candidate for prostate-cancer survivorship cognition studies, with exercise dose, body composition, androgen-deprivation exposure, vascular disease, sleep, and treatment history measured more tightly in the next round.
Questions About Smoking, Memory, and Prostate Cancer Survivorship
Did the study show that smoking causes memory problems after prostate cancer?
No. The design was cross-sectional, so it cannot prove causation. It showed that men with smoking exposure had worse verbal-learning performance than never-smokers in this 118-person post-prostatectomy cohort.
Was physical activity useless for cognition?
No. This study measured activity frequency crudely and found only a near-significant simple-reaction-time trend. Other prostate-cancer exercise studies, especially in men receiving androgen deprivation therapy, suggest exercise may support cognition when dose and treatment context are measured more carefully.
Should the obesity result change clinical advice?
Not by itself. The obesity group had slower Go/No-Go reaction time, but the finding was isolated and correction-sensitive. Weight, metabolic health, sleep apnea, vascular risk, and treatment side effects still matter in survivorship care; this paper does not prove that BMI alone explains cognitive function.
Why did anxiety and depression not differ by lifestyle group?
The cohort excluded men with psychiatric disorders and had low median HADS scores. That restriction can make mood-group differences harder to detect, especially in a modest sample.
References
- Popiolek A, Brzoszczyk B, Niemczuk E, Borkowska A, Jarzemski P, Bielinski M. Smoking Habits, Physical Activity and BMI as Predictors of Cognitive and Affective Function in Patients with Prostate Cancer. Research and Reports in Urology. 2026;18:572735. doi:10.2147/RRU.S572735
- Jarzemski P, Brzoszczyk B, Popiolek A, et al. Cognitive function, depression, and anxiety in patients undergoing radical prostatectomy with and without adjuvant treatment. Neuropsychiatric Disease and Treatment. 2019;15:819-829. doi:10.2147/NDT.S200501
- Gaynor AM, Flaherty KR, Root JC, Salas-Ramirez KY, Scott JM, Nelson CJ. Exercise associated with cognitive function in older men with prostate cancer undergoing androgen deprivation therapy. International Journal of Behavioral Medicine. 2023;30(6):924-929. doi:10.1007/s12529-022-10150-1
- Fang YY, Lee YH, Chan JC, et al. Effects of exercise interventions on social and cognitive functioning of men with prostate cancer: a meta-analysis. Supportive Care in Cancer. 2020;28(5):2043-2057. doi:10.1007/s00520-019-05278-y
- Visscher J, Hiwase M, Bonevski B, O’Callaghan M. The association of smoking with urinary and sexual function recovery following radical prostatectomy for localized prostate cancer: a systematic review and meta-analysis. Prostate Cancer and Prostatic Diseases. 2024;27(2):222-229. doi:10.1038/s41391-023-00701-2
- Fluharty M, Taylor AE, Grabski M, Munafo MR. The association of cigarette smoking with depression and anxiety: a systematic review. Nicotine & Tobacco Research. 2017;19(1):3-13. doi:10.1093/ntr/ntw140
- Wilson RL, Taaffe DR, Newton RU, Hart NH, Lyons-Wall P, Galvao DA. Obesity and prostate cancer: a narrative review. Critical Reviews in Oncology/Hematology. 2022;169:103543. doi:10.1016/j.critrevonc.2021.103543