Psychopathy is not a simple “low empathy equals abnormal brain scan” story. In 804 incarcerated men, psychopathy factors tracked empathic concern, perspective taking, cortical thickness, surface area, and cortical organization—but self-reported empathy scores did not map cleanly onto cortical structure.1
Research Highlights
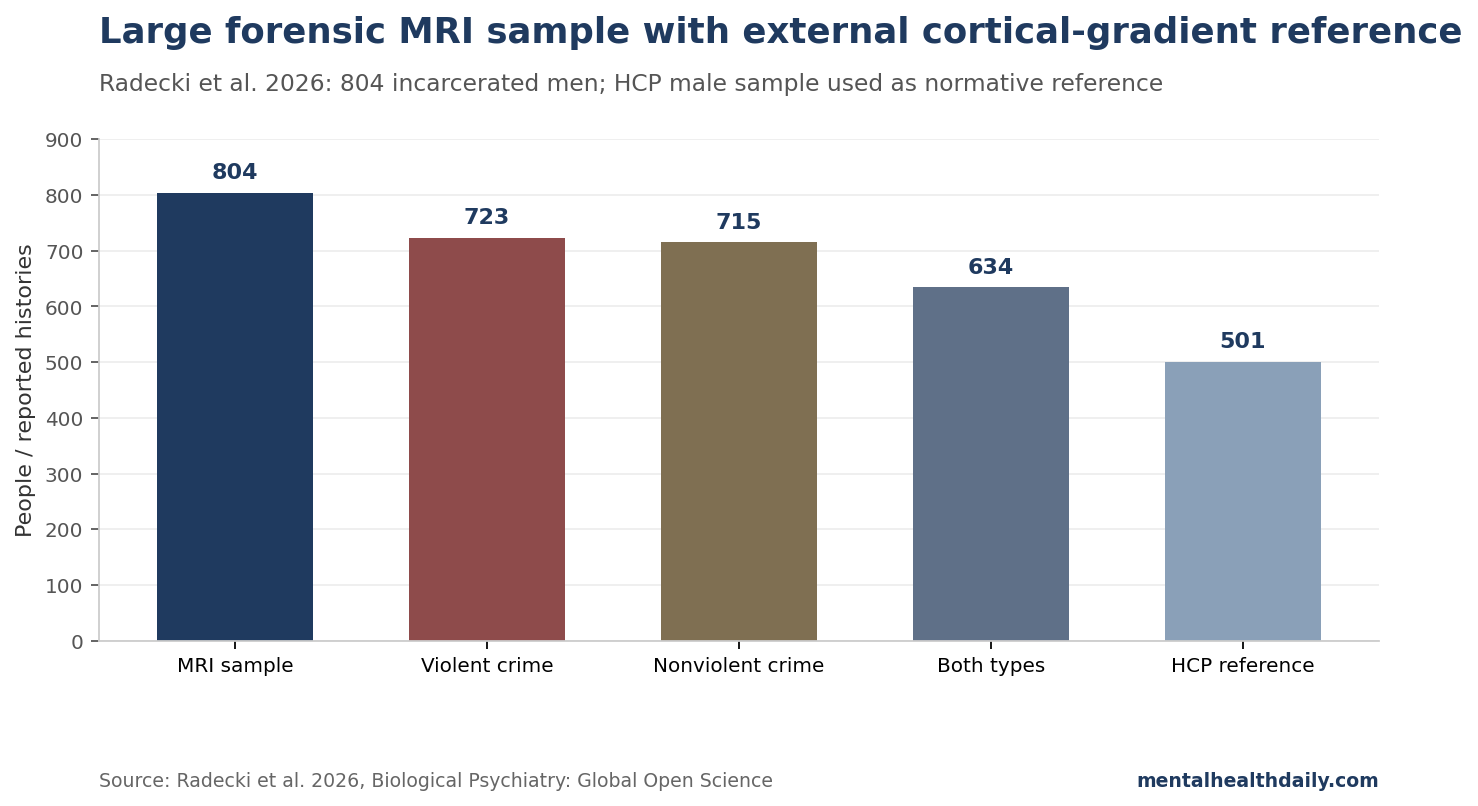
- The sample was unusually large for forensic MRI. Radecki et al. analyzed 804 incarcerated adult men with T1-weighted MRI, PCL-R psychopathy ratings, and empathy measures.1
- Psychopathy factors split by empathy domain. PCL-R factor 1, the interpersonal/affective factor, was uniquely negatively related to empathic concern; factor 2, the lifestyle/antisocial factor, was uniquely negatively related to perspective taking.1
- Empathy scores did not produce a clean cortical map. Cortical thickness and surface area were not related to the IRI empathy subscales, which argues against a simple empathy-region story.1
- Psychopathy itself had structural signals. Cortical thickness related mostly positively to factor 1, surface area related positively to both factors, and high-psychopathy men showed increased surface area and compressed cortical-thickness organization.1
- Clinical use stays dimensional: the 804-person MRI dataset supports brain-behavior co-alteration in psychopathy, but it does not make MRI a diagnostic shortcut for empathy, violence, or moral responsibility.
Brain scans of 804 incarcerated men will always tempt a deterministic headline: psychopathy has a brain signature, therefore the person is explained. The actual result is more useful because it is less cinematic. Psychopathy factors showed brain associations; empathy measures did not light up a simple structural empathy circuit.
Psychopathy is a personality configuration, not a single lesion. Empathy is not one trait either. Cognitive empathy, affective resonance, empathic concern, manipulation, impulsivity, and antisocial behavior can separate. Any interpretation has to keep those pieces apart.
804 Incarcerated Men, PCL-R Ratings, and 360 Cortical Regions
The study began with 912 incarcerated adult men recruited from correctional facilities in the southwestern and midwestern United States. After MRI quality control, missing-data exclusions, and IQ exclusions, the analytic sample contained 804 men. About 90% reported having committed a violent crime, about 89% a nonviolent crime, and about 79% both.1
The design is easiest to read as a study snapshot:
- Psychopathy measure: Psychopathy Checklist-Revised (PCL-R), separated into factor 1 interpersonal/affective traits and factor 2 lifestyle/antisocial traits.
- Empathy measures: Interpersonal Reactivity Index perspective taking (IRI-PT) and empathic concern (IRI-EC).
- MRI measures: cortical thickness, cortical surface area, and structural-covariance gradients across 360 cortical regions.
- Normative comparator: a 501-man Human Connectome Project sample used as an external reference for anterior-posterior cortical-thickness gradients.1
The PCL-R split is important. Factor 1 captures the interpersonal and affective side of psychopathy: shallow affect, manipulation, lack of remorse, and low empathic concern. Factor 2 captures lifestyle and antisocial features: impulsivity, irresponsibility, poor behavior control, and antisocial behavior. Treating those as one lump can obscure which psychological feature is doing the work.
The sample restriction matters too. These were incarcerated men, most with substantial offending histories. The findings should not be casually generalized to women, community samples, adolescents, non-incarcerated adults with psychopathic traits, or people with callousness emerging from different developmental pathways.
Factor 1 Mapped to Empathic Concern; Factor 2 Mapped to Perspective Taking
The psychological result split psychopathy factors across empathy measures. PCL-R factor 1 was uniquely negatively related to empathic concern, while factor 2 was uniquely negatively related to perspective taking.1
Plain English: the interpersonal/affective part of psychopathy looked more tied to not caring about another person’s welfare, while the antisocial/lifestyle part looked more tied to difficulty taking another person’s perspective. Those are not the same deficit.
A 2022 meta-analysis across 477 records and 142,692 participants supports the same split: psychopathy, antisocial behavior, and empathy are related in complicated ways that depend on the empathy framework and psychopathy dimension being used.2 Psychopathy is broader than “no empathy.” Some people high in psychopathic traits may read others well enough to manipulate them while showing reduced concern for others’ suffering.
Empathy Scores Did Not Map Cleanly to Cortical Structure
The paper’s most useful correction is negative. Cortical structure was not related to the IRI empathy subscales. That means lower empathic concern or perspective taking did not translate into a simple cortical-thickness or surface-area map.1
Empathy neuroscience is vulnerable to oversimplification. Functional studies often discuss regions such as medial prefrontal cortex, insula, ventromedial prefrontal cortex, striatum, amygdala, and somatosensory networks. But a structural MRI measure is not the same as task activation, and a self-report empathy questionnaire is not the same as real-world moral behavior.
Decety et al. have shown, in task-based work, that incarcerated men with high psychopathy can show atypical neural responses during affective perspective taking, especially when imagining another person in pain.4 The new structural paper does not erase that. It says broad cortical anatomy is not a one-to-one proxy for empathy scores.
Psychopathy Had Surface-Area and Gradient Signals
Psychopathy itself did show structural associations. Cortical thickness related to PCL-R factor 1, mostly positively. Surface area related positively to both PCL-R factors. Cortical thickness and surface area also had out-of-sample predictive utility for factor 1.1
When the authors compared low- and high-psychopathy men, the high-psychopathy group had lower empathic concern and increased cortical surface area, but not increased cortical thickness. The largest cortical effect sizes appeared in the paralimbic class and somatomotor network, and spatial overlap with task-based activation meta-analyses was highest for social-affective and sensory clusters.1
That pattern speaks to the older paralimbic model of psychopathy. Kiehl’s cognitive-neuroscience review argued that psychopathy involves dysfunction across paralimbic regions rather than a single damaged moral center.3 The new paper updates the idea with large-sample cortical morphometry and macroscale gradients instead of a simple region list.
Compressed Cortical Organization Is Not a Diagnosis
The gradient finding is interesting but easy to misuse. Structural-covariance gradients describe large-scale organization: how cortical regions covary with one another across people. In the total incarcerated sample, the researchers found anterior-posterior gradients; in high-psychopathy men, the cortical-thickness gradient was globally compressed.1
An individual MRI cannot diagnose psychopathy. Group-level gradients are statistical summaries of cortical organization across samples, not clinical scans. A compressed gradient may tell us something about macroscale cortical patterning in high psychopathy, but it does not identify a person, predict a crime, or settle responsibility.
The practical interpretation: psychopathy is associated with brain structure, but the useful unit is a multidimensional profile: PCL-R factor, empathy domain, cortical metric, network class, and developmental history. Single-number explanations are the failure mode.
How to Interpret Psychopathy Brain Scans Clinically
For forensic evaluation: MRI is not a replacement for structured assessment. The PCL-R, collateral history, behavior, developmental information, and risk formulation remain central.
For treatment research: the separation between empathic concern and perspective taking matters. A program targeting cognitive perspective taking may not repair affective concern, and vice versa.
For public interpretation: “brain differences” should not be translated into inevitability. Brain-behavior associations can inform mechanism without erasing agency, context, trauma exposure, social learning, or intervention potential.
For future studies: larger MRI cohorts need to link structural profiles to longitudinal outcomes: treatment response, recidivism, violence reduction, emotional learning, and real-world prosocial behavior.
The Radecki paper is strong because it resists the simplest answer. It shows that psychopathy has measurable cortical correlates in a large incarcerated sample, while also showing that empathy is not structurally reducible in the way a headline might want.
Evidence-strength note: this is a cross-sectional neuroimaging study. It can connect psychopathy dimensions, empathy scores, and cortical metrics measured at the same broad time point, but it cannot show whether cortical structure caused psychopathic traits, resulted from developmental adversity, reflected incarceration-related selection, or changed with intervention.
Longitudinal work would need to follow high-risk people before incarceration, measure trauma exposure and substance use more deeply, and test whether cortical profiles predict later behavior beyond structured risk tools. Until then, the clinical value is conceptual: the study argues against single-cause empathy explanations and for separating affective concern, perspective taking, surface area, cortical thickness, and developmental context.
That distinction also matters for intervention design. If affective concern and perspective taking split across psychopathy factors, then empathy training should not be treated as one generic module. Programs may need different targets for emotional concern, cognitive perspective taking, impulsive antisocial behavior, and violence risk.
Questions About Psychopathy, Empathy, and Brain Structure
Did brain structure predict empathy?
Not cleanly. Cortical thickness and surface area were not related to the IRI perspective-taking or empathic-concern subscales in this study.1
Which psychopathy factor related to empathic concern?
PCL-R factor 1, the interpersonal/affective factor, was uniquely negatively related to empathic concern. Factor 2 was uniquely negatively related to perspective taking.1
Can MRI diagnose psychopathy?
No. These are group-level research findings. They do not make MRI a clinical diagnostic test for psychopathy, empathy, or violence risk.
Why does surface area matter?
Surface area is one dimension of cortical structure. In this study, it related positively to both PCL-R factors and was increased in high-psychopathy men, but the clinical meaning still requires longitudinal work.1
References
- Cortical Structure in Relation to Empathy and Psychopathy in 800 Incarcerated Men. Radecki MA, Maurer JM, Harenski KA, et al. Biological Psychiatry: Global Open Science. 2026;6:100695. doi:10.1016/j.bpsgos.2026.100695
- Refining the Link Between Psychopathy, Antisocial Behavior, and Empathy: A Meta-Analytical Approach Across Different Conceptual Frameworks. Burghart M, Holl AK, Mier D. Clinical Psychology Review. 2022;94:102145. doi:10.1016/j.cpr.2022.102145
- A Cognitive Neuroscience Perspective on Psychopathy: Evidence for Paralimbic System Dysfunction. Kiehl KA. Psychiatry Research. 2006;142(2-3):107–128. doi:10.1016/j.psychres.2005.09.013
- An fMRI Study of Affective Perspective Taking in Individuals With Psychopathy: Imagining Another in Pain Does Not Evoke Empathy. Decety J, Chen C, Harenski C, Kiehl KA. Frontiers in Human Neuroscience. 2013;7:489. doi:10.3389/fnhum.2013.00489
- Specific Electrophysiological Components Disentangle Affective Sharing and Empathic Concern in Psychopathy. Decety J, Lewis KL, Cowell JM. Journal of Neurophysiology. 2015;114(1):493–504. doi:10.1152/jn.00253.2015