A 2026 Scientific Reports paper involving 1,205 participants found that people using GLP-1-style weight-loss medication were judged as less effortful, less moral, less competent, less warm, less deserving, and less attractive as cooperation partners after the same 20 kg weight loss described for a diet-and-exercise-only comparator.
Research Highlights
- Same weight loss, harsher judgment: Tissot et al. ran 4 preregistered vignette studies involving 1,205 participants in Belgium, the United States, and the United Kingdom.1
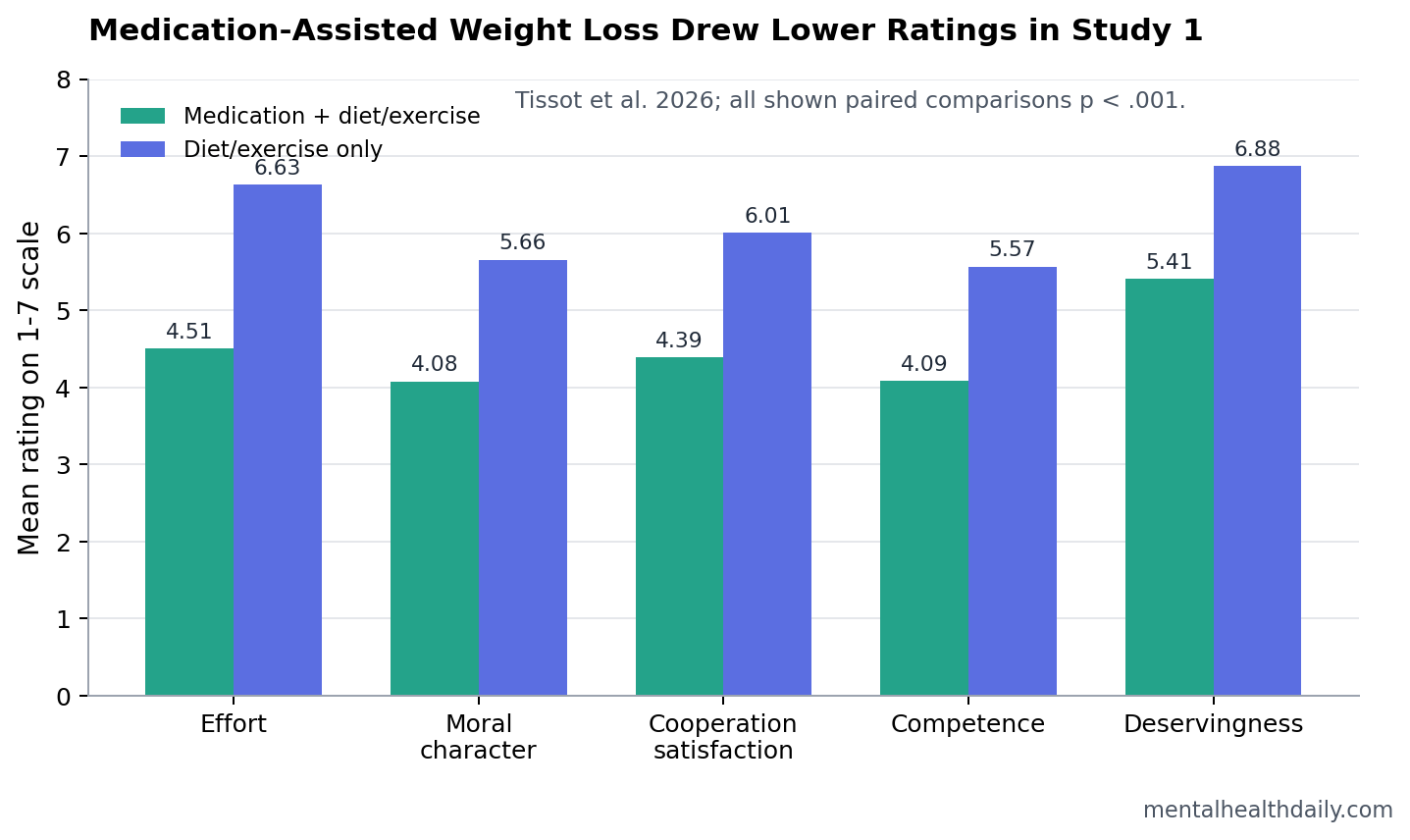
- Effort penalty was large: in Study 1, the medication-assisted target was rated lower on effort than the diet-and-exercise-only target, 4.51 vs. 6.63 on a 1-7 scale, with d = 1.31.1
- Moral judgment moved with effort: moral-character ratings were also lower for the medication-assisted target, 4.08 vs. 5.66, with d = 1.25.1
- Social penalties spread beyond morality: cooperation satisfaction, competence, warmth, and deservingness all favored the diet-and-exercise-only target, with Study 1 effect sizes from d = 0.56 to 0.96.1
- Mechanism was effort moralization: effort-difference and moral-judgment differences correlated at r = .59, .69, and .65 in Studies 2-4, matching prior work showing that observers treat effort as moral evidence.1,3
GLP-1 receptor agonists are drugs that mimic glucagon-like peptide-1, a gut hormone signal that helps regulate appetite, satiety, and blood sugar. Semaglutide and related medications are often discussed as Ozempic- or Wegovy-style weight-loss drugs, but the Tissot paper was not testing whether these drugs work; it tested how observers judge someone who used medication while also dieting and exercising.
Effort moralization means treating visible effort as evidence of moral character, even when the outcome is held constant. In this case, the social penalty did not come from a worse weight-loss result: both vignette targets lost 20 kg over 1 year, both changed diet and exercise, and both reached a body mass index (BMI) of 23.
4 Preregistered Studies Isolated Medication Use From Weight-Loss Success
Tissot et al. used a within-participant vignette design. Each participant evaluated 2 men, both described as initially overweight, equally determined, equally strict with diet and exercise, and equally successful after losing 20 kg in 1 year. One man also used anti-obesity medication that reduced hunger; the other relied only on diet and exercise changes.
Within-participant design means each participant compared both targets, so the key contrast was not between different groups of respondents. The design directly asked whether the medication detail changed judgment when the outcome and lifestyle effort described in the story were otherwise matched.
The included samples were:
- Study 1: 318 Belgian participants, 86.79% female, mean age 19.25 years.
- Study 2: 345 Belgian participants, 84.06% female, mean age 18.85 years.
- Study 3: 243 U.S. Prolific participants, 47.74% female, mean age 37.63 years.
- Study 4: 300 UK Prolific participants, 51.33% female, mean age 43.63 years.
The repeated result was straightforward: when medication entered the story, observers saw the same weight loss as less effortful and less morally impressive. Study 1 produced a large effort gap, with medication-assisted weight loss rated 4.51 vs. 6.63 for traditional-only weight loss, t(317) = 23.37, p < .001, d = 1.31.
Moral Character Ratings Fell Even When Diet and Exercise Stayed in the Story
Study 1 also found a large moral-character gap: 4.08 for the medication-assisted target vs. 5.66 for the diet-and-exercise-only target, t(317) = 22.27, p < .001, d = 1.25. The moral scale included traits such as trustworthy, honest, respectful, cooperative, dedicated, responsible, disciplined, and self-controlled.
The design makes the result sharper than ordinary “Ozempic shaming” commentary. The medication user was not described as skipping diet or exercise. The medication was added to the same lifestyle behavior and the same outcome, which means the judgment penalty attached to perceived method and effort rather than poorer adherence in the vignette.
The effort link replicated: Study 2 found that larger effort differences were associated with larger moral-judgment differences, r = .59. Study 3 found r = .69, and Study 4 found r = .65. In the across-study multilevel model, perceived-effort differences predicted moral-judgment differences with β = 0.59, 95% CI [0.50, 0.68], p < .001.
Shortcut beliefs added another layer: Study 4 found that stronger belief that anti-obesity medication was a shortcut correlated with larger moral-judgment differences, r = .52. The direction is clinically relevant because “shortcut” language can make medical treatment sound like character failure rather than one tool in chronic weight management.
Competence, Warmth, Deservingness, and Cooperation Were Penalized Too
The social penalty did not stop at abstract morality. Participants also rated the medication-assisted target lower on several downstream judgments:
- Cooperation satisfaction: 4.39 for the medication-assisted target vs. 6.01 for the traditional-only target, d = 0.95.
- Competence: 4.09 vs. 5.57, d = 0.89.
- Warmth: 4.23 vs. 4.88, d = 0.56.
- Outcome deservingness: 5.41 vs. 6.88, d = 0.96.
Those outcomes matter because stigma rarely stays in one mental box. A person judged as less disciplined may also be seen as less deserving, less competent, or less desirable to work with. In real health systems, that kind of judgment can shape social support, insurance preferences, clinician tone, workplace conversations, and whether patients disclose treatment.
Post and Persky tested a nearby GLP-1 question in women with higher and lower body weight and found that GLP-1 receptor agonist use affected social evaluation around weight loss.2 Tissot et al. added a cleaner mechanism: even when the medication user is still dieting and exercising, observers can treat reduced hunger as reduced effort, then translate that effort difference into moral and social penalties.
Effort Moralization Explains Why “Cheating” Language Sticks
Celniker et al. described effort moralization across 8 studies involving 5,502 participants: observers treated effort as morally admirable in paid work, personal fitness, and charitable fundraising, even when more effort did not produce better output.3 Berry and Lucas found a similar effort-to-character pattern for prosocial behavior, where greater effort increased perceived moral credit until observers decided that enough effort had been shown.4
That literature helps explain why GLP-1 stigma can feel intuitive even when it is logically weak. A medication that reduces hunger changes the visible hardship of weight loss. If observers treat hardship as proof of character, reducing hardship can look morally suspicious.
Calibration: effort is not irrelevant. Adhering to diet, exercise, medical visits, side-effect management, prescription access, and long-term maintenance can be difficult. The problem is turning visible suffering into the moral price of legitimacy. If a treatment works partly by lowering hunger, the lowered hunger is the mechanism, not evidence that the patient is less deserving.
Weight Stigma Can Affect Mental Health and Treatment Access
Weight stigma has been linked with anxiety, depression, social isolation, perceived stress, disordered eating, physical-activity avoidance, and lower willingness to seek medical care.5,6 A medication-specific stigma layer can add another barrier: patients may be judged for having obesity, then judged again for using a treatment that makes weight loss more achievable.
Rubino et al.’s international consensus statement framed obesity stigma as a public-health problem, not a harmless motivational tool.6 Tissot et al. sharpen that point for the GLP-1 era. Public messaging that treats medication-assisted weight loss as cheating can reward suffering as proof of virtue and penalize effective care when it reduces that suffering.
The strongest practical implication is not that every GLP-1 criticism is stigma. Cost, access, side effects, discontinuation, supply constraints, and long-term risk-benefit questions all deserve scrutiny. The stigma signal appears when the criticism shifts from evidence about treatment to moral suspicion about needing less hunger, less struggle, or more medical help.
Vignette Evidence Cannot Prove Real-World Treatment Harm
This evidence is strong for social judgment under controlled descriptions, but it does not prove real-world clinical outcomes. Vignette studies show how people respond to a written scenario; they do not measure actual prescribing, adherence, depression trajectories, insurance decisions, or patient disclosure.
Several limits keep the finding in the social-judgment lane:
- Target gender: the vignettes described male targets, so reactions to women, nonbinary people, or different body-size histories may differ.
- Sample frame: participants came from Belgium, the United States, and the United Kingdom, mostly Western samples.
- Weight history: participants’ own weight status was not measured, which may affect how they judge medication-assisted weight loss.
- Current-media timing: data were collected from November 2024 to February 2025, during intense public attention to GLP-1 drugs.
- Scenario simplification: real treatment includes dose escalation, access barriers, side effects, discontinuation, metabolic disease, psychiatric history, and clinician judgment.
Those limits do not erase the effect. They define it. Tissot et al. showed that a single medication detail can change moral and social evaluation when diet, exercise, weight-loss amount, timeline, and BMI endpoint are otherwise held constant.
Questions About GLP-1 Weight-Loss Stigma
Did this study test whether GLP-1 drugs are clinically good or bad?
No. The paper tested social judgment, not drug efficacy, safety, durability, or comparative clinical outcomes. The vignette held weight loss and lifestyle behavior constant to isolate how medication use changed observers’ ratings.
Why does effort matter so much in these judgments?
People often treat effort as a signal of discipline, commitment, and moral character. That shortcut can become unfair when it treats reduced suffering as reduced virtue, especially when the outcome is identical.
Does the finding mean people should hide GLP-1 use?
The study does not answer disclosure decisions for individual patients. It does suggest that public “cheating” narratives can create predictable social penalties, even when medication is used alongside diet and exercise.
What would reduce this kind of stigma?
Messaging should separate evidence-based criticism from character judgment. It is reasonable to discuss cost, side effects, access, and long-term maintenance; it is weaker to treat hunger reduction or medication use as proof that someone did not earn a health change.
References
- Tissot TT, Roth LHO. Anti-obesity medication use sparks effort-based sanctions and social penalties. Scientific Reports. 2026;16:13033. doi:10.1038/s41598-026-42166-y
- Post SM, Persky S. The effect of GLP-1 receptor agonist use on negative evaluations of women with higher and lower body weight. International Journal of Obesity. 2024;48(7):1019-1026. doi:10.1038/s41366-024-01516-4
- Celniker JB, Gregory A, Koo HJ, Piff PK, Ditto PH, Shariff AF. The moralization of effort. Journal of Experimental Psychology: General. 2023;152(1):60-79. doi:10.1037/xge0001259
- Berry Z, Lucas BJ. How Much Is Enough? The Relationship Between Prosocial Effort and Moral Character Judgments. Personality and Social Psychology Bulletin. 2023;49(11):1596-1611. doi:10.1177/01461672221135954
- Tomiyama AJ, Carr D, Granberg EM, et al. How and why weight stigma drives the obesity epidemic and harms health. BMC Medicine. 2018;16:123. doi:10.1186/s12916-018-1116-5
- Rubino F, Puhl RM, Cummings DE, et al. Joint international consensus statement for ending stigma of obesity. Nature Medicine. 2020;26(4):485-497. doi:10.1038/s41591-020-0803-x
- Papadopoulos S, Brennan L. Correlates of weight stigma in adults with overweight and obesity: A systematic literature review. Obesity. 2015;23(9):1743-1760. doi:10.1002/oby.21187