
A 2026 Neurological Sciences brief communication added 2 Tourette syndrome cases of aripiprazole-related oculogyric crisis — sustained, involuntary upward eye deviation from extraocular-muscle dystonia — after titration to 20 mg and 30 mg daily, with remission after dose reduction.1
Research Highlights
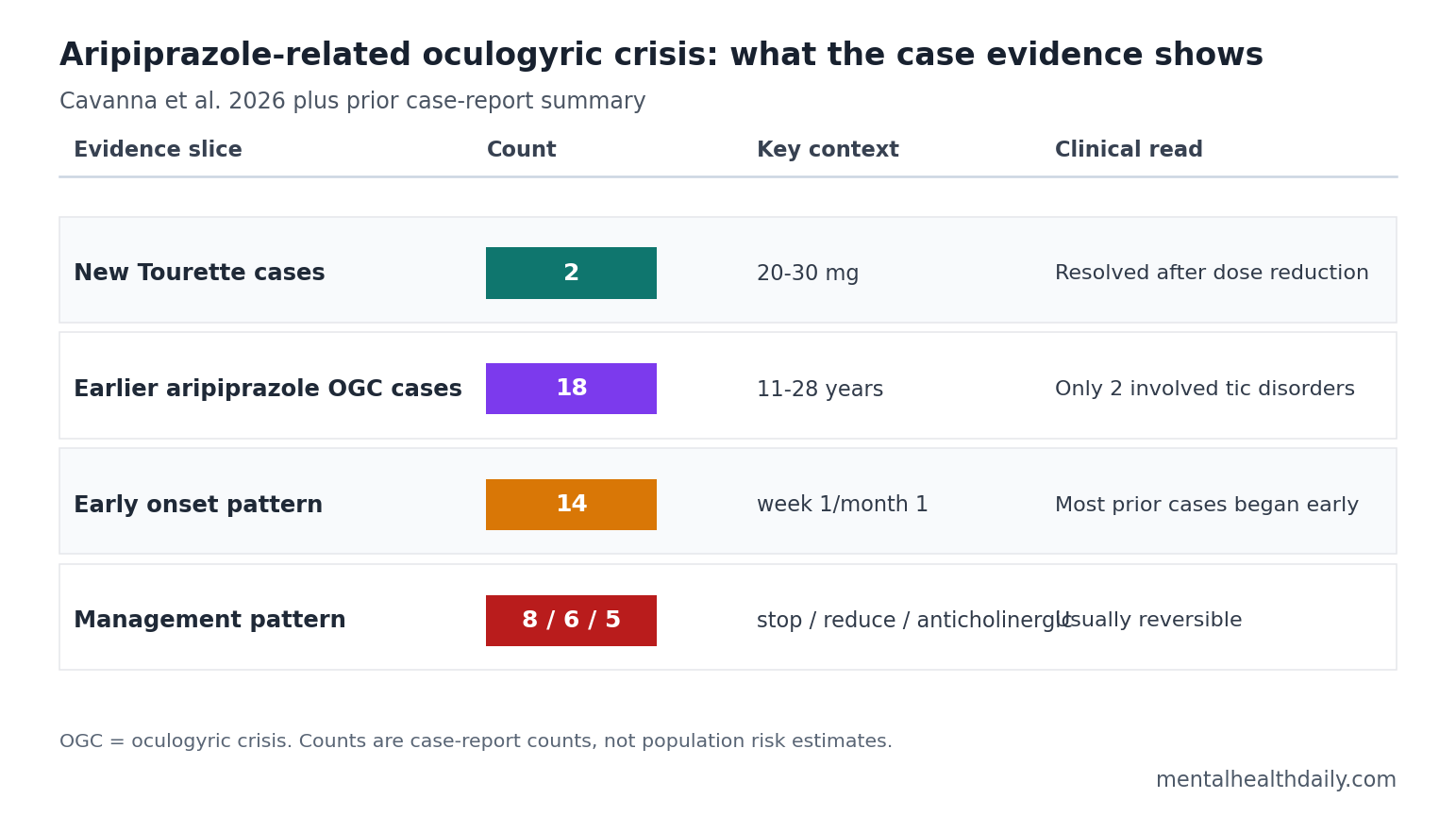
- 2 new Tourette cases: Cavanna et al. reported oculogyric crisis in females aged 16 and 22 years taking aripiprazole for chronic motor and vocal tics.1
- Dose timing was the practical clue: episodes began 2 weeks after reaching 20 mg daily in 1 patient and 3 days after reaching 30 mg daily in the other.1
- Prior reports were rare but patterned: the paper identified 18 earlier aripiprazole-related oculogyric crisis cases, including 9 females and an age range of 11–28 years.1
- Tic treatment was underrepresented: only 2 of the 18 earlier cases involved tic disorders, so the 2026 report roughly doubled the tic-indication case count.1,3
- Management was usually reversible: prior reports resolved with discontinuation in 8 cases, dose reduction in 6, and anticholinergic coadministration in 5; only 1 high-dose case persisted.1
Aripiprazole is a dopamine D2/D3 partial agonist often used when clinicians want antipsychotic or anti-tic effects with less prolactin elevation and less metabolic burden than many older dopamine blockers. That pharmacology does not remove dystonia risk. A partial dopamine agonist still changes striatal dopamine signaling, and aripiprazole has little anticholinergic activity to buffer acute motor reactions.1,2
The clinical issue is recognition. A patient with Tourette syndrome already has repetitive eye, face, neck, and body movements, so an adverse drug reaction can be mistaken for a new tic unless the pattern is separated carefully: sustained eye deviation, no premonitory urge, spasmodic extraocular-muscle contraction, and a tight relationship to recent aripiprazole titration.
20 mg and 30 mg Aripiprazole Preceded the New Tourette Cases
Cavanna et al. described 2 patients treated at a specialist Tourette syndrome clinic. Both had chronic motor and vocal tics, tic-related obsessive-compulsive symptoms, and no prior exposure to other antipsychotics or dopamine-blocking agents.1
Case 1: a 16-year-old female had marked tic severity, scoring 100% on the Tourette Syndrome Diagnostic Confidence Index and 80% on the Yale Global Tic Severity Scale. Aripiprazole was increased from 10 mg daily in 5 mg steps every 2 weeks until it reached 20 mg daily.
Two weeks after reaching 20 mg, she developed upward eye-rolling episodes lasting about 15 minutes. Reducing aripiprazole back to 10 mg daily resolved the episodes.1
Case 2: a 22-year-old female had moderate tic severity, scoring 73% on the diagnostic confidence index and 51% on the Yale scale. Aripiprazole was started at 5 mg daily and increased by 5 mg every 2 weeks to 30 mg daily.
Three days after reaching 30 mg, she developed weekly eye-rolling episodes lasting up to 30 minutes. Procyclidine, an anticholinergic drug used to treat dystonic reactions, did not stop the episodes at doses up to 20 mg daily; reducing aripiprazole to 15 mg daily did.1
Both cases point toward dose-sensitive vulnerability rather than a vague intolerance label. The adverse event appeared shortly after the target dose, the eye movements differed from baseline tics, and symptoms remitted after dose reduction rather than after a long washout or diagnostic detour.
Oculogyric Crisis Means Sustained Eye-Muscle Dystonia
Acute dystonia means involuntary, sustained muscle contraction that can twist the eyes, neck, jaw, tongue, trunk, or limbs into abnormal postures. In oculogyric crisis, the dominant contraction involves the extraocular muscles, classically producing forced upward gaze.
That distinction matters operationally because Tourette tics and oculogyric crisis can both involve the eyes. Cavanna et al. separated the events by phenomenology:
- No premonitory urge: the eye-rolling spells lacked the rising inner sensation that often precedes tics.
- Sustained tonic contraction: episodes lasted 15–30 minutes rather than appearing as brief tic bursts.
- Medication timing: both patients developed the spells shortly after reaching medium/high aripiprazole doses.
- Reversibility with dose reduction: symptoms resolved when aripiprazole exposure was lowered.
For readers taking or monitoring aripiprazole, the relevant question is not whether every unusual eye movement is dangerous. The signal is a new sustained eye-deviation episode after dose escalation, especially when it feels different from the person’s usual tics and lacks the ordinary tic urge-release cycle.
18 Earlier Cases Put the 2026 Report in Context
The 2026 report summarized 18 prior aripiprazole-related oculogyric crisis cases. Half were female, ages ranged from 11 to 28 years, and only 2 earlier cases involved tic disorders. The other indications were psychosis in 5 cases, affective disorders in 4, obsessive-compulsive disorder in 3, autism-spectrum-related challenging behaviors in 2, attention-deficit/hyperactivity disorder in 1, and borderline personality disorder in 1.1
Timing also clustered early. Among the prior cases, 8 developed oculogyric crisis within the first week of aripiprazole treatment and 6 within the first month, across a dose range of 2.5–40 mg daily. That pattern fits an acute dystonic adverse event more than a slowly emerging tic phenotype.
Resolution pattern: 8 cases resolved after aripiprazole discontinuation, 6 after dose reduction, and 5 after adding an anticholinergic drug. The count exceeds 18 because management strategies can overlap across reports. Only 1 earlier case — a 23-year-old female receiving 30 mg daily for obsessive-compulsive disorder — was described as not fully reversible in the summary.1
Earlier individual reports support the same adverse-event direction. Fountoulakis et al. reported acute dystonia with low-dose aripiprazole in Tourette’s disorder, making tic treatment part of the signal years before the 2026 report.3 Lim et al. described dystonic symptoms associated with aripiprazole treatment, and Bhachech reported aripiprazole-induced oculogyric crisis as an acute dystonic reaction.4,5
FAERS Data Flagged Aripiprazole Ocular Adverse Events
Case reports are useful for recognizing a rare clinical pattern, but they cannot estimate incidence because there is no denominator: the reader sees the people who had the event, not the much larger number who took the drug without it. Mu and Chen added a different kind of evidence by analyzing Food and Drug Administration Adverse Event Reporting System reports from 2016 to 2022.2
FAERS is a spontaneous adverse-event reporting database. It can detect disproportionality signals — events reported more often than expected for a drug — but it cannot prove causality, rule out confounding, or calculate true population risk. In that real-world signal analysis, olanzapine had the highest signal intensity for oculogyric crisis, while aripiprazole had the highest signal strength for overall ocular adverse reactions and blepharospasm.1,2
That database pattern fits the case-report logic without overstating it. Aripiprazole is not uniquely dangerous for oculogyric crisis across every antipsychotic comparison, but its ocular-adverse-event signal is strong enough that new sustained eye deviation after titration deserves medication review rather than automatic classification as a tic.
Dose Reduction Was Enough in Both Tourette Cases
Clinical management in the 2026 report was conservative and informative. Neither patient needed permanent cessation in the published cases. Reducing aripiprazole from 20 mg to 10 mg daily resolved the first patient’s episodes; reducing it from 30 mg to 15 mg daily resolved the second patient’s episodes after anticholinergic coadministration failed.1
That does not create a universal rule that dose reduction is always sufficient. The prior literature included cases resolved by discontinuation and anticholinergic treatment, plus 1 persistent high-dose case. A reasonable clinical hierarchy is narrower:
- Recognize the event: sustained upward eye deviation after a recent dose increase is dystonia-compatible, especially without a premonitory urge.
- Check timing and dose: early onset after initiation or escalation is a core clue in the published pattern.
- Treat it as medication-linked until reviewed: dose reduction, discontinuation, anticholinergic treatment, or switching decisions belong in clinician-supervised care.
- Do not erase tic treatment benefit: aripiprazole can still reduce severe tics for some patients; the point is faster adverse-event recognition, not blanket avoidance.
Evidence strength remains limited. The new paper is a 2-person case report, and the 18 earlier cases are vulnerable to publication bias. Rare, dramatic adverse events are more likely to be written up than uneventful treatment courses. FAERS adds broader signal detection, but spontaneous reports still cannot provide an incidence rate. The practical inference is therefore recognition and monitoring, not numerical risk prediction.
Questions About Aripiprazole and Oculogyric Crisis
Can aripiprazole cause oculogyric crisis even though it is a partial dopamine agonist?
Yes. Published case reports and FAERS signal data indicate that aripiprazole can be linked to dystonic ocular events despite its partial-agonist profile.1,2 Partial agonism still changes dopamine signaling in motor circuits, and the drug does not have strong anticholinergic properties that might reduce acute dystonia risk.
How is oculogyric crisis different from a tic?
Oculogyric crisis usually involves sustained eye deviation from muscle contraction, often lasting minutes. Tics are typically briefer, often preceded by a premonitory urge, and followed by a sense of relief after the tic. Cavanna et al. emphasized that the new eye-rolling episodes in both Tourette patients lacked the usual tic urge and lasted 15–30 minutes.1
Does this mean aripiprazole should never be used for Tourette syndrome?
No. The evidence supports awareness of a rare adverse event, especially around dose escalation. It does not show that aripiprazole is generally inappropriate for tic disorders or that the risk outweighs benefit for every patient.
What should someone do if sustained eye deviation appears after an aripiprazole dose increase?
New sustained upward eye deviation after aripiprazole initiation or escalation should be treated as urgent medication-safety information and reviewed by a clinician. Published management has included dose reduction, discontinuation, and anticholinergic treatment; the right choice depends on severity, recurrence, tic control, psychiatric indication, and available alternatives.1
References
- Cavanna AE, Colangelo C, Melina C, Ravasi A, Arienti G, Riva A, Nacinovich R, Seri S. Oculogyric crisis in two patients treated with aripiprazole for chronic tics. Neurological Sciences. 2026;47:450. https://doi.org/10.1007/s10072-026-09056-7
- Mu C, Chen L. Characteristics of eye disorders induced by atypical antipsychotics: A real-world study from 2016 to 2022 based on Food and Drug Administration Adverse Event Reporting System. Frontiers in Psychiatry. 2024;15:1322939. https://doi.org/10.3389/fpsyt.2024.1322939
- Fountoulakis KN, Siamouli M, Kantartzis S, Panagiotidis P, Iacovides A, Kaprinis GS. Acute dystonia with low-dosage aripiprazole in Tourette’s disorder. Annals of Pharmacotherapy. 2006;40:775–777. https://doi.org/10.1345/aph.1G331
- Lim HK, Pae CU, Lee C, Lee CU. Tardive dystonic symptoms associated with aripiprazole treatment. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2008;32:589–590. https://doi.org/10.1016/j.pnpbp.2007.10.018
- Bhachech JT. Aripiprazole-induced oculogyric crisis (acute dystonia). Journal of Pharmacology and Pharmacotherapeutics. 2012;3:279–281. https://doi.org/10.4103/0976-500X.99446