A 2026 meta-analysis of 34 studies involving 13,107 participants found that body dysmorphic disorder symptoms and perfectionism were moderately correlated: r = .32, 95% CI 0.28 to 0.36, p < .001. The result supports perfectionism as a useful clinical clue in body dysmorphic disorder, but the estimate dropped to r = .09 after depression adjustment in the 5 studies that reported enough data for that test.
Research Highlights
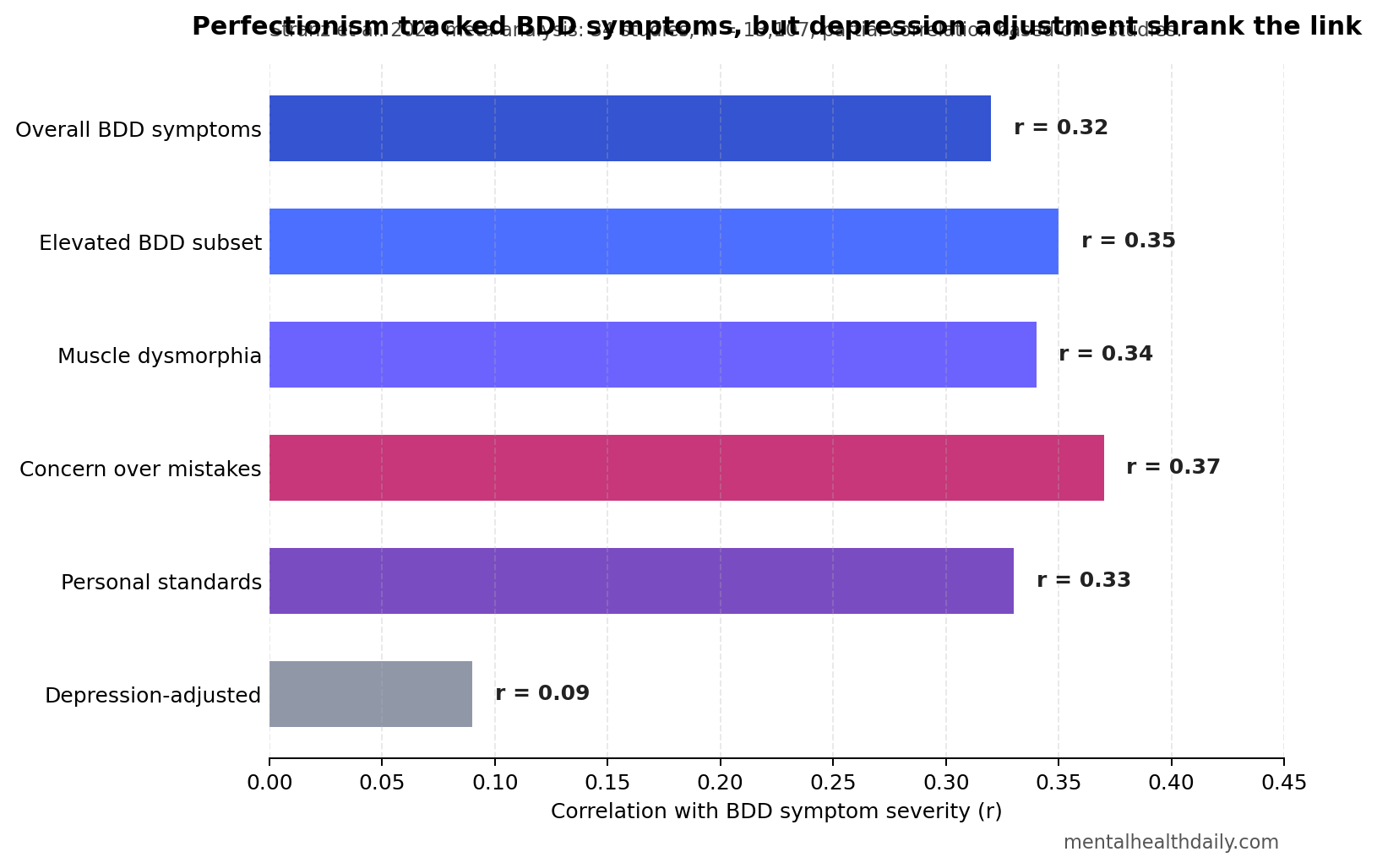
- Moderate headline link: Across 34 studies and 13,107 participants, body dysmorphic disorder symptoms correlated with perfectionism at r = .32, 95% CI 0.28 to 0.36.
- Depression changed the estimate: In the 5 studies that allowed depression adjustment, the partial correlation fell to r = .09, 95% CI 0.02 to 0.16.
- Concern and standards both counted: Concern over mistakes correlated at r = .37, personal standards at r = .33, and doubts about actions at r = .19.
- Muscle dysmorphia looked similar: Studies focused on muscle dysmorphia showed r = .34, close to r = .31 for broader body dysmorphic symptoms.
- Causality remains unresolved: Heterogeneity was high at I² = 81%, Egger’s test suggested small-study effects, and every included study was cross-sectional.
Body dysmorphic disorder (BDD) means persistent preoccupation with a perceived defect in appearance that looks minor or invisible to others, paired with repetitive behaviors such as mirror checking, grooming, comparing, camouflaging, or reassurance seeking. Perfectionism means rigid standards and harsh self-evaluation; in BDD, those standards often attach to appearance, symmetry, muscularity, skin, hair, facial features, or body shape.
The 2026 Stranz et al. meta-analysis matters because BDD theory has long treated perfectionism as part of the clinical picture, but the field lacked a pooled estimate for the association. The new synthesis says the relationship is real enough to assess, but not clean enough to treat as a single causal mechanism.
BDD Symptoms and Perfectionism Correlated at r = .32 Across 34 Studies
Stranz et al. pooled zero-order correlations from 34 studies published between 2002 and 2025. A zero-order correlation is the raw association between 2 variables before adjusting for another variable such as depression, obsessive-compulsive symptoms, or eating-disorder symptoms.
The pooled association was moderate: r = .32, 95% CI 0.28 to 0.36, p < .001. In plain terms, people with more severe BDD symptoms also tended to score higher on perfectionism, but the correlation was not so large that perfectionism can stand in for BDD severity.
Evidence base: 19 studies included participants meeting full diagnostic or probable BDD criteria, 15 studies involved subclinical symptoms or elevated body dissatisfaction, and 9 studies focused on muscle dysmorphia. Participants averaged about 25 years old, and approximately 55% were women.
Measurement spread: BDD symptoms were usually measured by self-report rather than clinician interview. Perfectionism instruments varied too, including the Frost Multidimensional Perfectionism Scale, Multidimensional Perfectionism Scale, Eating Disorder Inventory perfectionism subscale, and perfectionistic self-presentation measures.
That measurement spread helps explain why the headline estimate should be read as a robust association, not a precise biological constant. The meta-analysis reported high heterogeneity, I² = 81%, meaning the studies varied far more than sampling error alone would predict.
Concern Over Mistakes Was the Strongest Perfectionism Facet
Perfectionism is not one thing. The Stranz analysis separated available Frost-scale facets where enough subscale data existed. Concern over mistakes showed the largest association with BDD symptom severity: r = .37, p < .001.
Concern over mistakes captures the self-critical part of perfectionism: errors feel threatening, small deviations feel unacceptable, and personal worth becomes tied to avoiding visible flaws. In BDD, that maps onto appearance monitoring, repeated checking, and distress over features that other people may barely notice.
Personal standards also showed a substantial association, r = .33, p < .001. That facet reflects high internal standards, which can become appearance rules: skin has to look exact, muscularity has to meet a fixed ideal, or facial symmetry has to feel “right” before the person can leave the house.
Doubts about actions was smaller but still significant at r = .19, p = .023. That facet fits the repetitive uncertainty loop: the person checks, compares, adjusts, or seeks reassurance, then doubts whether the action was enough.
Depression Adjustment Cut the Correlation to r = .09
The most important calibration in the 2026 paper is the depression-adjusted result. Only 5 studies reported enough intercorrelation data to calculate partial correlations, but in those studies the association between BDD symptoms and perfectionism shrank from the moderate range to r = .09, 95% CI 0.02 to 0.16, p = .011.
Partial correlation means the analysis estimates the BDD-perfectionism link after statistically accounting for depressive symptoms. The drop does not erase perfectionism from BDD formulation. It says that part of the raw association probably reflects shared negative affect, self-criticism, shame, and perceived failure rather than an appearance-specific mechanism.
Older transdiagnostic work fits this calibration. Egan et al. reviewed perfectionism as a process that cuts across depression, anxiety, obsessive-compulsive disorder, eating disorders, and related conditions.
Pinto et al. made a similar clinical point for obsessive-compulsive and related disorders: perfectionism may be relevant in treatment planning, but it should be mapped to the patient’s actual maintaining loop rather than treated as a generic target.
For BDD, the practical interpretation is narrower and more useful: assess perfectionistic standards when they organize the appearance rituals, but do not assume the standards are BDD-specific unless the history and symptom chain show that.
Muscle Dysmorphia Fit the Same Pattern
Muscle dysmorphia is a BDD-related presentation centered on the belief that one’s body is insufficiently muscular or lean, often paired with checking, comparison, rigid diet or training rules, and distress about size or definition. In the Stranz meta-analysis, studies focused on muscle dysmorphia showed a pooled association of r = .34, 95% CI 0.29 to 0.39.
That estimate was close to the broader BDD-symptom subgroup, r = .31, 95% CI 0.26 to 0.36. Formal subgroup tests did not show significant differences by diagnostic subtype, age group, gender, or clinical status.
The content can still differ. In muscle dysmorphia, perfectionistic standards may focus on size, leanness, symmetry, strength, and training discipline. In other BDD presentations, standards may focus on skin, hair, facial shape, body proportions, or perceived asymmetry. The pooled result says perfectionistic self-evaluation travels across appearance concerns; it does not say every presentation has the same trigger or ritual chain.
Cross-Sectional Evidence Cannot Prove Perfectionism Causes BDD
All included studies were cross-sectional. Cross-sectional means symptoms and traits were measured at roughly the same time, so the analysis cannot decide whether perfectionism came first, BDD symptoms increased perfectionistic checking, or both reflected a broader vulnerability.
Risk-of-bias ratings also argue for restraint. Of the 34 studies, only 3 were rated low risk of bias, 14 were moderate, and 17 were high. Many studies relied on convenience samples and self-report scales, which can inflate correlations when the same person reports both appearance distress and self-critical perfectionism.
Publication bias is another warning. Funnel plot inspection suggested asymmetry, and Egger’s regression found significant small-study effects: bias estimate = 2.08, SE = 0.76, p = .010. Smaller studies tended to report larger associations, so the pooled r = .32 may be an upper-bound estimate.
Still, the signal did not disappear. Leave-one-out analyses kept the main estimate in the same direction and magnitude, and a secondary analysis restricted to 7 studies involving elevated body image-related distress found r = .35, 95% CI 0.22 to 0.47, p < .001. The evidence is imperfect, but it is not random noise.
Clinical Use: Assess the Standard, the Ritual, and the Comorbidity
Perfectionism is most useful in BDD when it explains what keeps the symptom loop running. A clinician, patient, or family member can ask 3 concrete questions:
- What standard is being enforced? Examples include “no visible acne,” “perfect symmetry,” “no sign of thinning hair,” or “muscles must look defined enough from every angle.”
- What ritual follows the standard? Checking, grooming, reassurance seeking, comparing, photo review, avoidance, makeup, clothing changes, cosmetic consultation, or compulsive exercise may all serve the standard.
- What else is driving self-criticism? Depression, obsessive-compulsive symptoms, eating-disorder symptoms, trauma, social anxiety, or shame can strengthen the same perfectionistic language.
Cognitive-behavioral therapy for BDD already targets distorted appearance beliefs, checking, avoidance, reassurance, and safety behaviors. Harrison et al. found that CBT reduced BDD symptoms in randomized trials, but the Stranz meta-analysis did not test whether directly treating perfectionism reduces BDD. That question still needs longitudinal and intervention evidence.
Self-compassion and shame-focused approaches are also plausible adjuncts. Linde et al. tested an acceptance and compassion-based therapy targeting shame in BDD using a multiple-baseline design, and Stranz et al. highlighted adolescent evidence linking higher self-compassion with lower BDD symptoms. Those findings are not enough to replace CBT, but they fit the same clinical logic: harsh self-evaluation may be a treatment-relevant process when it fuels appearance rituals.
Questions About BDD and Perfectionism
Does this mean perfectionism causes body dysmorphic disorder?
No. The 2026 meta-analysis found a cross-sectional association, not a causal sequence. Perfectionism may precede symptoms in some people, follow BDD-related distress in others, or reflect shared depression, shame, and obsessive-compulsive traits.
Is perfectionism specific to BDD?
Probably not. The depression-adjusted estimate fell to r = .09 in the 5 studies with enough data, and broader reviews describe perfectionism as transdiagnostic. The BDD-specific issue is how perfectionistic standards attach to perceived appearance defects and rituals.
Should treatment target perfectionism?
Sometimes. If perfectionistic rules are driving mirror checking, comparison, avoidance, cosmetic reassurance, or compulsive exercise, they belong in formulation. Current evidence is stronger for CBT for BDD than for perfectionism-only treatment in BDD.
How should the r = .32 estimate be read?
It is a moderate association. BDD severity and perfectionism tend to rise together across studies; the correlation is too limited to explain most BDD symptoms or diagnose BDD.
Bottom Line
The 2026 meta-analysis gives BDD clinicians and readers a useful number: perfectionism and BDD symptoms correlate at about r = .32 across 34 studies. The sharper interpretation is not “perfectionism causes BDD.” It is that rigid standards, concern over mistakes, and harsh self-evaluation often travel with BDD symptoms, while depression and other transdiagnostic problems explain part of the overlap.
Perfectionism should be assessed when BDD symptoms revolve around impossible appearance rules. The next evidence step is longitudinal and treatment research that tests whether changing those rules changes BDD symptoms beyond questionnaire-level co-movement.
References
- Stranz R, Maas genannt Bermpohl F, Bosbach K, Grocholewski A, Martin A, Hartmann AS. The cross-sectional relationship between body dysmorphic disorder and perfectionism: a meta-analysis. BMC Psychiatry. 2026;26:338. https://doi.org/10.1186/s12888-026-08044-7
- Egan SJ, Wade TD, Shafran R. Perfectionism as a transdiagnostic process: a clinical review. Clinical Psychology Review. 2010;31(2):203-212. https://doi.org/10.1016/j.cpr.2010.04.009
- Krebs G, Quinn R, Jassi A. Is perfectionism a risk factor for adolescent body dysmorphic symptoms? Evidence for a prospective association. Journal of Obsessive-Compulsive and Related Disorders. 2019;22:100445. https://doi.org/10.1016/j.jocrd.2019.100445
- Kuck N, Cafitz L, Burkner PC, Hoppen L, Wilhelm S, Buhlmann U. Body dysmorphic disorder and self-esteem: a meta-analysis. BMC Psychiatry. 2021;21:310. https://doi.org/10.1186/s12888-021-03185-3
- Harrison A, Fernandez de la Cruz L, Enander J, Radua J, Mataix-Cols D. Cognitive-behavioral therapy for body dysmorphic disorder: a systematic review and meta-analysis of randomized controlled trials. Clinical Psychology Review. 2016;48:43-51. https://doi.org/10.1016/j.cpr.2016.05.007
- Linde J, Luoma JB, Ruck C, Ramnero J, Lundgren T. Acceptance and compassion-based therapy targeting shame in body dysmorphic disorder: a multiple baseline study. Behavior Modification. 2023;47(3):693-718. https://doi.org/10.1177/01454455221129989
- Angelakis I, Gooding PA, Panagioti M. Suicidality in body dysmorphic disorder: a systematic review with meta-analysis. Clinical Psychology Review. 2016;49:55-66. https://doi.org/10.1016/j.cpr.2016.08.002
- Pinto A, Dargani N, Wheaton MG, Cervoni C, Rees CS, Egan SJ. Perfectionism in obsessive-compulsive disorder and related disorders: what should treating clinicians know? Journal of Obsessive-Compulsive and Related Disorders. 2017;12:102-108. https://doi.org/10.1016/j.jocrd.2017.01.001