Auditory hallucinations — voices, usually critical or persecutory — are the most recognized symptom of schizophrenia, reported by up to 75% of patients.9 Antipsychotic medication helps most patients, but roughly a third keep hearing voices despite treatment.
For that group, the question becomes which psychological therapy works best. AVATAR therapy, developed at King’s College London and tested in the UK’s AVATAR1 and AVATAR2 trials, has been getting media attention as the newer, more dramatic option.
A 2026 Hsu network meta-analysis is the first head-to-head synthesis comparing it to standard CBT.
Research Highlights
- About 30% of people on antipsychotics still hear voices.8 When medication doesn’t quiet auditory hallucinations, the next step is psychological therapy. Cognitive behavioral therapy (CBT) is the established option; AVATAR therapy — where a therapist gives the voice a digital face the patient can talk back to — is the newer one.
- Across 26 trials, AVATAR and CBT roughly tie at end of treatment. A 2026 network meta-analysis pooled the trials and found no statistically significant difference between the two for reducing voice severity right after treatment ends.2 A 2021 head-to-head pilot trial reached a similar conclusion.7
- AVATAR’s edge shows up at 3 months. Three months after therapy stops, AVATAR’s benefit holds up better than CBT’s (SMD −0.37, 95% CI −0.69 to −0.05). It also produces a slightly larger reduction in overall psychotic symptoms (SMD −0.41).
- AVATAR uses fewer sessions for similar results. Average 7 sessions over 11 weeks for AVATAR vs. 15 sessions over 18 weeks for CBT. Half the time commitment for comparable benefit, with somewhat better durability — that’s the practical headline.
- The “AVATAR is better than CBT” framing overshoots the formal statistics. The endpoint between-group comparison isn’t significant, and the meta-analysis flags small-study effects (Egger’s test p < 0.01), which usually inflate apparent benefits. Both treatments work for voices; AVATAR is a viable shorter alternative, not a clear winner on every outcome.
What AVATAR Therapy Actually Does for Auditory Hallucinations
AVATAR (Audio Visual Assisted Therapy Aid for Refractory auditory hallucinations) was developed by Julian Leff and colleagues in 2013 as a proof-of-concept study showing patients could engage in dialogue with a digital representation of their voice.4 The patient describes the voice they hear — how it sounds, what it says, what it looks like if it had a face. The therapist builds a digital avatar matching that description and uses computer software to speak through it in real time. The patient sits in front of a screen and has a face-to-face dialogue with the avatar; the therapist alternates between voicing the avatar and coaching the patient as themselves.
The therapeutic mechanism is similar to exposure-based CBT: bring the feared stimulus into the room, decouple the fear from the encounter, and gradually shift the power dynamic so the patient gains control over the voice. AVATAR makes the voice visible and addressable, which gives the role-play structure CBT uses verbally a more concrete form.
The first adequately-powered AVATAR trial (AVATAR1, Craig et al. 2018, Lancet Psychiatry) showed substantial reductions in voice severity at 12 weeks compared with supportive counseling.5 AVATAR2 (Garety et al. 2024) tested an extended protocol against a brief version and provided more detail on which therapeutic targets drove benefit.6
Standard CBT for psychosis (CBTp) covers similar ground — helping patients reframe the meaning of the voice, develop coping skills, reduce distress — but works through conversation alone. CBTp is recommended by NICE, the American Psychiatric Association, and the Royal Australian and New Zealand College of Psychiatrists for treatment-resistant positive symptoms.1
Numbers from a 2026 Network Meta-Analysis: AVATAR vs. CBT in Psychosis
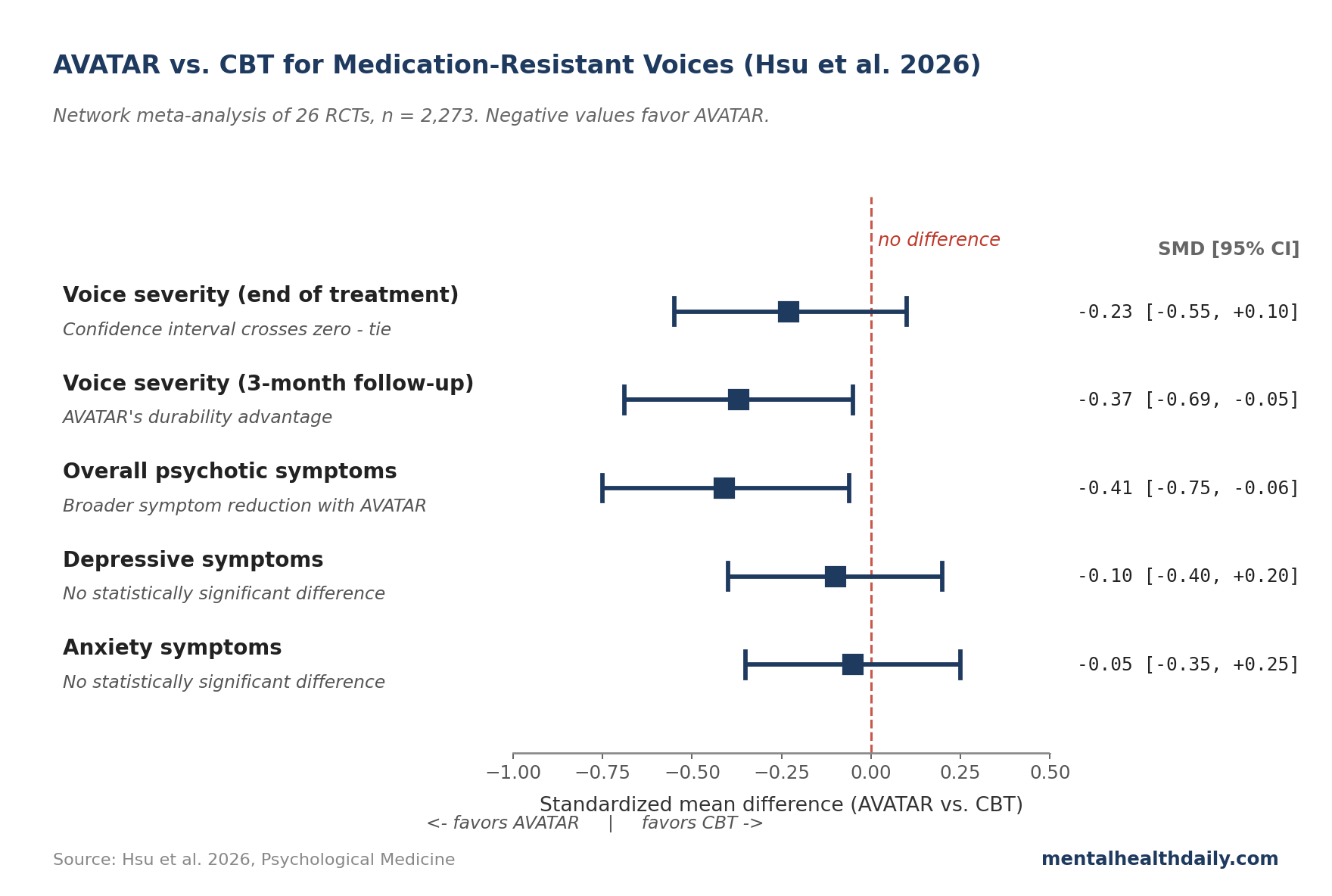
Hsu and colleagues’ 2026 network meta-analysis in Psychological Medicine pooled 26 randomized controlled trials of psychological therapies for medication-resistant auditory hallucinations.2 The trials enrolled 2,273 participants total — mean age 39, 65% male. Network meta-analysis is a way of comparing treatments that haven’t all been tested directly against each other: it links direct head-to-head comparisons with indirect comparisons through shared common controls (treatment-as-usual, supportive psychotherapy) to estimate every-vs-every contrasts.
Headline findings:
- Voice severity right after treatment ends. AVATAR vs. CBT: SMD −0.23 (95% CI −0.55 to 0.10). The standardized mean difference (SMD) lets the meta-analysis pool studies that used different voice-severity scales onto one scale; negative values favor AVATAR. The confidence interval crosses zero, so the difference isn’t statistically confirmed at endpoint.
- Voice severity 3 months after treatment ends. AVATAR vs. CBT: SMD −0.37 (95% CI −0.69 to −0.05). Now the confidence interval doesn’t cross zero — AVATAR’s benefit holds up better through follow-up. This is the cleanest evidence of an AVATAR advantage.
- Overall psychotic symptoms. AVATAR vs. CBT: SMD −0.41 (95% CI −0.75 to −0.06). AVATAR produces a meaningfully larger reduction in broader psychotic-symptom severity, not just voice intensity.
- Positive, negative, depressive, anxiety, quality-of-life outcomes. No statistically significant differences. Discontinuation rates were also comparable.
Stepping back: AVATAR is roughly tied with CBT at endpoint and somewhat better at 3 months, with a slightly broader effect on overall psychotic symptoms. Neither shows a clear edge on mood or quality-of-life secondary outcomes.
Where the Headlines Have Outpaced the Statistics
UK media covered the AVATAR2 trial in 2024 with stories framing AVATAR as a breakthrough that beats traditional therapy. The actual statistics support a more modest claim: AVATAR is comparable to CBT, with somewhat better durability and a session-count advantage. Three reasons to read the apparent advantage cautiously:
- The endpoint comparison crosses zero. SMD −0.23 with CI −0.55 to 0.10 means the data are consistent with anything from a moderate AVATAR advantage to a slight CBT advantage. The point estimate leans AVATAR, but the difference isn’t formally confirmed.
- Small-study effects are detectable. Egger’s test for publication bias was significant at p < 0.01 for the primary AH-severity outcome — meaning small trials with flattering results are over-represented in the literature. When the published trials skew toward small positive studies, the pooled effect is probably inflated. The trim-and-fill correction usually shrinks effects of this kind by 20-40%.
- Risk of bias is high. The Cochrane Risk of Bias 2 tool rated 13 of 26 trials as moderate risk and 7 as high risk. Blinding patients and therapists is essentially impossible in psychotherapy trials, and outcome assessors weren’t always blinded either. The pooled SMDs include some inflation from this.
The honest synthesis: AVATAR works for treatment-resistant voices, somewhere in the same range as CBT, with somewhat better durability at the 3-month mark. Whether it’s actually better than CBT in expectation, or just appears better because of which trials get published, isn’t yet settled.
Why AVATAR Might Be More Efficient
The session-count comparison is the practical headline that doesn’t get the attention it deserves. AVATAR therapy in the trials averaged 7 sessions over 11 weeks. CBT averaged 15 sessions over 18 weeks. AVATAR is delivering roughly comparable benefit in less than half the therapist time.
The likely mechanism is structural. CBT works through repeated conversation, gradually building skills and shifting beliefs. AVATAR adds a face-to-face confrontation with the voice from session one — a high-intensity exposure that may compress the therapeutic process. Patients quickly externalize the voice and start gaining mastery over it, rather than slowly building toward that point.
The clinical implication: if the goal is to treat the largest number of patients with the limited supply of trained psychotherapists, AVATAR’s shorter course may be the more scalable option. The same therapist who can run two CBT courses simultaneously can run four AVATAR courses. The therapist time saved per patient could matter more than a small effect-size advantage.
Where the AVATAR Literature Has Gaps
The evidence base is younger and thinner than CBT’s, and several limitations cut across the trials.
Most AVATAR trials come from a single research group. The Leff/Garety/Craig group at King’s College London ran the original 2013 trial, AVATAR1 (Craig 2018), and AVATAR2 (Garety 2024). Their work is high-quality, but external replication outside the originators is limited. Independent groups tend to produce smaller effect sizes than originator groups across psychotherapy in general — an “allegiance effect” that the AVATAR literature hasn’t yet had time to absorb.
Long-term durability past 6 months is unmeasured. Most trials follow patients for 12-24 weeks. Whether AVATAR’s 3-month durability advantage persists at 1 or 2 years isn’t known. Voices in schizophrenia tend to wax and wane over years; the relevant clinical question is whether either therapy’s benefit translates to durable reduction in distress and hospitalization, and the trial data can’t yet answer that.
Patient selection is narrow. Most trials enrolled stable adults already engaged in mental-health services with voices severe enough to be classified as treatment-resistant but not so severe that they couldn’t participate in structured weekly therapy. Generalizability to acutely ill patients, those without insight, or those without access to specialty mental-health services is limited.
Mechanism comparison hasn’t been formally tested. The plausible reason AVATAR works faster is the embodied confrontation with the voice. But no trial has dismantled this — comparing AVATAR with vs. without the digital-avatar component, for instance — to isolate which active ingredient drives the effect.
How AVATAR and CBT Sit in Practice
Both AVATAR and CBT have a place in treatment-resistant voices, and the choice depends on access and preference rather than strong superiority.
- If access permits, AVATAR is a reasonable first choice for patients with persistent voices on antipsychotics. Shorter course, comparable benefit, somewhat better durability. The 81% probability of being the best intervention in Hsu’s network ranking is suggestive but not confirmatory; the practical efficiency advantage holds either way.
- CBTp remains a strong option and is more widely available. Most NHS, US specialty-clinic, and Australian community-mental-health services that offer psychotherapy for psychosis offer CBTp, not AVATAR. Where AVATAR isn’t available, CBTp is the next-best evidence-based choice. Salahuddin’s 2024 meta-analysis of CBTp vs. treatment-as-usual found a moderate advantage for CBTp on positive symptoms (effect size 0.31).3
- Continue antipsychotic medication during either therapy. Both AVATAR and CBT trials enrolled patients on stable antipsychotic regimens; the therapies are studied as additions, not replacements. Stopping medication during psychological treatment has not been studied and is not advisable.
- Set realistic expectations. Voice severity reduction in trials is moderate, not transformative. Most patients still hear voices after either therapy; the goal is reducing distress and increasing the patient’s sense of control, not silencing voices entirely. AVATAR’s average effect size suggests a real but bounded benefit.
- If neither AVATAR nor CBTp is locally available, ask about supportive psychotherapy. The Hsu network found supportive psychotherapy worse than AVATAR but comparable to CBT on some outcomes. It’s better than no psychological treatment.
Questions About AVATAR Therapy
Is AVATAR therapy actually better than CBT for hearing voices?
Roughly comparable at end of treatment; somewhat better at 3-month follow-up. AVATAR’s 81% probability of being the best intervention in the network ranking is suggestive, but the formal endpoint between-group test isn’t statistically significant. The clearer advantage is durability and a shorter course.2
How does AVATAR therapy work?
A therapist builds a digital avatar that matches the voice the patient hears — the same pitch, tone, and persona — and uses computer software to speak through it. The patient sits in front of a screen and has face-to-face dialogue with the avatar; the therapist alternates between voicing the avatar and coaching the patient. Over 6-8 sessions, the patient gradually gains control over the encounter.
How long does AVATAR therapy take?
Trials averaged 7 sessions over 11 weeks. CBT for the same population averaged 15 sessions over 18 weeks — AVATAR is roughly half the time commitment for comparable benefit.
Is AVATAR therapy widely available?
Not yet. Most of the trial work has been done in the UK at King’s College London, with smaller programs in Canada and Australia. Roll-out outside research settings is limited; CBTp is far more widely available in NHS, US, and Australian mental-health services. That gap is the major practical barrier to AVATAR adoption.
Can AVATAR therapy replace antipsychotic medication?
No. The trials studied AVATAR as an add-on for patients whose voices persisted despite stable antipsychotic treatment. Stopping medication during therapy has not been tested and is not advisable.
Does AVATAR work for command hallucinations or persecutory voices specifically?
The trials enrolled patients with persistent distressing voices broadly. AVATAR’s mechanism — gaining control over the voice through direct dialogue — is particularly suited to persecutory and commanding voices, which is what most participants reported. Whether it works as well for non-distressing or pleasant voices isn’t well-studied.
What if I don’t want to face the voice directly?
CBTp is a reasonable alternative that doesn’t require confronting the voice with a digital face. The therapeutic work happens through conversation rather than embodied confrontation, which some patients prefer.
References
- Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Galletly C et al. Australian and New Zealand Journal of Psychiatry. 2016;50(5):410-472. doi:10.1177/0004867416641195
- AVATAR versus cognitive-behavioral therapy for medication-resistant auditory hallucination: a systematic review and network meta-analysis. Hsu TW et al. Psychological Medicine. 2026;56:e107. doi:10.1017/S0033291726104127
- Cognitive behavioural therapy for the positive symptoms of schizophrenia: a systematic review and meta-analysis. Salahuddin NH et al. Schizophrenia Research. 2024;264:392-401. doi:10.1016/j.schres.2024.01.019
- Computer-assisted therapy for medication-resistant auditory hallucinations: proof-of-concept study. Leff J et al. British Journal of Psychiatry. 2013;202:428-433. doi:10.1192/bjp.bp.112.124883
- AVATAR therapy for auditory verbal hallucinations in people with psychosis: a single-blind, randomised controlled trial. Craig TKJ et al. The Lancet Psychiatry. 2018;5(1):31-40. doi:10.1016/S2215-0366(17)30427-3
- AVATAR therapy for distressing voices: a comprehensive account of therapeutic targets. Garety PA et al. Schizophrenia Bulletin. 2024;50(5):1059-1069. doi:10.1093/schbul/sbae014
- A randomized trial of avatar therapy versus cognitive-behavioral therapy for the treatment of persistent auditory verbal hallucinations in schizophrenia. Dellazizzo L et al. Schizophrenia Research. 2021;229:53-60. doi:10.1016/j.schres.2021.01.016
- The treatment of chronic schizophrenia with neuroleptic drugs: a meta-analysis. Sommer IE et al. Schizophrenia Bulletin. 2012;38(4):704-714. doi:10.1093/schbul/sbq099
- The prevalence and clinical significance of auditory hallucinations in clinical and non-clinical groups. Waters F, Fernyhough C. Schizophrenia Bulletin. 2017;43(1):32-43. doi:10.1093/schbul/sbw132