People with PTSD are far more likely to also have a substance use disorder, and people with substance use disorders are far more likely to have a trauma history. The pattern has been documented for decades, but the mechanism connecting them has been less clear. The 2026 DeGrace meta-analysis brings the first quantitative answer to a specific version of the question: when something reminds a person with a trauma history of their trauma, does it directly trigger craving, or does it work through the emotional response to the reminder?
Research Highlights
- Reminders of trauma reliably trigger substance craving in people with trauma histories. A 2026 meta-analysis of 32 studies and 21 unique datasets found small-to-medium effects (Cohen’s d 0.26 to 0.53) when participants saw or heard cues tied to their traumatic experience.
- The path runs through negative emotions, not directly. When trauma reminders show up, they trigger sadness, fear, anger, or shame first; that wave of negative feeling is what then drives the craving. The meta-analysis tested this formally and confirmed negative affect mediates most of the trauma-craving link.
- This explains why PTSD and substance use disorders cluster together. Cocaine use disorder doubles the rate of PTSD; cannabis use disorder is 2.6 times more common in people with PTSD than in trauma-exposed people without PTSD; alcohol use disorder is 1.3 times more common.
- Practical implication: treatments that target the negative-affect step interrupt the chain. Skills that quiet the emotional response to trauma reminders — mindfulness, distress tolerance, exposure-based therapy — should reduce craving downstream, even without directly targeting substance use.
- Effect sizes are modest, not huge. The trauma-craving signal is reliable across studies, but the magnitude is small-to-medium. Trauma reminders explain part of relapse risk, not all of it. Other drivers (substance cues, social context, withdrawal) still matter.
What Cue Reactivity Studies Actually Measure
The basic experimental setup is the cue reactivity paradigm. Researchers expose participants to two kinds of stimuli in a controlled lab setting:
- Trauma cues. A photo, video, audio recording, or written script related to the participant’s specific traumatic experience — a car wreck for someone who survived a motor vehicle accident, a combat scene for a veteran, a recording of an aggressor’s voice for an assault survivor.
- Neutral cues. A matched stimulus with no trauma association — a photo of a toothbrush, a recording of office sounds. The neutral cue controls for the act of paying attention to a stimulus, so anything that shows up only on the trauma cue can be attributed to the trauma content.
After each cue, participants self-report their substance craving (a standardized question like “How much do you want to use [substance] right now?”) and their negative emotional state. Some studies also measure physiological responses like heart rate, skin conductance, or cortisol. The trauma vs. neutral comparison gives an experimental causal estimate, not a correlational one — the cue exposure is randomized within-person, so the difference is the cleanest available test of trauma reminders directly causing craving.
The Headline Finding: Trauma Cues Do Trigger Craving, at a Modest Magnitude
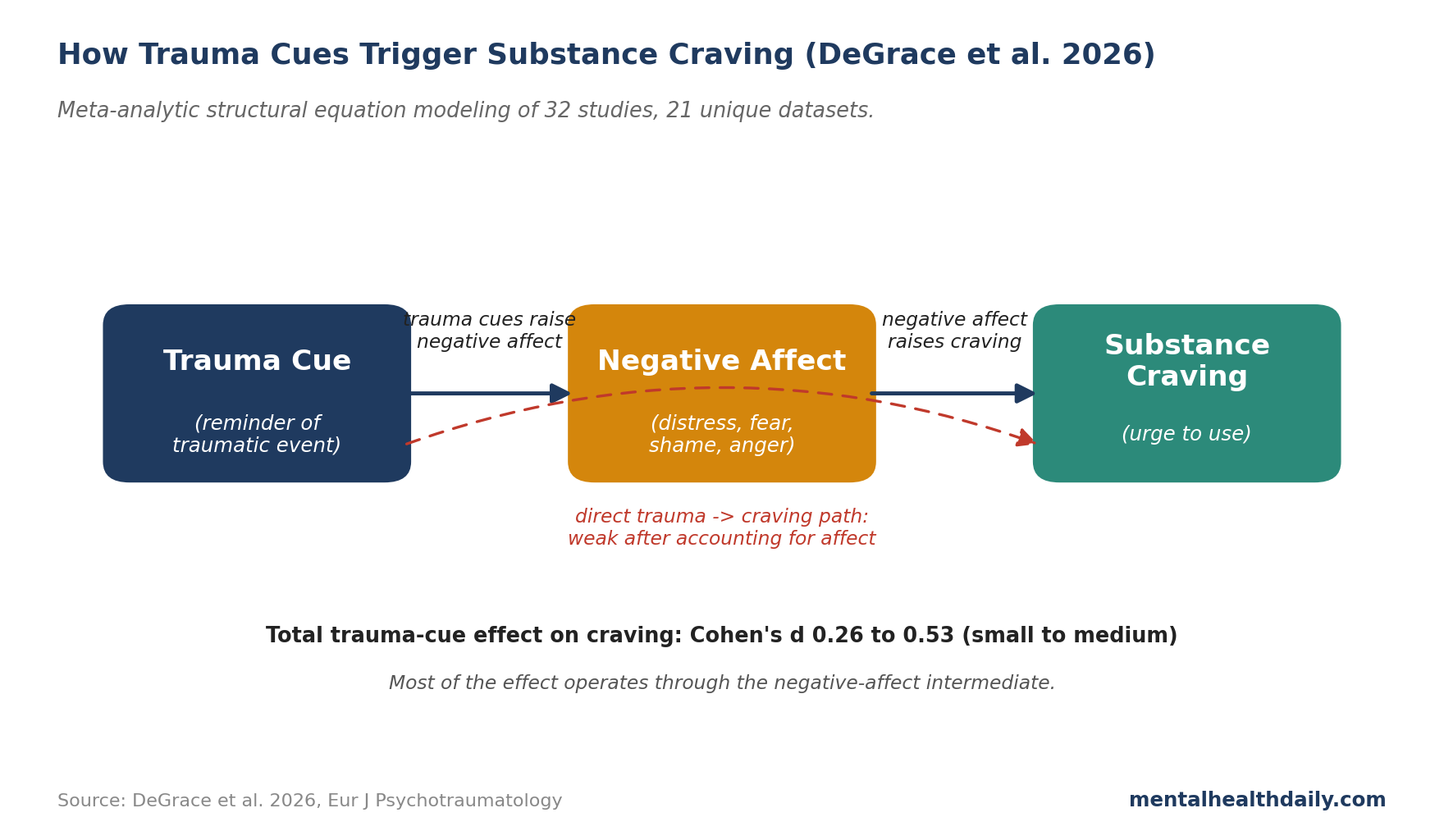
DeGrace and colleagues’ 2026 meta-analysis in the European Journal of Psychotraumatology pooled effect sizes from 32 studies covering 21 unique datasets of people with trauma histories who use substances.1 The pooled effect of trauma cues on substance craving:
- Trauma cues vs. neutral cues: Cohen’s d around 0.5 (medium effect). When the same person watched their trauma reminder versus a neutral video, craving was meaningfully higher for the trauma reminder.
- Trauma cues vs. substance cues: Cohen’s d around 0.3 (small effect, favoring trauma cues). Trauma cues trigger somewhat more craving than substance-related cues alone — meaning that for people with PTSD, a reminder of the trauma may be a stronger relapse trigger than seeing the substance itself.
- Trauma cues vs. pre-cue baseline: Cohen’s d around 0.5 (medium). Compared to the participant’s resting craving level, the trauma reminder produced a clear bump.
(Cohen’s d is a standardized effect size that lets the meta-analysis pool studies using different craving scales onto a single metric. Rough rules of thumb: d = 0.2 is small, 0.5 is medium, 0.8 is large. The trauma-cue effects sit in the small-to-medium range — reliably present, not overwhelming.)
The signal is consistent across cue type, comparator, and substance. Whether the participant uses alcohol, cannabis, cocaine, or nicotine, trauma reminders produce a bump in craving relative to neutral controls.
Why Negative Affect Mediates the Path
The more surprising finding is the mediation. DeGrace’s team ran a two-step meta-analytic structural equation model — a method that combines effect sizes from multiple studies to test whether one variable (negative affect) sits on the path between two others (trauma cue and craving). The model returned a confirmed indirect effect: most of the trauma-cue effect on craving runs through negative affect.
That structure matters for both theory and treatment. Two competing models had been on the table:
- Direct conditioning. Trauma cues become conditioned stimuli for substance craving through repeated pairing — the person uses substances after a trauma reminder, the brain learns the association, and eventually the trauma cue alone triggers craving. This would predict trauma cues directly elicit craving without an emotional intermediate.
- Negative-affect mediation. Trauma cues trigger negative emotions (the affective processing model from Baker and colleagues, 2004), and it is the negative emotion — not the cue itself — that conditionally triggers the craving response.2 This predicts the indirect path runs through affect.
The DeGrace mediation result favors the second model. Trauma reminders work by triggering distress; distress drives craving. The implication is that the relapse pathway is indirect, which gives more places to intervene.
Why PTSD and Substance Use Disorders Cluster Together
The DeGrace meta-analysis fits inside a much larger literature on PTSD-SUD comorbidity. The clustering is well-documented:
- Cocaine use disorder: people with cocaine use disorder are 2.18 times more likely to have PTSD in their lifetime than people without (Saunders et al. 2015).3
- Cannabis use disorder: people with PTSD are 2.6 times more likely to have CUD than trauma-exposed people without PTSD (Walsh et al. 2014).1 17.6% of US adults with PTSD will also be diagnosed with CUD at some point (Hasin et al. 2016).4
- Alcohol use disorder: diagnosed AUD is 1.3 times more common in people with lifetime PTSD (Grant et al. 2015), and longitudinal data show PTSD raises subsequent AUD risk specifically — the temporal direction matters.5
Two non-mutually-exclusive theoretical frameworks dominate explanations:
- The self-medication hypothesis (Khantzian 1997). Substances that acutely reduce PTSD symptoms — alcohol blunts hyperarousal, cannabis dampens flashbacks for some users, opioids quiet emotional pain — get used repeatedly to manage distress. The reinforcement cycle locks in.6
- Mutual maintenance. PTSD worsens substance use, substance use worsens PTSD, and each disorder feeds the other. Hawn and colleagues’ 2020 review synthesized this bidirectional model.7
The DeGrace meta-analysis fits both: trauma cues elicit negative affect, which drives craving, which drives use, which acutely dampens negative affect, which reinforces the next cycle. Across enough cycles, a robust conditioned link between trauma reminders and substance craving builds up — which is what the cue reactivity studies measure.
Where the Evidence Has Real Gaps
Several limitations cut across the cue reactivity literature.
Lab cues aren’t real-world cues. A 30-second video clip in a lab setting can’t fully replicate the intensity of an unexpected trauma trigger encountered in daily life. The lab effect sizes (d 0.26 to 0.53) probably underestimate the magnitude of in-the-moment relapse triggers. Ecological momentary assessment studies — tracking craving and trauma cues in real time on smartphones — would help calibrate this, but those are harder to run and pool.
Most studies are small. The 21 unique datasets have a median sample size in the low double-digits. Small samples produce noisy effect estimates and inflate apparent moderator effects. Pooled estimates are still informative, but individual study results should be read as imprecise.
Risk of bias varies. DeGrace’s team identified study quality as a significant moderator — lower-quality trials produced larger effects. The pooled effect, after weighting toward higher-quality studies, would land at the smaller end of the d 0.26 to 0.53 range.
Negative affect measurement is heterogeneous. Different studies used different scales and different sub-dimensions (general distress, anxiety, sadness, anger). The mediation finding is robust to this heterogeneity, but which specific emotion drives the most craving isn’t yet clearly identified.
The literature skews toward English-speaking, North American samples. Generalizability to other populations — particularly trauma-exposed populations in low- and middle-income settings — is limited.
What the Mediation Pathway Suggests for Treatment
If the path runs through negative affect rather than direct conditioning, treatment approaches that interrupt the affective response should reduce craving downstream. Several existing interventions fit this logic.
- Concurrent treatment of PTSD and SUD beats sequential treatment in the trial data. Programs like COPE (Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure) treat both conditions in parallel; Mills and colleagues’ 2012 JAMA trial of integrated treatment showed superior outcomes compared with substance-focused care alone.8 The rationale lines up with the mediation finding: reducing the negative-affect response to trauma cues should reduce the trauma-driven craving.
- Mindfulness-based relapse prevention has growing trial support. The mechanism is teaching people to observe negative affect without acting on it — which interrupts exactly the affect-to-craving step DeGrace identified.
- Distress tolerance skills from DBT (dialectical behavior therapy) target the same path. When the trauma reminder triggers a wave of distress, distress tolerance gives the patient something to do other than reach for the substance.
- Naltrexone-style craving medication may be more effective when paired with affect-focused therapy. Anti-craving medications target the downstream craving directly; combining them with therapy that reduces the upstream affective response could compound the benefit. This is a hypothesis the trial literature hasn’t fully tested but the mediation result motivates.
- SSRIs alone are not enough. Standard PTSD pharmacotherapy with SSRIs reduces some PTSD symptoms but has unclear effects on cue-elicited craving. Combination treatment is the more defensible approach for comorbid PTSD-SUD.
Quick Answers on Trauma Cues and Craving
If a trauma reminder triggers craving, does that mean I’ll relapse?
A craving spike from a trauma cue is a relapse risk factor, not a relapse. The effect sizes (Cohen’s d 0.26 to 0.53) describe a meaningful average bump in craving, but craving and use are separable — many people experience strong craving without acting on it. The point of treatment is to widen that gap.
Why do trauma cues make me crave the substance specifically, not something else?
Because the substance has been repeatedly paired with trauma reminders or with the negative emotions trauma reminders produce. The brain learns “when I feel this way, I use this thing to feel better.” Over time, that association becomes automatic. The DeGrace mediation result clarifies that the path is feeling-first, craving-second — the substance is cued by the negative emotion, not directly by the trauma cue.1
Does this only apply to people with diagnosed PTSD?
No. The DeGrace analysis enrolled people with trauma histories and substance use, regardless of formal PTSD diagnosis. Higher PTSD-symptom severity in the sample produced somewhat larger effects, consistent with Saladin and colleagues’ 2003 finding that PTSD severity predicts cue-elicited craving magnitude.1,9 The trauma-cue craving response shows up in trauma-exposed substance users without PTSD too.
Is one type of substance more strongly cued by trauma than another?
Theoretically, sedating substances (alcohol, cannabis, opioids) should show stronger trauma-cue craving than stimulants, because the negative-reinforcement loop is tighter when the substance directly dampens distress. The DeGrace meta-analysis found some moderation but not a clean pattern — the effect was visible across substance types.
What can I do when a trauma cue triggers craving?
Two practical strategies the literature supports: (1) Notice the negative emotion that arises before deciding what to do — mindfulness-style observation creates a gap between the emotion and the action. (2) Use a distress tolerance skill from DBT that competes with the urge to use — cold water on the face, paced breathing, brief intense exercise. These work because they target the affect-to-craving step directly.
Is concurrent or sequential treatment better for comorbid PTSD and substance use?
Concurrent. The historical view that you have to “get sober first” before treating PTSD has been contradicted by the trial data; concurrent treatment of both conditions with integrated programs like COPE produces better outcomes than treating one at a time.
References
- When trauma triggers craving: meta-analytic evidence for the mediating role of negative affect among trauma-exposed individuals who use substances. DeGrace S et al. European Journal of Psychotraumatology. 2026;17(1):2645996. doi:10.1080/20008066.2026.2645996
- Addiction motivation reformulated: an affective processing model of negative reinforcement. Baker TB et al. Psychological Review. 2004;111(1):33-51. doi:10.1037/0033-295X.111.1.33
- Posttraumatic stress disorder, alcohol use, and physical health concerns. Saunders EC et al. Journal of Behavioral Medicine. 2015;38(6):932-945. doi:10.1007/s10865-015-9648-z
- Prevalence and correlates of DSM-5 cannabis use disorder, 2012-2013. Hasin DS et al. American Journal of Psychiatry. 2016;173(6):588-599. doi:10.1176/appi.ajp.2015.15070907
- Epidemiology of DSM-5 alcohol use disorder. Grant BF et al. JAMA Psychiatry. 2015;72(8):757-766. doi:10.1001/jamapsychiatry.2015.0584
- The self-medication hypothesis of substance use disorders: a reconsideration and recent applications. Khantzian EJ. Harvard Review of Psychiatry. 1997;4(5):231-244. doi:10.3109/10673229709030550
- A systematic review of the etiology and maintenance of comorbid PTSD and substance use disorders. Hawn SE, Cusack SE, Amstadter AB. Journal of Traumatic Stress. 2020;33(5):699-708. doi:10.1002/jts.22521
- A randomized controlled trial of integrated trauma-focused therapy for comorbid PTSD and substance use disorders. Mills KL et al. JAMA. 2012;308(7):690-699. doi:10.1001/jama.2012.9071
- PTSD symptom severity is associated with increased trauma cue-elicited craving. Saladin ME et al. Addictive Behaviors. 2003;28(9):1611-1629. doi:10.1016/j.addbeh.2003.08.037