
A 2026 controlled study of 96 people found severe long-COVID fatigue across 3 validated fatigue scales, but the tested peripheral inflammation, cellular-stress, neuroprotection, and autoimmunity markers did not significantly differ by group or explain fatigue severity.1 The finding argues against a simple blood-marker story, not against the reality of long-COVID fatigue.
Research Highlights
- Fatigue was large: Long-COVID cases had median fVAS 63 versus 5 in recovered controls, FACIT-F 21.5 versus 49, and SF-36 vitality 25 versus 72.5; all p < 0.001.1
- Inflammation markers missed the split: CRP, TNF-α, IL-6, and IL-1β did not show a significant group difference that explained fatigue severity in the 48-case sample.1
- Cellular-stress markers also missed: HSP90α, Serpin F1, hemopexin, and APOA4 were not significantly different between 48 long-COVID cases and 48 recovered controls.1
- Autoimmunity was not the obvious answer: ANA positivity was 10.4% in cases versus 4.2% in controls, p = 0.38, and did not influence fatigue levels.1
- Design limits matter: This 2026 cross-sectional blood study cannot rule out central, autonomic, vascular, metabolic, or time-varying immune mechanisms.
Long-COVID fatigue means persistent exhaustion after SARS-CoV-2 infection that is not explained by ordinary tiredness, deconditioning alone, or a current acute infection. In this study, cases met NICE long-COVID criteria and were compared with recovered controls who also had prior infection.
Peripheral biomarkers are molecules measured in blood outside the brain. They are useful because they are accessible, but a negative blood panel can miss processes inside the central nervous system, immune-cell function, blood-vessel regulation, autonomic control, or energy metabolism.
48 Long-COVID Cases Had Severe Fatigue on 3 Scales
Omdal et al. enrolled 48 people with long COVID and 48 age- and sex-matched recovered controls. The groups were similar in age, and 82 of 96 participants were female. The researchers excluded conditions that could independently explain fatigue, then measured fatigue with 3 established instruments.
The Fatigue Visual Analog Scale (fVAS) runs from 0 to 100, with higher scores meaning worse fatigue. Long-COVID cases had a median score of 63, compared with 5 in recovered controls. The Functional Assessment of Chronic Illness Therapy-Fatigue scale (FACIT-F) moves in the opposite direction: lower scores mean worse fatigue. Cases scored 21.5 versus 49 in controls. SF-36 vitality also favored controls, 25 versus 72.5.1
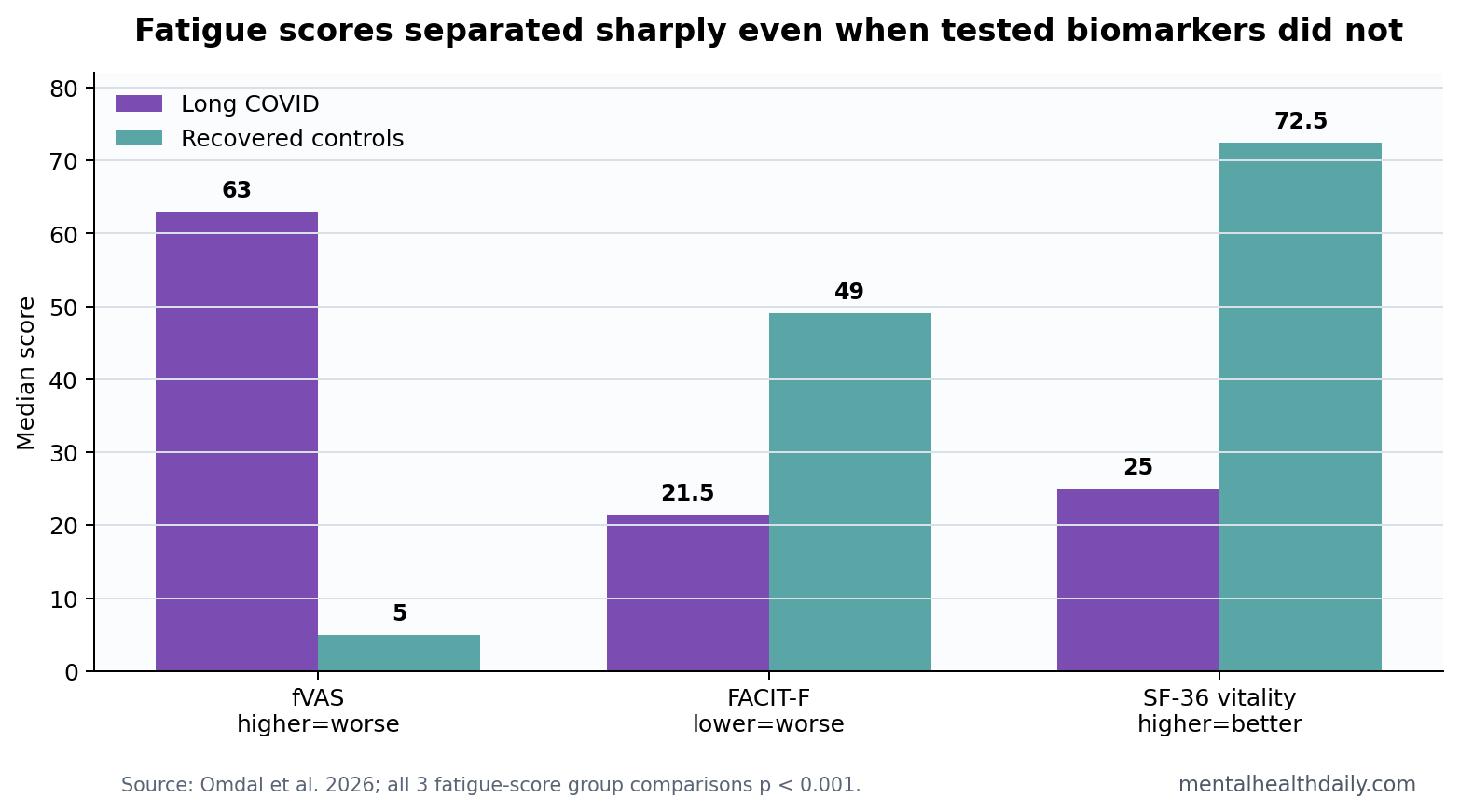
The symptom separation is important because it prevents a common misread of biomarker-negative studies. The patients were not mildly tired people with a vague complaint. The fatigue signal was clinically large; the tested blood markers simply did not map onto it.
CRP, TNF-Alpha, and IL-6 Did Not Explain Fatigue Severity
CRP (C-reactive protein) is a broad inflammation marker. TNF-α and IL-6 are cytokines, signaling proteins immune cells use to coordinate inflammation. They are plausible fatigue candidates because inflammatory illnesses can produce sickness behavior: fatigue, reduced activity, low appetite, and cognitive slowing.
In this sample, CRP did not differ significantly between groups. TNF-α and IL-6 trended higher in long-COVID cases, both p = 0.07, but neither reached statistical significance, and regression models did not show significant associations between the selected markers and fatigue severity.1
Calibration: p = 0.07 is not proof of no biology. It is also not confirmation of the inflammation explanation. The honest read is that this specific panel did not produce a reliable fatigue biomarker in 48 cases.
Cellular-Stress and Neuroprotection Markers Were Also Flat
The researchers also tested markers outside the usual CRP-cytokine frame. HSP90α is a heat-shock protein involved in cellular stress responses. Serpin F1, also called pigment epithelium-derived factor, is linked to neuroprotection and inflammation regulation. Hemopexin binds free heme, and APOA4 is an apolipoprotein involved in lipid transport and inflammatory signaling.
None of these markers significantly separated long-COVID cases from recovered controls. HSP90α was 9.3 ng/mL in cases versus 10.1 in controls, p = 0.20. Serpin F1 was 13.7 versus 13.0 μg/mL, p = 0.65. CRP was 1.0 versus 0 mg/L, p = 0.32.1
That pattern narrows the claim. A blood test built from these candidates would not have separated fatigued long-COVID cases from recovered controls in this study. It does not show that fatigue is psychological, invented, or unrelated to post-infectious biology.
ANA Positivity Did Not Support a Simple Autoimmune Explanation
Anti-nuclear antibodies (ANA) are immune markers sometimes used as a screen for autoimmune conditions. ANA positivity appeared in 5 of 48 long-COVID cases, or 10.4%, and 2 of 48 recovered controls, or 4.2%. The group difference was not statistically significant, p = 0.38.1
ANA status also did not influence fatigue levels or biomarker concentrations. That result weakens a simple conventional-autoimmunity explanation in this sample. It does not rule out immune dysregulation that would require different assays, different timing, cell-specific tests, or tissue-specific sampling.
Why This Does Not Settle Long-COVID Mechanisms
Ceban et al. showed that fatigue after COVID-19 is common enough to be a major public-health and clinical problem, not a rare curiosity.2 The Omdal study adds a sharper point: the presence of severe fatigue does not guarantee that ordinary peripheral inflammation markers will be abnormal at one blood draw.
Adjacent fatigue evidence: ME/CFS and inflammatory-disease literature warns against one-marker thinking. Montoya et al. reported cytokine-severity associations in ME/CFS, but the broader field has struggled with replication, subgrouping, and assay timing.3
Anti-TNF therapy can improve fatigue in some inflammatory diseases, while post-viral fatigue may involve different mechanisms than TNF-α measured in peripheral blood.4
Normal Blood Markers Still Have Clinical Value
A biomarker-negative result can still help care if it prevents false precision. If routine blood markers are normal, the patient can still be severely fatigued. The study’s fVAS, FACIT-F, and SF-36 vitality differences make that explicit. Normal CRP or IL-6 should not be used as a shortcut for dismissing the symptom.
Rule-out value: basic labs can still identify anemia, thyroid disease, liver disease, kidney disease, autoimmune disease, inflammatory flare, medication effects, or other treatable contributors. Omdal et al. excluded several fatigue-related conditions before the final comparison, which made the long-COVID signal cleaner but also means ordinary clinical screening still belongs before a post-infectious fatigue label is treated as final.
Research value: negative markers sharpen the next study. A useful next panel would need to test time-varying immune activation, autonomic physiology, exercise intolerance, vascular function, sleep disruption, mitochondrial signaling, or central nervous system processes rather than only repeating the same peripheral proteins in a similar sample.
The recovered-control comparison is also important. Controls had prior SARS-CoV-2 infection but did not have long COVID, and their fatigue scores looked similar to pre-pandemic healthy controls in the study’s additional comparison. That design makes the result more specific than a simple infected-versus-never-infected contrast, because both main groups had passed through the viral exposure.
Patient-facing interpretation: a normal inflammatory panel should shift the diagnostic search, not close it. The next question is which mechanism better explains exertional intolerance, brain fog, sleep disruption, orthostatic symptoms, pain, or post-exertional worsening in that individual patient.
The depression comparison also helps keep the result precise. Omdal et al. measured depressive symptoms with HADS-D because depression can worsen perceived energy and overlap with fatigue. Their biomarker models still failed to identify a reliable fatigue predictor. That does not make mood irrelevant; it means the tested blood markers were not quietly explaining fatigue through measured depression either.
For patients, that distinction is concrete: fatigue can be assessed seriously even when mood symptoms, ordinary inflammatory labs, and autoimmune screening do not give a tidy explanation.
Care-pathway implication: a biomarker-negative visit should still document functional limits. Walking tolerance, post-exertional symptom worsening, orthostatic symptoms, sleep quality, work capacity, medication effects, and pacing response may be more useful for day-to-day management than repeating the same inflammation panel. The study makes that practical point by showing severe fatigue without a matching peripheral-marker signature.
Rehabilitation plans should also avoid assuming that normal inflammatory markers mean ordinary deconditioning. Graded activity, pacing, sleep treatment, and autonomic evaluation answer different clinical questions.
Function is the clinical signal that should not be lost.
Evidence-strength note: this was a cross-sectional case-control study. It can show that a tested marker panel did not separate groups or correlate with fatigue at the study visit. It cannot show what happened during acute infection, whether markers fluctuated earlier, or whether a central nervous system process persisted without a peripheral blood signature.
Questions About Long-COVID Fatigue Biomarkers
Does a negative biomarker panel mean long-COVID fatigue is psychological?
No. It means this peripheral blood panel did not explain the fatigue signal. Severe symptoms can exist without a convenient blood marker.
Did the study rule out inflammation?
No. It ruled against a strong, easily detectable difference in the measured peripheral markers at one time point. Central inflammation, immune-cell function, vascular mechanisms, autonomic dysfunction, and metabolic changes remain separate questions.
How should clinicians read a normal inflammation panel in long-COVID fatigue?
Routine inflammatory markers may be poor triage tools for long-COVID fatigue severity. A patient can have disabling fatigue even when CRP, TNF-α, IL-6, and related blood markers look unremarkable.
References
- Omdal R, et al. Persistent fatigue in long-COVID is not associated with peripheral inflammatory or cellular stress biomarkers. Brain, Behavior, and Immunity – Health. 2026. doi:10.1016/j.bbih.2026.101226
- Ceban F, Ling S, Lui LMW, et al. Fatigue and cognitive impairment in post-COVID-19 syndrome: a systematic review and meta-analysis. Brain, Behavior, and Immunity. 2022;101:93-135. doi:10.1016/j.bbi.2021.12.020
- Montoya JG, Holmes TH, Anderson JN, et al. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proceedings of the National Academy of Sciences. 2017;114:E7150-E7158. doi:10.1073/pnas.1710519114
- Druce KL, Jones GT, Macfarlane GJ, Basu N. Patients receiving anti-TNF therapies experience clinically important improvements in RA-related fatigue. Rheumatology. 2022. doi:10.1093/rheumatology/keab837