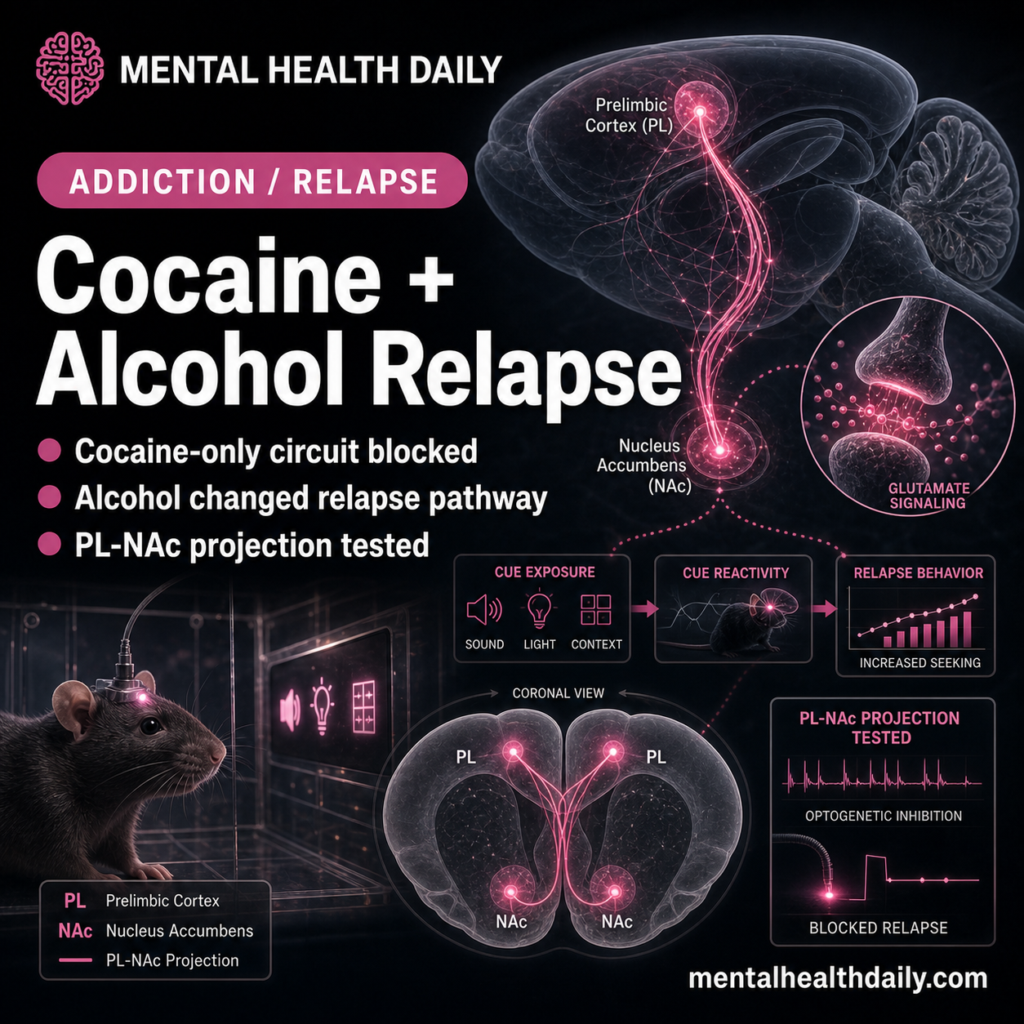
Cocaine relapse circuitry looks different when alcohol is part of the history. In a rat model, inhibiting prelimbic cortex neurons projecting to the nucleus accumbens core blocked cue-triggered cocaine seeking after cocaine alone, but failed after sequential cocaine-alcohol polysubstance use.1
Research Highlights
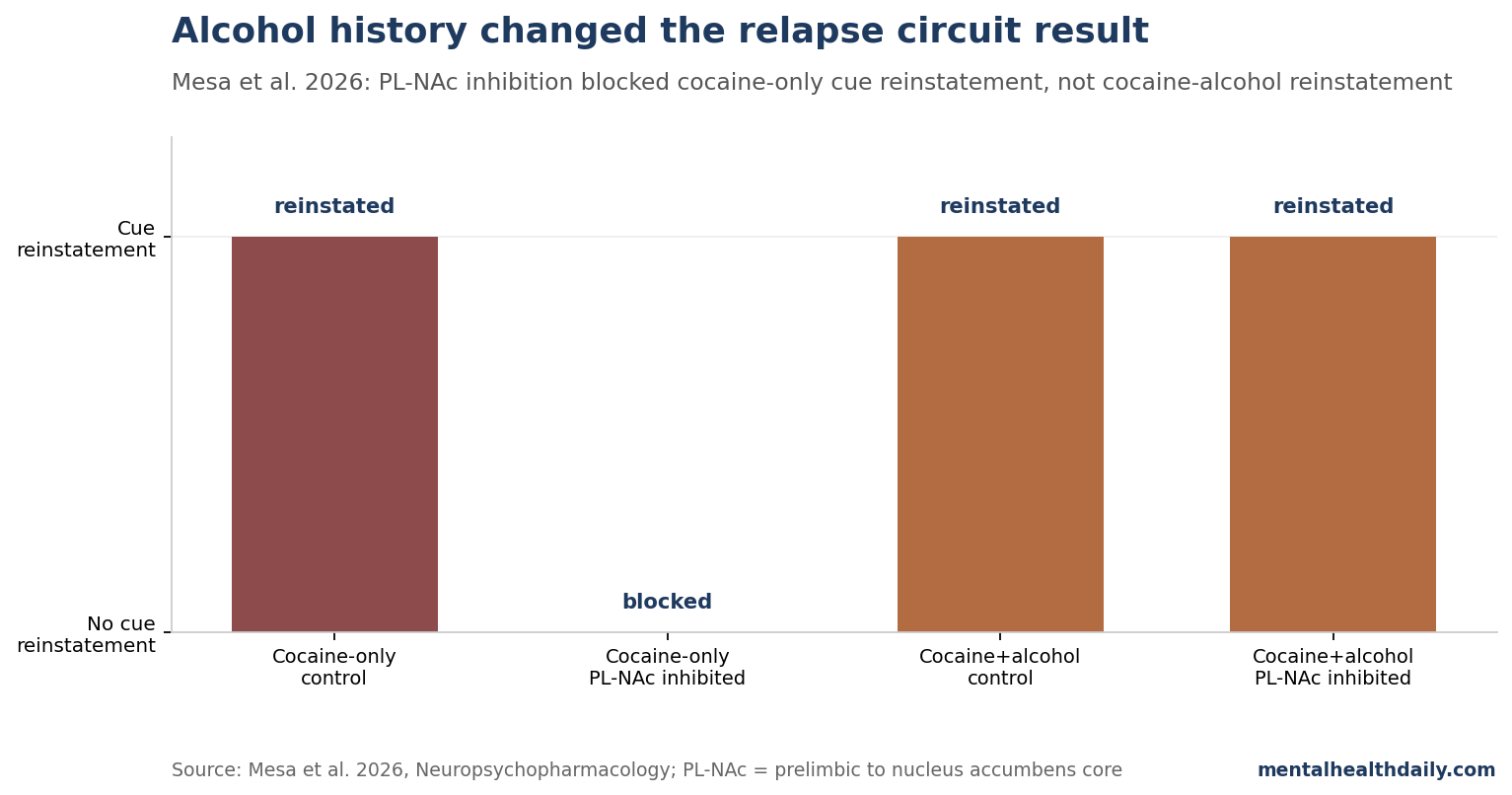
- PL-NAc inhibition split by drug history: in a 4-group DREADD experiment, inhibiting the prelimbic-to-nucleus-accumbens-core projection prevented cue-primed reinstatement in cocaine-only rats, but not in cocaine-alcohol rats.1
- 2020 glutamate work pointed the same way: 2 earlier cocaine-alcohol studies found nucleus accumbens glutamate adaptations distinct from cocaine alone, including altered reinstatement-associated glutamate signaling.2,3
- Experiment 2 restrained the circuit claim: activating the same projection did not increase cue-primed reinstatement or cocaine-induced locomotion.1
- Small groups limit the claim: final reinstatement-test groups ranged from 7 to 8 rats, so the finding should guide circuit hypotheses more than clinical claims.1
- 0 approved medications raises the stakes: cocaine use disorder with alcohol co-use may need treatment models that are not inferred only from cocaine-only circuitry.
Cocaine cues can recruit a prefrontal-to-accumbens relapse pathway, and that pathway has real experimental support. The prelimbic cortex sends excitatory projections to the nucleus accumbens core, a route long implicated in cue-driven drug seeking.
Most people with cocaine use disorder, however, do not use cocaine in a clean laboratory vacuum.
Alcohol co-use is common, clinically important, and biologically relevant. Cocaine plus alcohol can produce cocaethylene, extend intoxication, and change patterns of reinforcement. The Mesa paper asks a narrower circuit question: after a cocaine-alcohol history, does the same prelimbic-to-accumbens pathway still control cue-triggered cocaine seeking?
Sequential Cocaine-Alcohol Use Tested a Specific Relapse Projection
The study by Mesa et al. used a rat model of sequential polysubstance use. Rats self-administered intravenous cocaine, then had access to either water alone or 20% alcohol. After extinction training, the researchers tested cue-primed reinstatement—the animal-model version of a drug-associated cue pulling cocaine seeking back online.1
The experimental setup is easiest to read as a study snapshot:
- Projection tested: prelimbic cortex neurons projecting to the nucleus accumbens core.
- Method: chemogenetic DREADDs, with hM4Di used to inhibit and hM3Dq used to stimulate the projection.
- Experiment 1 final groups: cocaine+water+GFP n = 7; cocaine+water+hM4Di n = 7; cocaine+alcohol+GFP n = 8; cocaine+alcohol+hM4Di n = 7.
- Main behavioral endpoint: active lever presses during cue-primed reinstatement compared with the final 2 days of extinction.1
The experiment is narrow by design. It does not model all polysubstance use, human relapse, withdrawal, trauma, psychiatric comorbidity, or treatment. It tests whether one projection involved in cocaine relapse still carries the same causal weight after alcohol has been added to the drug history.
Inhibition Blocked Cocaine-Only Reinstatement, Not Cocaine-Alcohol Reinstatement
The key result came from Experiment 1. During cocaine self-administration, cocaine intake increased over time, and active lever presses increased as well. During extinction, active lever pressing declined. Then came the reinstatement test.1
The critical interaction was Liquid × AAV × Time, F(1,25) = 4.476, P < 0.05. Post-hoc tests showed active lever presses increased from extinction to test in the cocaine+water+GFP, cocaine+alcohol+GFP, and cocaine+alcohol+hM4Di groups, but not in the cocaine+water+hM4Di group.1
Plain English: silencing the prelimbic-to-accumbens-core projection stopped cue-triggered cocaine seeking when the rats had cocaine-only history. It did not stop cue-triggered cocaine seeking when the rats had cocaine plus alcohol history.
Alcohol Co-Use May Move Relapse Away From the Classic Glutamate Pattern
The result fits earlier work from the same research line. Stennett and Knackstedt reported that cocaine-alcohol polysubstance self-administration produced altered cocaine seeking and altered glutamate levels in the nucleus accumbens.3 A later Neuropsychopharmacology paper found nucleus accumbens core glutamate-homeostasis adaptations after sequential cocaine-alcohol self-administration that differed from cocaine-only adaptations.2
Glutamate homeostasis means the system that keeps excitatory signaling in the nucleus accumbens from becoming either too quiet or too reactive. In cocaine-only models, reinstatement is often tied to prefrontal glutamate drive into the nucleus accumbens core. Alcohol exposure could change that setup through several related mechanisms:
- Transporter function: altered glutamate clearance can change how much extracellular glutamate is available when a drug cue appears.
- Receptor tone: changed receptor sensitivity can make the same prefrontal input land differently in accumbens circuitry.
- Baseline accumbens state: a cocaine-plus-alcohol history may leave the downstream circuit less dependent on the classic PL-NAc route.
The PL-NAc projection can look causal when the accumbens state is cocaine-shaped, then lose that leverage when the accumbens state is cocaine-plus-alcohol-shaped. Mesa et al. therefore point to circuit-specific loss of explanatory power after alcohol enters the drug history: treatment targets built from cocaine-only circuitry could underperform when cocaine use is embedded in alcohol co-use.
Stimulation Did Not Prove the Projection Is Sufficient
The stimulation experiment is an important restraint on the story. DREADD-mediated stimulation of the prelimbic-to-accumbens-core projection did not increase cue-primed reinstatement and did not increase cocaine-induced locomotion.1
That prevents an overly simple interpretation. The projection can be necessary for cue-primed reinstatement after cocaine alone, because inhibiting it blocked the behavior. But it was not obviously sufficient to drive extra seeking when stimulated under the tested conditions.
Circuit neuroscience often separates necessity from sufficiency. A pathway can be required in one state without being a universal accelerator.
State dependence: drug history, cue context, extinction learning, alcohol exposure, sex, withdrawal duration, stress, and receptor adaptation can all change which lever in the circuit actually moves behavior.
Why Cocaine-Only Models Can Mislead Treatment Thinking
Cocaine use disorder has no FDA-approved medication, and relapse remains a major clinical problem. That makes mechanistic animal models necessary. But the Mesa paper highlights a translational trap: if the model excludes common co-use patterns, it may identify a pathway that is true for the model and incomplete for the clinic.
Cocaine-alcohol co-use is a common clinical pattern. A cocaine-only circuit model should be treated as one case within a broader human relapse landscape. A medication, neuromodulation target, or behavioral treatment that reduces cue reactivity in cocaine-only circuitry may need a different test when alcohol has shaped the same reward system.
The same caution applies to biomarker thinking. If a relapse biomarker is trained on cocaine-only cue reactivity, it may partly measure the wrong circuit in cocaine-alcohol users. A null result in a polysubstance sample could mean the sample is biologically mixed. For treatment trials, that argues for stratifying by alcohol co-use as a core biological variable.
Model-design implication: polysubstance use should be built into preclinical addiction models earlier, before a treatment target has been overfit to cocaine-only circuitry. The clinically common case deserves first-class modeling.
How to Interpret Cocaine-Alcohol Relapse Circuitry
For addiction neuroscience: the PL-NAc pathway remains important, but its causal role depends on drug history. “Cocaine relapse circuitry” is not one fixed wiring diagram.
For treatment development: alcohol co-use should be an effect modifier. It may change glutamate homeostasis, cue reactivity, and which circuit interventions work.
For clinical framing: patients using cocaine and alcohol together should not be treated as cocaine-only patients with an extra habit. The combination may create a different relapse biology.
For interpretation: this is a small rat circuit study, not a human treatment trial. Its value is mechanistic direction: it tells researchers where the cocaine-only model may be insufficient.
Evidence-strength note: chemogenetic rat work can test circuit necessity more directly than a human observational study, but it still models a narrow relapse slice. Cue-primed reinstatement after extinction is not the same as relapse after treatment, social stress, withdrawal symptoms, financial pressure, or mixed drug availability in people.
The useful next step is a better preclinical screen before any direct leap to PL-NAc neuromodulation:
- Compare drug histories: test candidate medications and circuit manipulations in cocaine-only, alcohol-only, and cocaine-alcohol histories side by side.
- Stress-test the target: ask whether sex, withdrawal duration, and drinking pattern change the result.
- Raise the translational bar: a target that survives those comparisons is more clinically credible than one discovered only in a simplified cocaine-only model.
That framing also affects clinical measurement. Trials that enroll cocaine users should record alcohol co-use with enough detail to distinguish occasional drinking, binge-linked cocaine use, and sustained polysubstance patterns. Those groups may not share the same cue biology.
Questions About Cocaine-Alcohol Relapse Circuits
What did inhibiting the PL-NAc projection do?
It blocked cue-primed cocaine seeking in rats with cocaine-only history, but not in rats with sequential cocaine-alcohol polysubstance history.1
Does alcohol make cocaine relapse stronger?
This paper is not mainly about stronger versus weaker relapse. It shows that alcohol co-use changed which circuit controlled reinstatement behavior.
Does this prove a human treatment target?
No. The study uses rats, chemogenetics, and cue-primed reinstatement. It points to a mechanism that should be tested in more clinically realistic models.
Why is the nucleus accumbens core important?
The nucleus accumbens core is a major reward and motivation node. Prefrontal glutamate inputs into it have been repeatedly implicated in cue-triggered drug seeking and relapse models.4
References
- The Role of the Prelimbic Cortex to Nucleus Accumbens Core Projection in the Reinstatement of Cocaine-Seeking After Cocaine-Alcohol Polysubstance Use. Mesa JR, Dick SY, Greenan K, Wu L, Knackstedt LA. Neuropsychopharmacology. 2026;51:769–777. doi:10.1038/s41386-025-02198-w
- Sequential Cocaine-Alcohol Self-Administration Produces Adaptations in Rat Nucleus Accumbens Core Glutamate Homeostasis That Are Distinct From Those Produced by Cocaine Self-Administration Alone. Stennett BA, Padovan-Hernandez Y, Knackstedt LA. Neuropsychopharmacology. 2020;45:441–450. doi:10.1038/s41386-019-0452-2
- A Rat Model of Cocaine-Alcohol Polysubstance Use Reveals Altered Cocaine Seeking and Glutamate Levels in the Nucleus Accumbens. Stennett BA, Knackstedt LA. Frontiers in Neuroscience. 2020;14:877. doi:10.3389/fnins.2020.00877
- Anatomy and Pharmacology of Cocaine Priming-Induced Reinstatement of Drug Seeking. Kalivas PW, McFarland K. European Journal of Pharmacology. 2005;526(1-3):77–88. doi:10.1016/j.ejphar.2005.09.068
- Persistent Strengthening of the Prefrontal Cortex-Nucleus Accumbens Pathway During Incubation of Cocaine-Seeking Behavior. Ma YY, et al. Neurobiology of Learning and Memory. 2016;138:281–289. doi:10.1016/j.nlm.2016.10.003