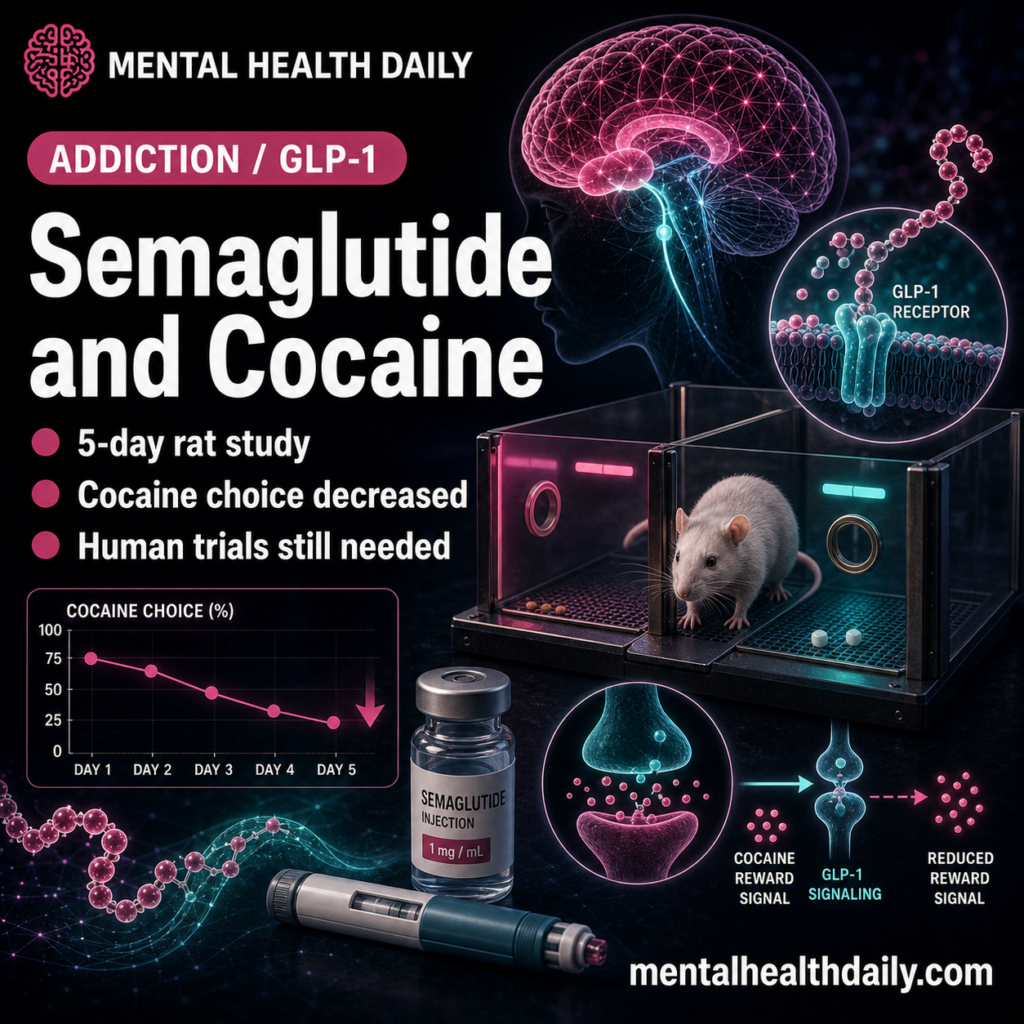
Semaglutide is not close to being an approved cocaine-use-disorder medication, but a 2026 rat study gives the idea a more demanding preclinical test than ordinary self-administration experiments. After 5 days of treatment, rats shifted away from cocaine choice without losing total operant responding, which separates the result from a broad appetite-suppression artifact.
Research Highlights
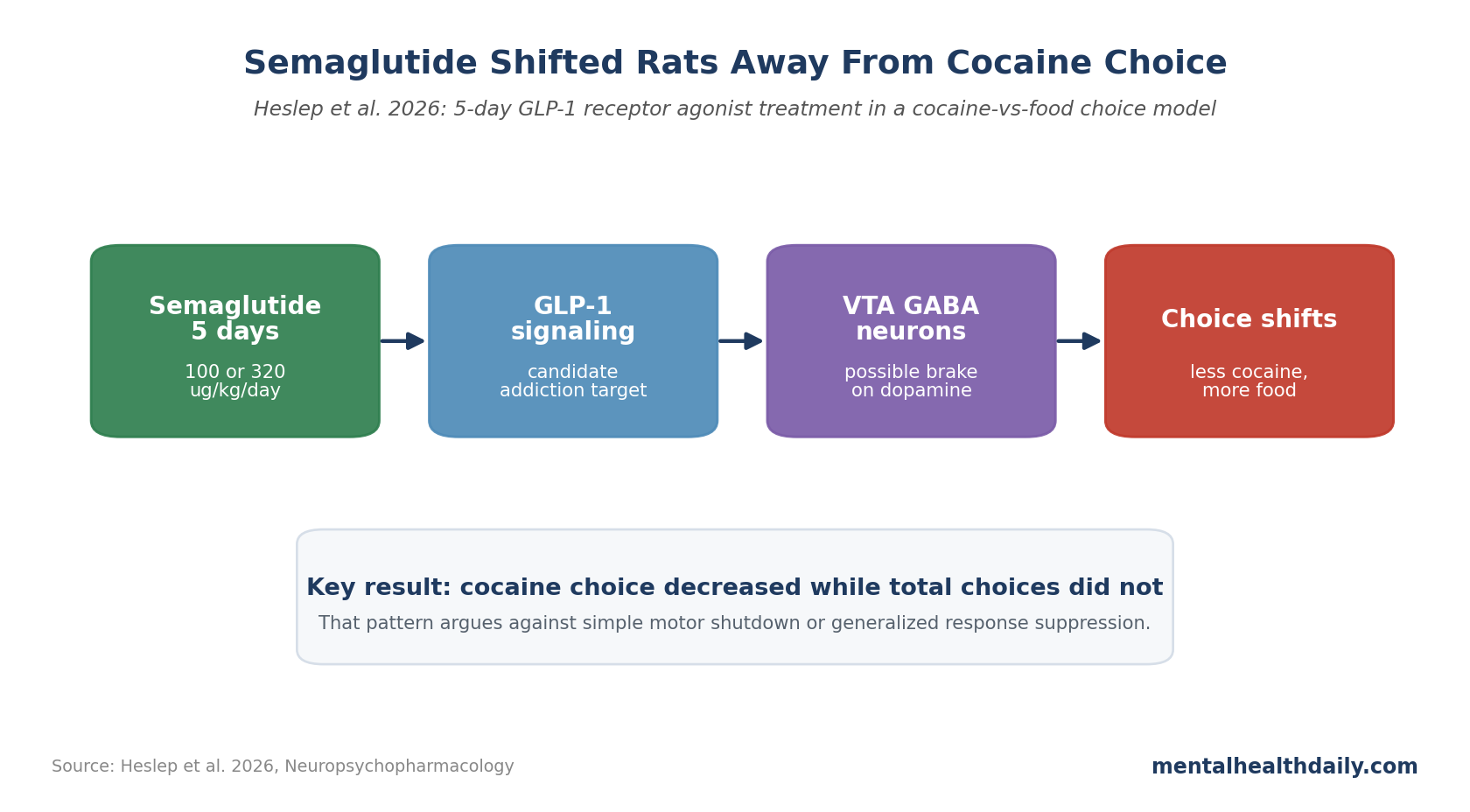
- Semaglutide reduced cocaine choice in rats: repeated 100 and 320 μg/kg/day semaglutide reduced choice of 0.32 mg/kg/infusion cocaine, and 320 μg/kg/day also reduced choice of 0.1 mg/kg/infusion cocaine.
- Total responding stayed intact: after 5 days of dosing, the rats made fewer cocaine choices and more food choices, but total choices did not fall, arguing against a simple sedation or motor-impairment explanation.
- Weight loss is not the whole story: 320 μg/kg/day semaglutide decreased body weight, yet food choices increased at the high dose; that pattern separates cocaine reinforcement from appetite suppression.
- Human evidence remains early: acute exenatide did not reduce cocaine self-administration in a human laboratory study, so the next question is repeated dosing, not whether one GLP-1 exposure instantly blocks cocaine effects.
- Mechanism remains plausible but unfinished: glucagon-like peptide-1 (GLP-1) receptor signaling may reduce ventral tegmental area dopamine output, but antagonist and pathway-specific tests are still needed.
Heslep et al. tested semaglutide in a cocaine-vs-food choice procedure: rats could allocate behavior toward cocaine infusions or toward food reinforcement. That design separates reduced drug-directed behavior from a general flattening of all behavior.
5-Day Semaglutide Shifted Choice Away From Cocaine
Heslep et al. used male and female rats and tested repeated semaglutide over 5 days.1 In the main within-session choice procedure, increasing cocaine dose produced the expected dose-dependent increase in cocaine choice.
Semaglutide changed that allocation. Results did not say “rats stopped responding.” They were narrower and more useful:
- At 0.32 mg/kg/infusion cocaine: both 100 and 320 μg/kg/day semaglutide significantly reduced cocaine choice.
- At 0.1 mg/kg/infusion cocaine: 320 μg/kg/day semaglutide reduced cocaine choice.
- For food behavior: 320 μg/kg/day semaglutide increased food choices, while both active doses decreased session cocaine choices.
- For total behavior: total choices did not change, which makes simple incapacitation a poor explanation.
Statistics were strong for a small animal study: semaglutide effect on cocaine choice, F1.5,19.3 = 15.2, p = 0.0003; cocaine dose effect, F1.3,17.2 = 85.8, p < 0.0001; interaction, F3.3,34.2 = 3.7, p = 0.017. For session food, cocaine, and total reinforcers, the dependent-measure effect was F1.1,11.8 = 105, p < 0.0001, with an interaction of F1.7,17.6 = 8.4, p = 0.004.
A second behavioral-economic procedure tested whether semaglutide changed how much effort rats would allocate to cocaine as the response requirement increased. At 320 μg/kg/day, semaglutide reduced 0.32 mg/kg/infusion cocaine choice at fixed ratio 3 (FR3; 3 lever responses per reinforcer), with semaglutide F1,6 = 35, p = 0.001 and interaction F1.5,5.3 = 8.3, p = 0.027.
No significant sex differences appeared for any dependent measure. The small sample therefore did not show an obvious sex split, while larger studies would still be needed to test male-female moderation.
Cocaine-vs-Food Choice Is a Tougher Preclinical Test
Simple self-administration studies can mistake broad behavioral suppression for anti-addiction benefit. A drug that makes an animal nauseated, sleepy, or unable to respond can look like it reduces cocaine taking even if it has no useful effect on cocaine reinforcement.
Choice design reduces that problem because it asks where behavior goes. In this study, semaglutide moved behavior away from cocaine and toward food instead of lowering all responding. Clinically, the target is less drug-seeking and more behavior allocated to non-drug rewards.
This design has 3 strengths:
- It separates drug-specific effects from global suppression. Total responding stayed intact, which makes the reduction in cocaine choice harder to dismiss as behavioral shutdown.
- It tests competing reinforcement. Cocaine had to compete with food, which better resembles real behavior than an isolated lever-press task.
- It connects to translational pharmacology. Negus and Banks have argued that choice procedures can better model medication goals for substance use disorders than one-reinforcer self-administration tasks.8
Earlier GLP-1 Studies Pointed to Cocaine Reward
GLP-1 addiction rationale: GLP-1 receptor agonists are best known for diabetes and obesity, but addiction researchers have been circling them for years because GLP-1 signaling reaches reward circuitry, stress systems, and feeding pathways.2
The addiction question is whether GLP-1 signaling can change reinforcement and craving-related circuits, not whether weight loss alone reduces addiction.
Earlier mouse work found that exendin-4 reduced cocaine self-administration.7 Egecioglu et al. reported that exendin-4 attenuated rewarding properties of psychostimulant drugs in mice, and Graham et al. found that a GLP-1 analog attenuated cocaine reward.3,4
More recent semaglutide work made the case more specific. Aranäs et al. reported that semaglutide suppressed cocaine taking, seeking, and cocaine-evoked dopamine levels in the nucleus accumbens, a central reward-region output node.5 Merkel et al. described an endogenous GLP-1 circuit engaging ventral tegmental area (VTA) gamma-aminobutyric acid (GABA) neurons to regulate mesolimbic dopamine neurons and attenuate cocaine seeking.6
Human data are thinner and less favorable so far. Angarita et al. tested acute exenatide in people with cocaine use disorder and did not find reduced cocaine self-administration or subjective cocaine effects.9 The trial tested one acute dose, not a repeated semaglutide regimen. Mismatch between acute human exenatide and repeated rat semaglutide prevents easy enthusiasm.
Weight Loss Does Not Explain the Cocaine Result
Semaglutide reduced body weight in the Heslep study: day effect F1.5,20.4 = 108.7, p < 0.0001; dose effect F1,14 = 31.9, p < 0.0001; interaction F1,6.4 = 35.6, p = 0.0009.1 If the cocaine finding were only appetite suppression or sickness, food choices should have fallen too.
They did not. Food choices increased at the high semaglutide dose while cocaine choices fell. Weight changed, but the behavioral allocation moved in a drug-specific direction.
Lorcaserin shows why weight-loss-adjacent pharmacology is not enough. This 5-HT2C receptor agonist failed to reduce cocaine-vs-food choice in rhesus monkeys and later failed in a randomized clinical trial for cocaine use disorder despite body-weight effects.10,11
Semaglutide may still fail in humans. A narrower claim survives: this rat study looks more like a cocaine-choice effect than a “drug made animals eat less” artifact.
VTA GABA and Dopamine Are Plausible, Not Proven
Semaglutide has limited blood-brain barrier penetration, so the mechanism cannot be assumed to be direct, uniform brain entry. GLP-1 biology is distributed across peripheral, vagal, hindbrain, hypothalamic, and reward-circuit pathways.12
Addiction-relevant mechanism likely involves several pieces:
- VTA GABA neurons: GLP-1 receptors on VTA GABAergic neurons may inhibit dopamine neurons that project into the nucleus accumbens.6
- Dopamine selectivity: cocaine reinforcement depends heavily on mesolimbic dopamine signaling, so dampening that pathway could affect cocaine more than food.
- Peripheral and brainstem inputs: semaglutide can affect vagal and hindbrain signaling, which may indirectly change reward valuation and drug seeking.
- Antagonist tests still matter: future work needs to show whether GLP-1 receptor blockade prevents the anti-cocaine-choice effect.
Could Semaglutide Treat Cocaine Addiction?
Cocaine use disorder has no Food and Drug Administration-approved medication. A useful medication would not need to erase cocaine effects completely; even a meaningful reduction in craving, binge frequency, cue-reactivity, or relapse after abstinence could matter if the drug were tolerable and retained patients in treatment.
For semaglutide, clinical testing should answer practical questions before broad claims:
- Repeated dosing: acute exenatide was not enough in humans, so trials should test sustained GLP-1 receptor agonist exposure.
- Patient selection: people with cocaine use disorder plus obesity, diabetes, or cardiometabolic disease may have a different risk-benefit profile than lean patients.
- Retention and nausea: gastrointestinal adverse effects could undermine adherence in a population where treatment retention is already difficult.
- Meaningful endpoints: trials should measure cocaine-negative urine samples, craving, relapse timing, binge frequency, non-drug reward engagement, and subjective drug liking.
Semaglutide is a candidate worth testing, not a proven addiction medication. Rat data clear one preclinical hurdle: the drug shifted choice away from cocaine while preserving behavior allocated to food.
Questions About Semaglutide and Cocaine Use Disorder
Is semaglutide approved for cocaine use disorder?
No. Semaglutide is approved for diabetes and weight management under specific indications, not cocaine use disorder. Any addiction use would require clinical trials showing benefit and acceptable safety.
What exactly did the 2026 rat study show?
After 5 days of semaglutide, rats chose cocaine less often and food more often. Total choices stayed intact, supporting a shift in reward choice rather than broad behavioral shutdown.1
Does this mean weight loss treats addiction?
No. Weight changed, but the behavior pattern points beyond appetite suppression. Food choice increased at the high dose while cocaine choice fell, which is the opposite of what a pure appetite-suppression explanation would predict.
Why would a diabetes and weight-loss drug affect cocaine?
GLP-1 signaling interacts with reward pathways. One plausible route involves VTA GABA neurons reducing dopamine activity in circuits that cocaine strongly recruits.6
Has this worked in people?
Not yet. A human laboratory study of acute exenatide did not reduce cocaine self-administration or subjective effects. Repeated semaglutide has not yet been proven clinically for cocaine use disorder.9
Would repeated semaglutide need a human cocaine-use-disorder trial?
A randomized clinical trial of repeated GLP-1 receptor agonist treatment in people with cocaine use disorder, with endpoints that include cocaine use, craving, retention, adverse effects, and non-drug reward behavior.
References
- Repeated semaglutide treatment attenuates cocaine-vs-food choice in male and female rats. Heslep N et al. Neuropsychopharmacology. 2026. doi:10.1038/s41386-026-02386-2
- The potential utility of GLP-1 receptor agonist medications for addiction treatment. Yammine L et al. Current Addiction Reports. 2025;12:59. doi:10.1007/s40429-025-00657-4
- The glucagon-like peptide 1 analogue, exendin-4, attenuates the rewarding properties of psychostimulant drugs in mice. Egecioglu E et al. PLOS One. 2013;8:e69010. doi:10.1371/journal.pone.0069010
- GLP-1 analog attenuates cocaine reward. Graham DL et al. Molecular Psychiatry. 2013;18:961–962. doi:10.1038/mp.2012.141
- Semaglutide suppresses cocaine taking, seeking, and cocaine-evoked dopamine levels in the nucleus accumbens. Aranäs C et al. European Neuropsychopharmacology. 2025;98:1–10. doi:10.1016/j.euroneuro.2025.07.001
- An endogenous GLP-1 circuit engages VTA GABA neurons to regulate mesolimbic dopamine neurons and attenuate cocaine seeking. Merkel R et al. Science Advances. 2025;11:eadr5051. doi:10.1126/sciadv.adr5051
- The GLP-1 receptor agonist exendin-4 reduces cocaine self-administration in mice. Sørensen G et al. Physiology & Behavior. 2015;149:262–268. doi:10.1016/j.physbeh.2015.06.013
- Confronting the challenge of failed translation in medications development for substance use disorders. Negus SS, Banks ML. Pharmacology Biochemistry and Behavior. 2021;210:173264. doi:10.1016/j.pbb.2021.173264
- Testing the effects of the GLP-1 receptor agonist exenatide on cocaine self-administration and subjective responses in humans with cocaine use disorder. Angarita GA et al. Drug and Alcohol Dependence. 2021;221:108614. doi:10.1016/j.drugalcdep.2021.108614
- Repeated 7-day treatment with lorcaserin or pimavanserin fails to reduce cocaine vs. food choice in male rhesus monkeys. Banks ML, Negus SS. Neuropsychopharmacology. 2017;42:1082–1092. doi:10.1038/npp.2016.259
- Results of a randomized, double-blind, placebo-controlled trial of lorcaserin in cocaine use disorder. McCann DJ et al. Drug and Alcohol Dependence. 2024;255:111063. doi:10.1016/j.drugalcdep.2023.111063
- Semaglutide lowers body weight in rodents via distributed neural pathways. Gabery S et al. JCI Insight. 2020;5:e133429. doi:10.1172/jci.insight.133429