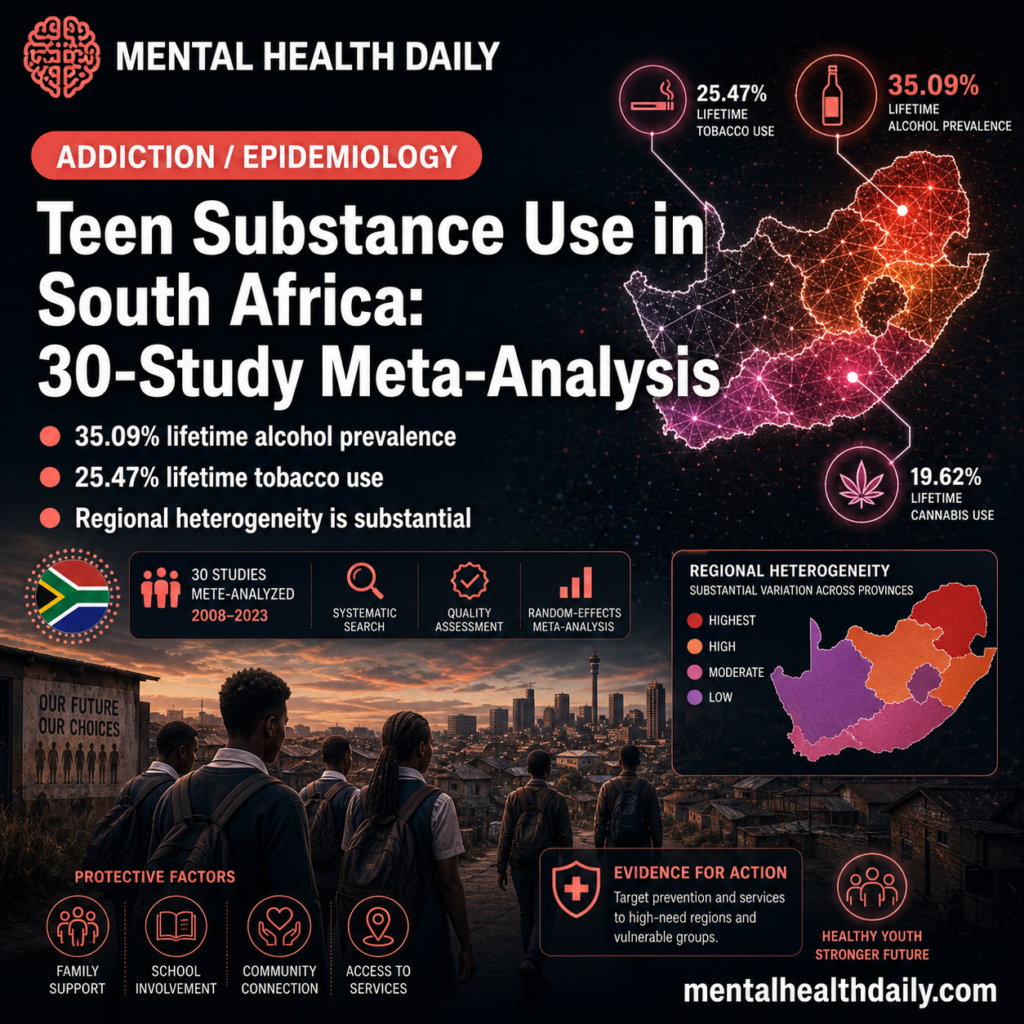
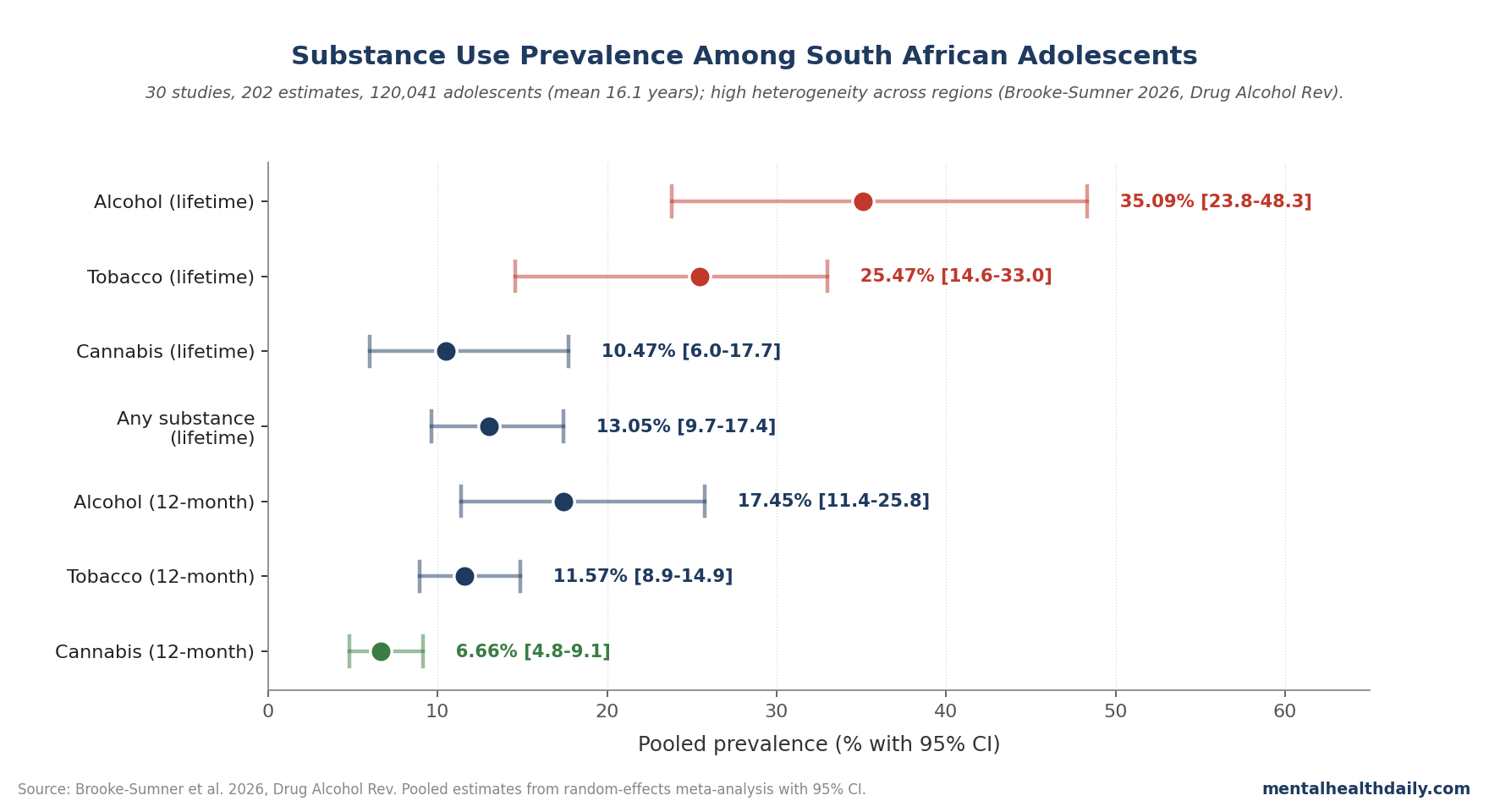
A 2026 PRISMA-compliant systematic review and meta-analysis in Drug and Alcohol Review consolidated 30 publications covering 202 prevalence estimates from 120,041 South African adolescents: pooled lifetime prevalence was 35.09% for alcohol use, 25.47% for tobacco use, and 10.47% for cannabis use.1
Research Highlights
- 30 publications, 202 estimates: pooled data covered 120,041 South African adolescents.
- Alcohol dominance: lifetime prevalence was 35.09% (95% CI 23.83–48.30).
- Nicotine + cannabis: lifetime prevalence was 25.47% for tobacco and 10.47% for cannabis.
- 12-month use: prevalence was 17.45% alcohol, 11.57% tobacco, and 6.66% cannabis.
- Local variation: 202 estimates varied by setting, school type, gender, and survey method.
The wide confidence intervals and substantial between-study heterogeneity are themselves the second important finding. South African adolescent substance use varies dramatically by region, school type, gender, and survey method.
Why Synthesizing South African Data Has Been Difficult
South Africa has a long history of substance-use research, but the evidence base comes from pieces that do not aggregate cleanly:1
- Regional variation: Western Cape data can look different from KwaZulu-Natal data.
- Sampling frame: township samples, suburban school samples, household surveys, and treatment-seeking samples capture different adolescents.
- Study design: cross-sectional surveys estimate prevalence, while longitudinal cohorts are needed to track trajectories.
Methodological upgrade: Brooke-Sumner et al. applied PRISMA methodology with random-effects pooling and meta-regression to handle the heterogeneity. Joanna Briggs Institute quality assessment screened studies for risk of bias. The result is the first national-scale synthesis that uses formal meta-analytic techniques rather than narrative aggregation.
The substantial heterogeneity (high I²) means the pooled estimates have wide confidence intervals. The 95% CI for alcohol — 23.83% to 48.30% — spans nearly 25 percentage points. That uncertainty isn’t a methodological flaw; it’s an accurate reflection of how variable substance use actually is across the country.
Adolescent Substance Use Raises Later Mental-Health Risk
Early substance use is a robust risk marker for later psychiatric morbidity. The developmental logic is easier to scan as mechanism labels:
- Neurodevelopmental disruption: the adolescent brain is still developing reward, prefrontal-control, and inhibitory networks. Substance exposure during this window can alter learning, reward sensitivity, impulse control, and stress reactivity in ways that do not map cleanly onto adult-onset use.2
- Trajectory effects: early initiation gives substance use more years to become habitual, socially reinforced, and biologically entrenched. Each earlier year of onset is associated with higher long-term risk for substance use disorder.2
The mental-health connection runs in both directions. Adolescents with depression, anxiety, ADHD, or trauma exposure are more likely to initiate substance use; substance use itself increases risk for subsequent depression, anxiety, and psychotic disorders. The bidirectional pattern is particularly strong for cannabis and psychotic-spectrum outcomes, where the early-onset, high-potency use pattern is most concerning.3
South Africa’s adolescent population is particularly exposed to layered risk factors that can make the same substance-use prevalence more clinically loaded:
- HIV and family illness burden: chronic stress can interact with mood, school attendance, caregiving roles, and household instability.
- Trauma exposure: violence and community instability increase the chance that substance use becomes coping behavior rather than experimentation.
- Economic precarity: unemployment, school instability, and household stress can increase exposure while reducing treatment access.
- Limited youth services: thin adolescent mental-health infrastructure means risky use is less likely to be caught early.
The 35% alcohol-exposure figure has to be read against this background.
The Cannabis Number Deserves Specific Attention
Lifetime cannabis prevalence of 10.47% in South African adolescents is in the same range reported in many high-income countries. The 12-month rate of 6.66% is somewhat lower.
Cannabis risk is pattern-specific: the psychiatric signal is not evenly distributed across all cannabis exposure. Risk is highest in early-onset, frequent, high-potency use, especially when family psychosis risk, trauma exposure, or other substance use is present.3
Local context changes interpretation: cultural normalization, uneven enforcement, changing legal status, and limited treatment infrastructure can all affect whether adolescent cannabis use is treated as low-risk experimentation or a mental-health warning sign.
Cannabis was decriminalized for personal use in private settings in South Africa in 2018 (Constitutional Court ruling), and a regulatory framework continues to evolve. Adolescent use prevalences in this meta-analysis include both pre- and post-decriminalization data; whether decriminalization has shifted youth use patterns will require post-2018-only analyses.
Alcohol Is the Dominant Public-Health Concern
The 35.09% lifetime alcohol prevalence is the largest single substance-use signal in the data. Alcohol is also the substance most strongly tied to several near-term adolescent harms:
- Injury and violence exposure: intoxication raises accident risk and can increase exposure to unsafe social settings.
- Sexual risk-taking: alcohol can lower inhibition in environments where adolescents already face elevated vulnerability.
- School disruption: heavy episodic drinking can interfere with attendance, concentration, and completion.
- Later alcohol-use disorder: South Africa has one of the world’s highest per-capita alcohol-related disease burdens, and adolescent initiation feeds the upstream pipeline.4
Risk-of-harm pattern matters as much as prevalence. Heavy episodic drinking (binge drinking) carries substantially higher harm risk than equivalent-volume regular consumption. The meta-analysis pooled various drinking measures, so the ratio of any-use to harmful-use can’t be precisely estimated from the synthesized numbers.
Tobacco Trajectories and Vaping
The 25.47% tobacco prevalence reflects a substance class that has been actively targeted by South African public-health policy for decades. The interpretation now depends on which nicotine pathway is being measured:
- Combustible tobacco: tax increases, advertising restrictions, packaging changes, and public-place restrictions can reduce cigarette use.
- Vaping and e-cigarettes: nicotine exposure may persist through newer delivery systems even if cigarette smoking declines.
- Survey definitions: pooled tobacco estimates can hide whether adolescent nicotine exposure is falling or changing format.
The Brooke-Sumner synthesis covers studies through approximately 2024, capturing the early-vape transition but not necessarily the most recent dynamics. Whether tobacco/nicotine exposure is genuinely declining in South African adolescents or shifting form remains an open empirical question.
What the Heterogeneity Tells Us
The wide between-study heterogeneity is clinically informative. Substance use among South African adolescents varies sharply by local setting. Regional, socioeconomic, and demographic factors produce dramatically different exposure profiles.1
This has direct implications for prevention design. National-level interventions that ignore local context will fail in some regions and over-target others. The meta-regression approach the researchers used identifies study-level moderators, but surveillance still needs 3 practical upgrades:
- Representative sampling: school-only data miss adolescents who have dropped out or attend intermittently.
- Consistent substance definitions: alcohol, tobacco, vaping, cannabis, and polysubstance use need stable categories across surveys.
- Regional resolution: national averages should not erase provincial and community-level patterns that decide where prevention resources belong.
The authors flag this as the central policy implication. South Africa lacks a standardized adolescent substance-use surveillance system comparable to the U.S. Monitoring the Future study or European ESPAD. Building one would change what’s possible analytically and clinically.
What Effective Adolescent Prevention Looks Like
The evidence base for adolescent substance-use prevention has matured substantially. Strategies with the most defensible support are active, specific, and tied to the environment adolescents actually live in:5
- Interactive school programs: skills-based prevention works better than didactic anti-drug lecturing.
- Family-based interventions: higher-risk adolescents often need parent, caregiver, or household-level support, not classroom messaging alone.
- Environmental policy: alcohol pricing, advertising restrictions, and retailer compliance change exposure more reliably than slogans.
- Integrated mental-health care: prevention works better when depression, anxiety, ADHD, trauma, and substance use are treated as linked problems.
Weak strategies: scare-tactic education, drug-testing in schools, single-session presentations, and abstinence-only messaging do not work consistently. Prevention has to combine exposure reduction, mental-health treatment, and harm-reduction realism.
Limits of the Synthesized Evidence
The pooled estimates are useful, but the evidence has several practical limits:
- Mixed sampling frames: school surveys, household surveys, and treatment-seeking samples capture different adolescent populations.
- Inconsistent definitions: substance categories, age ranges, geographic settings, and measurement periods varied across studies.
- Self-report bias: recall and social-desirability bias likely differ by substance, survey context, and local stigma.
- Mostly cross-sectional evidence: most included studies cannot prove whether substance use caused later mental-health problems or whether earlier psychiatric risk increased substance use.
- Older-adolescent skew: mean age was 16.1, so the pooled estimates are most informative for late-secondary-school ages.
Younger adolescent prevalences are likely lower; emerging-adult prevalences (18–24) are likely higher. The numbers should be read as late-adolescent exposure estimates, not as a clean map of early initiation.
Questions About Adolescent Substance Use
How does South Africa compare internationally?
Lifetime alcohol and cannabis rates are roughly comparable to many high-income countries. The harm profile is more concerning because of comorbid risk factors and limited treatment access.
Does early use cause later substance use disorder?
Earlier age of initiation is consistently associated with higher risk of later substance use disorder. The relationship is partly causal (neurodevelopmental effects) and partly confounded (the same factors that drive early initiation drive long-term use).
What about polysubstance use?
The meta-analysis reports each substance separately, but adolescent polysubstance use is common in South African data — alcohol plus cannabis is the most frequent combination. Polysubstance patterns predict worse trajectories than single-substance use.
Are vaping/e-cigarette rates included?
Tobacco prevalence in this synthesis primarily reflects combustible tobacco; vape-specific rates were not separately pooled. South African vape use among adolescents is rising but data remain sparse.
References
- Brooke-Sumner C et al. Systematic review and meta-analysis of the prevalence of substance use among adolescents in South Africa. Drug Alcohol Rev. 2026;45:e70143. doi:10.1111/dar.70143
- Volkow ND et al. Adolescent substance use: from neuroscience to policy. NEJM. 2014;371(22):2095-2103. doi:10.1056/NEJMra1402309
- Marconi A et al. Meta-analysis of the association between the level of cannabis use and risk of psychosis. Schizophr Bull. 2016;42(5):1262-1269. doi:10.1093/schbul/sbw003
- WHO. Global status report on alcohol and health 2018. World Health Organization, Geneva. WHO record
- Foxcroft DR, Tsertsvadze A. Universal school-based prevention programs for alcohol misuse in young people. Cochrane Database Syst Rev. 2011;(5):CD009113. doi:10.1002/14651858.cd009113