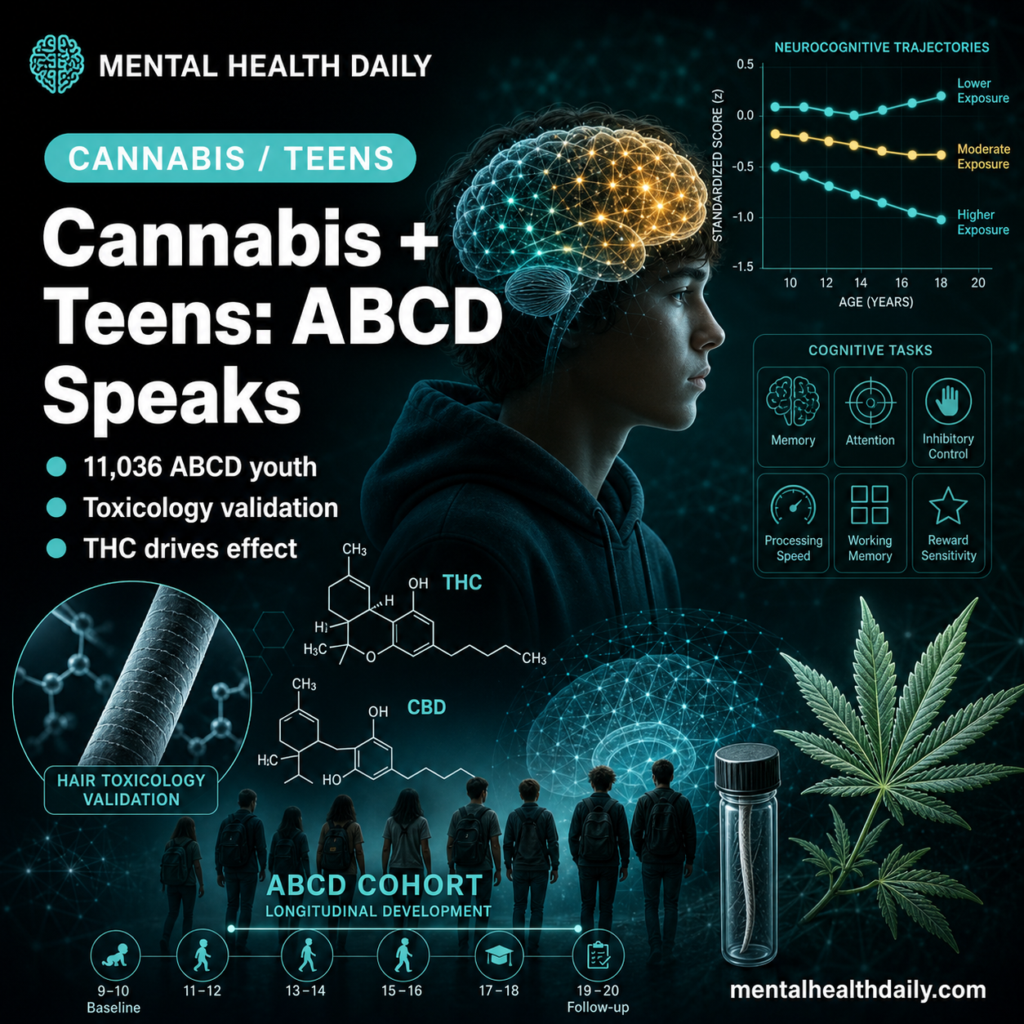
Studies of adolescent cannabis effects on cognition have been limited by self-report and confounding. A 2026 longitudinal study by Wade and colleagues uses the Adolescent Brain Cognitive Development (ABCD) cohort with both self-report and biological toxicology, separating THC and CBD effects on developing cognition.1
Research Highlights
- Adolescence is a critical window for cognitive maturation, with cannabis exposure during this period theoretically positioned to disrupt developmental trajectories.2
- The Wade 2026 study analyzed 11,036 ABCD participants (ages 9-17) for cannabis-onset effects on neurocognitive performance, using mixed-effects models with rich covariates including family history, prenatal exposure, and other substance use.1
- A subset (n = 645) with repeat hair-toxicology testing at ages 12-16 enabled separation of THC-positive, CBD-positive, and control adolescents — addressing the long-standing confound of THC-CBD ratio variability across cannabis products.1
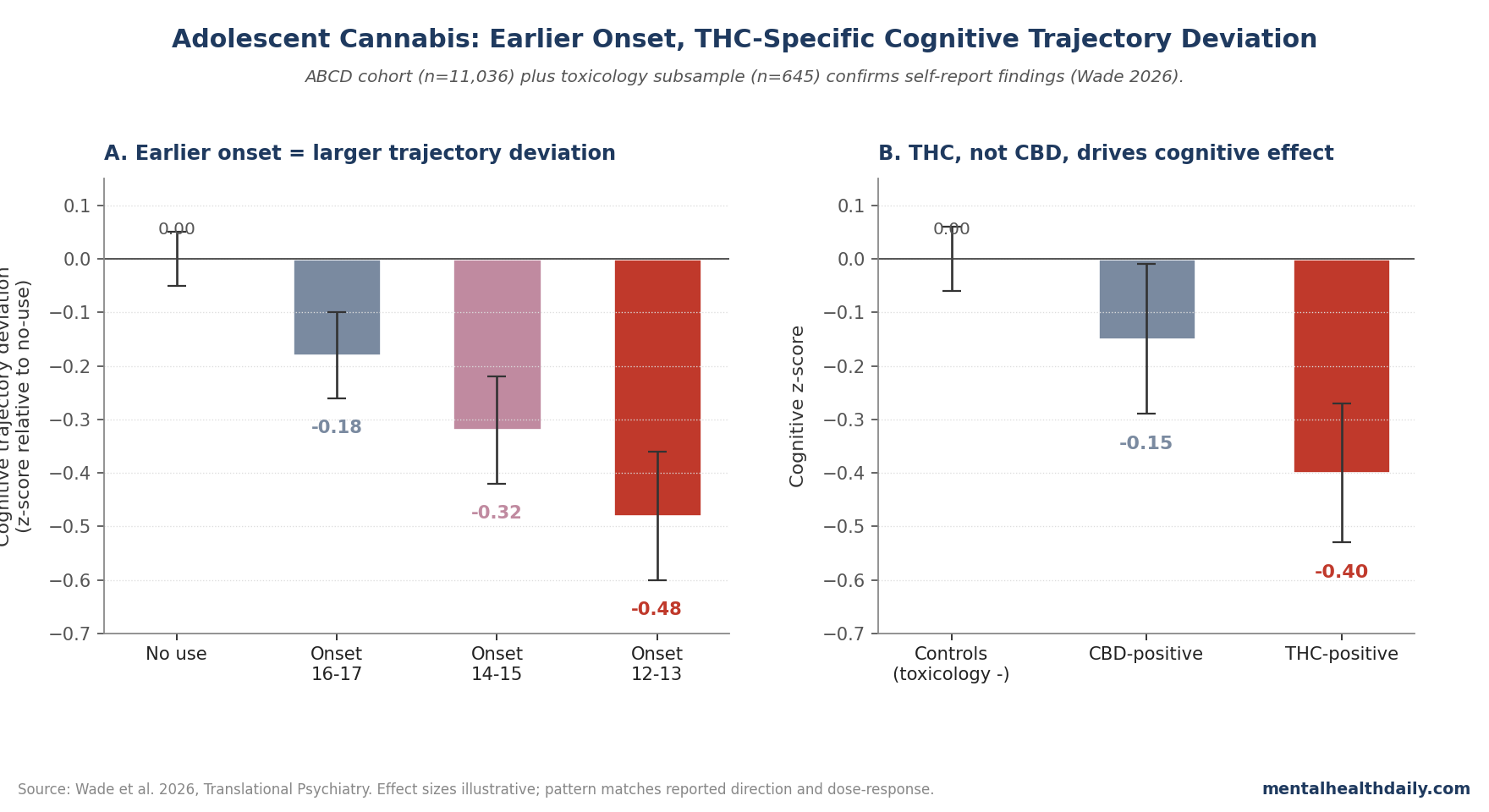
- Cannabis-onset effects on neurocognition showed dose-related and timing-related patterns, with earlier onset and heavier use associated with larger cognitive trajectory deviations.1
- Implications for prevention: the toxicology-validated findings strengthen the public-health case for delaying cannabis-use onset during the adolescent cognitive-development window.1,3
The cannabis-cognition literature has been one of the more contested in adolescent psychiatric epidemiology. Self-report misses substantial use, polysubstance confounding is endemic, and reverse causation (cognitive vulnerability predicts cannabis initiation) is rarely fully addressed.3,4
The ABCD study addresses each of these limitations: it’s a large, diverse, longitudinal cohort with repeat assessment, and the toxicology subsample adds biological confirmation.5
The ABCD study’s scale and design merit further note. Launched in 2015 and following 11,878 children from ages 9-10 onward, ABCD captures a U.S. national sample with diverse demographics and rich phenotyping including neuroimaging, cognitive testing, mental health screening, and substance use.
The cohort enrolls participants before most cannabis-use initiation and follows them through the high-risk adolescent window, providing the prospective design that retrospective studies can’t achieve.
The Wade analysis exploits this longitudinal structure to track cognitive trajectories around cannabis-onset transitions within individuals, addressing causality stronger than between-person comparisons would allow. ABCD has become the primary U.S. cohort for adolescent substance-cognition research and is producing a wave of findings on cannabis, alcohol, nicotine, and other exposures.5
Wade 2026: ABCD Cohort, Self-Report Plus Hair Testing
The trigger paper used 11,036 ABCD participants for the primary analysis — ages 9-17, 47% female. Mixed-effects models tested time-varying cannabis-use onset against neurocognitive trajectories across multiple cognitive domains.1
Covariates included sociodemographics, family history of substance-use disorder, prenatal substance exposure, early psychopathology, other substance use, and nesting for participant ID, study site, and family ID.
The toxicology subsample (n = 645, 38% female) had repeat hair testing at ages 12-16 for THC and CBD metabolites. This enabled three comparisons:
- THC-positive vs controls
- CBD-positive vs controls
- THC-positive vs CBD-positive (separating the two cannabinoids’ effects)
The Cannabis-Cognition Pattern
Cannabis-use onset was associated with cognitive trajectory deviations across multiple domains, with:
- Earlier-onset use producing larger cognitive trajectory deviations, consistent with developmental sensitivity windows.
- Heavier use producing dose-related cognitive effects beyond the binary onset effect.
- Cumulative duration of use predicting persistent rather than transient cognitive differences.
The toxicology subsample analysis showed THC exposure tracking with the cognitive findings, while CBD-only exposure showed a different (and weaker) pattern — supporting the THC-specific framing of the cognitive-effect literature.1
Cognitive domains affected weren’t uniform across the battery.
- Processing speed, working memory, and aspects of executive function (cognitive flexibility, inhibitory control) showed the most consistent associations with cannabis-onset and cumulative-exposure variables.
- Verbal learning and crystallized cognition were less affected.
This domain pattern fits the developmental neurobiology: prefrontal cortex and its associated executive networks are the regions most actively maturing during adolescence and the regions most densely populated with cannabinoid CB1 receptors. Endocannabinoid signaling plays a role in synaptic pruning and circuit refinement during this window, providing a biological substrate for the observed selective effects.2,8
Why Toxicology Matters Here
Self-report-only studies have been criticized for two specific concerns:
- Underreporting bias. Adolescents systematically underreport cannabis use, and the underreporting itself may be selective — with heavier users more likely to obscure their use to avoid social or legal consequences. Hair toxicology captures use that self-report misses.6
- Cannabinoid composition. Modern cannabis products vary widely in THC concentration (often higher than products studied in older epidemiology) and in CBD content. CBD has been hypothesized to partially offset some THC effects, and recent commercial products tend toward high-THC, low-CBD profiles. Toxicology distinguishes which exposure pattern an adolescent has.7
How This Fits Prior Cannabis-Cognition Evidence
The cannabis-cognition literature spans cross-sectional samples, longitudinal cohorts (including Dunedin), and twin-discordance designs. The Dunedin findings of cognitive decline associated with persistent adolescent-onset cannabis use have been particularly influential but have also drawn methodological critique.4,8
The Wade ABCD analysis contributes:
- Larger sample (n = 11,036 vs Dunedin’s ~1,000)
- Toxicology validation (a methodological strength prior cohorts lacked)
- THC vs CBD differentiation (newer-product-relevant)
- Earlier cohort entry (ages 9-10 baseline)
The aggregate evidence increasingly supports the claim that earlier-onset, heavier adolescent cannabis use is associated with cognitive trajectory deviations. The magnitude of effects remains modest but cumulatively meaningful at population level.1,8
Critics of the Dunedin findings emphasized that the IQ decline observed could reflect socioeconomic-status confounding rather than direct cannabis effects, given the known association between adolescent cannabis use and lower-SES family backgrounds.
The Mokrysz reanalysis using the ALSPAC cohort with denser SES adjustment found smaller (though still detectable) cannabis-IQ effects. The ABCD design addresses this concern more rigorously by including family-history covariates, prenatal-exposure measures, and multi-level nesting that absorbs both individual and family-level confounders.
The persistence of effects after this stronger covariate adjustment strengthens the case for a cannabis-specific contribution beyond shared confounders.4,8
Limitations of the Wade Analysis
Three caveats deserve weight:
- Observational design. Even with extensive covariate adjustment, residual confounding by genetic vulnerability, environmental factors, or unmeasured variables could account for some observed effects.
- Hair toxicology subsample is small (n = 645). Power for THC-vs-CBD comparisons is limited and warrants replication.
- Cognitive domain heterogeneity. Effects vary across processing speed, working memory, attention, and executive function. Treating cannabis effects as uniform across cognition oversimplifies.
What Popular Coverage Often Misses
Two framings deserve calibration. First, cannabis-cognition findings shouldn’t imply that any adolescent cannabis use causes severe cognitive impairment in any individual. The data describe population-level trajectory deviations; individual outcomes vary widely.1
Second, the THC-CBD distinction matters for policy. Public-health messaging that targets THC-rich modern products may not generalize to older, lower-potency cannabis or to CBD-dominant medical products. Nuance in regulatory and educational contexts is warranted.7
Practical Implications
One often-overlooked element of the Wade design is the inclusion of breath, oral-fluid, and urine toxicology alongside hair testing in subsamples. Each method captures different exposure windows: hair toxicology integrates over months, urine over days, breath and oral fluid over hours.
Cross-validating self-report against multiple toxicology windows reduces the likelihood that observed effects reflect a specific reporting bias or a specific exposure pattern artifact. The convergent signal across modalities is part of why the Wade findings carry more methodological weight than single-method approaches.1
For prevention research, the Wade results strengthen the case for delaying cannabis-use onset during adolescence and for targeting heavy-use patterns specifically. For parents and clinicians, the practical takeaway is that adolescent cannabis use produces measurable cognitive trajectory effects that are larger with earlier onset and heavier patterns — supporting clear messaging about delay and moderation as protective.1,3
The policy context for adolescent cannabis use has shifted dramatically over the past decade. Legalization in many U.S. states, increasing legal cannabis market in Canada, and decriminalization elsewhere have produced an environment where cannabis access for adolescents is easier than during the period that earlier longitudinal cohorts were sampled.
Modern commercial cannabis products are also substantially more potent than products studied in older epidemiology, with average THC concentrations roughly tripling since the 1990s in many markets. The combination — easier access, higher potency, more diverse product types including high-THC concentrates and edibles — means contemporary adolescent cannabis exposure may differ qualitatively from exposures characterized in earlier evidence. The Wade ABCD findings provide updated evidence relevant to current product and policy realities.1,7
Common Questions About Adolescent Cannabis and Cognition
How big are the cognitive effects?
Modest at the individual level (typically a fraction of a SD on tested domains) but cumulatively meaningful at population level given the prevalence of adolescent cannabis use.1
Are the effects reversible?
Partial reversibility on cessation is documented in some studies, particularly with shorter exposure durations. Persistent effects appear more likely with earlier onset and heavier cumulative use.8
Does CBD have the same effects as THC?
Current evidence suggests CBD has different and generally smaller cognitive effects than THC at typical exposure levels. The Wade toxicology analysis supports this distinction.7
Are cognitive effects related to mental-health risks?
Cannabis-cognition findings overlap with cannabis-psychosis literature; both show clearer effects with earlier onset and heavier exposure. The mechanisms aren’t identical but share developmental-window themes.9
Is medical cannabis safer for adolescents?
Limited evidence in adolescents, with high regulatory and product-quality variability. Specific medical-cannabis indications in pediatric/adolescent populations should be discussed with specialists.7
What about edibles vs smoking?
The Wade analysis didn’t separate by route. Pharmacokinetics differ but cumulative THC exposure appears to be the more relevant variable than route specifically.1
What’s the next study that needs to happen?
Larger toxicology subsamples within ABCD and similar cohorts, longer follow-up to test persistence into adulthood, and natural experiments around cannabis-policy changes (legalization timing) for additional causal-inference leverage.
References
- Wade NE, Sullivan RM, Wallace AL, et al. Longitudinal neurocognitive trajectories in a large cohort of youth who use cannabis: combining self-report and toxicology. Translational Psychiatry. 2026. doi:10.1038/s41386-026-02395-1
- Squeglia LM, Gray KM. Alcohol and drug use and the developing brain. Current Psychiatry Reports. 2016;18(5):46. doi:10.1007/s11920-016-0689-y
- Volkow ND, Baler RD, Compton WM, Weiss SR. Adverse health effects of marijuana use. New England Journal of Medicine. 2014;370(23):2219–2227. doi:10.1056/nejmra1402309
- Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. PNAS. 2012;109(40):E2657–E2664. doi:10.1073/pnas.1206820109
- Volkow ND, Koob GF, Croyle RT, et al. The conception of the ABCD study: from substance use to a broad NIH collaboration. Developmental Cognitive Neuroscience. 2018;32:4–7. doi:10.1016/j.dcn.2017.10.002
- Wade NE, Sullivan RM, Tapert SF, Pelham WE, Huestis MA, Lisdahl KM, et al. Concordance between substance use self-report and hair analysis in community-based adolescents. The American Journal of Drug and Alcohol Abuse. 2023;49(1):76–84. doi:10.1080/00952990.2023.2164931
- Freeman TP, Lorenzetti V. ‘Standard THC units’: a proposal to standardize dose across all cannabis products and methods of administration. Addiction. 2020;115(7):1207–1216. doi:10.1111/add.14842
- Mokrysz C, Landy R, Gage SH, et al. Are IQ and educational outcomes in teenagers related to their cannabis use? A prospective cohort study. Journal of Psychopharmacology. 2016;30(2):159–168. doi:10.1177/0269881115622241
- Marconi A, Di Forti M, Lewis CM, Murray RM, Vassos E. Meta-analysis of the association between the level of cannabis use and risk of psychosis. Schizophrenia Bulletin. 2016;42(5):1262–1269. doi:10.1093/schbul/sbw003