
A 2026 analysis followed 161 people with cancer for 9 months to evaluate whether 2 forms of online mindfulness-based cognitive therapy reduced psychological distress: therapist-led group-blended care and individual self-guided modules. Psychological distress improved significantly in both formats, but fewer participants dropped out when the program included therapist-led group sessions.
Research Highlights
- Distress improved through 9 months: Badaghi et al. followed 161 people with cancer who received online mindfulness-based cognitive therapy (MBCT), a structured program that trains attention, decentering, and self-compassion for distress management.1
- 2 online formats improved outcomes: group-blended MBCT and individual-unguided MBCT reduced psychological distress, fear of cancer recurrence, rumination, and fatigue while improving mindfulness skills, decentering, and self-compassion.
- Format did not clearly change symptom benefit: time-by-intervention tests were non-significant across 8 outcomes, meaning the analysis did not show a reliable advantage for group-blended vs. unguided delivery on symptom change.
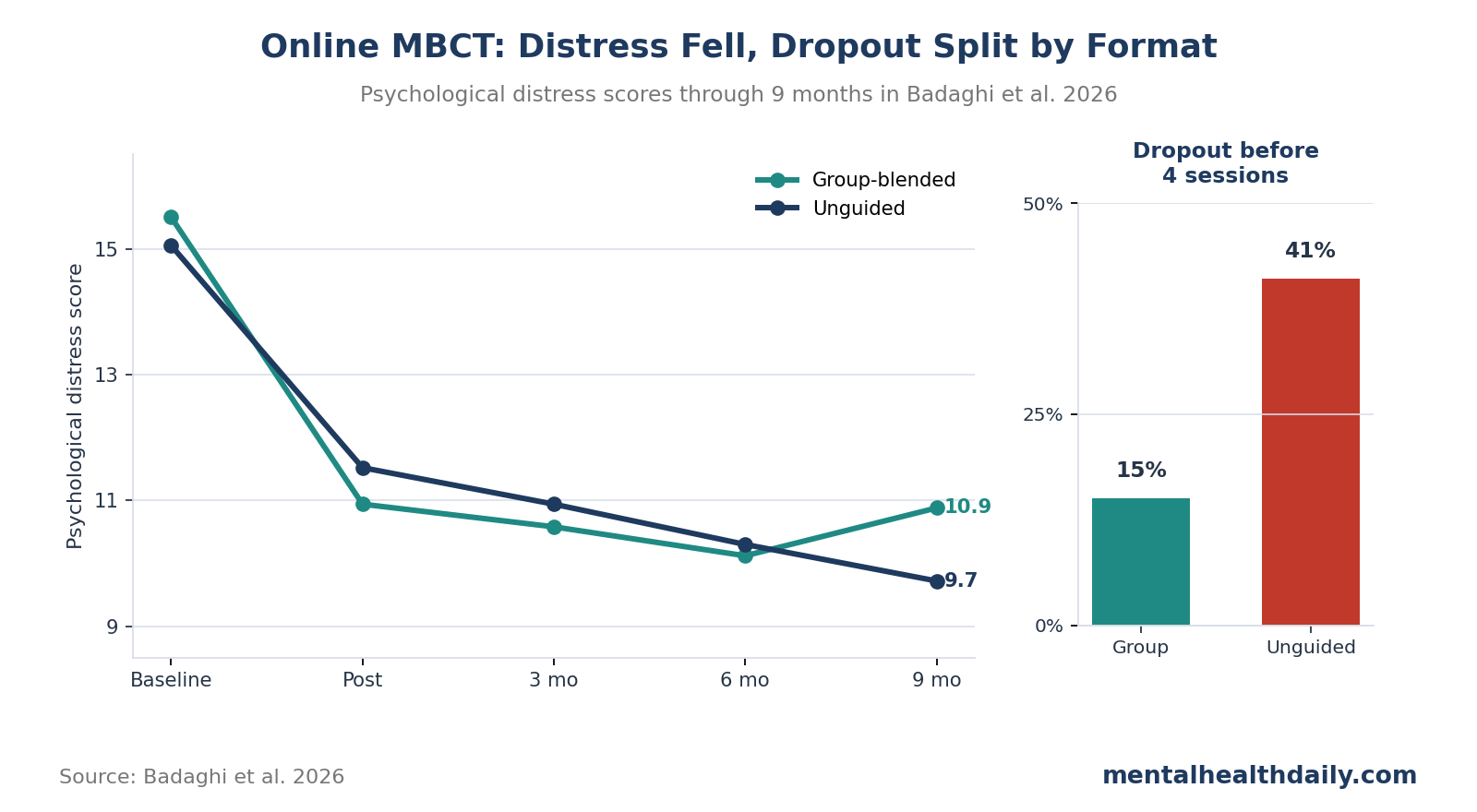
- Dropout separated the formats: 15% of group-blended participants dropped out before 4 sessions compared with 41% of individual-unguided participants, a major implementation signal even when symptom trajectories looked similar.
- Evidence strength is useful but exploratory: this was a 9-month secondary analysis with substantial attrition and no power calculation for moderator tests, so it supports durability and feasibility questions more than definitive format selection.
Based on these results, online MBCT can reduce cancer-related distress for people who engage with it, but a self-guided program may lose more participants before the therapeutic dose arrives.
161 Participants Tested 2 Online MBCT Formats
Mindfulness-based cognitive therapy is a structured psychological program that teaches people to notice thoughts, body sensations, and emotions as changing mental events rather than immediate threats that must be solved or avoided. It uses guided meditation, attention training, cognitive therapy exercises, and home practice to build decentering — the ability to step back from thoughts without treating them as facts.
In cancer care, MBCT does not target cancer biology itself. It targets the mental load around diagnosis, treatment, recurrence fear, fatigue, rumination, and the loss of ordinary control that can persist after oncology visits end.
Proposed distress mechanism: MBCT is expected to reduce distress by making rumination less automatic, helping patients tolerate uncomfortable sensations, and improving recovery when fear or fatigue pulls attention into a threat loop.
Badaghi et al. analyzed long-term outcomes from people with cancer who had been randomized to 1 of 2 online MBCT formats.1 The group-blended format mixed online content with therapist-led group sessions. The individual-unguided format delivered the program through self-guided online modules.
The final long-term sample included 161 participants: 71 in group-blended MBCT and 90 in individual-unguided MBCT. The sample was 80% female, 48% had breast cancer, 77% were receiving or had completed treatment with curative intent, and mean age was 52.8 years.
The outcomes covered more than one distress score:
- Psychological distress: the primary mental-health outcome.
- Fear of cancer recurrence: worry that cancer will return or progress.
- Rumination: repetitive negative thinking that keeps distress active.
- Fatigue: cancer-related tiredness severe enough to affect daily functioning.
- Mindfulness skills, decentering, and self-compassion: process measures that reflect whether participants learned the psychological skills MBCT tries to build.
Distress Scores Stayed Lower at 9 Months
Distress scores: both formats showed significant improvement from baseline to 9-month follow-up across primary and secondary outcomes. In the group-blended arm, psychological distress fell from a mean of 15.50 at baseline to 10.88 at 9 months. In the individual-unguided arm, distress fell from 15.05 to 9.72.
Effect-size caution: Cohen’s d, a standardized mean difference showing change in standard-deviation units, was 0.73 for group-blended psychological distress and 0.83 for individual-unguided psychological distress. Those are clinically meaningful within-group changes, though within-group effects cannot by themselves prove how much of the improvement came from MBCT rather than time, selection, or continued care.
Secondary outcomes: fear of recurrence also improved. Group-blended scores moved from 77.84 to 64.76, while individual-unguided scores moved from 77.06 to 67.00. Fatigue severity fell from 37.12 to 29.19 in the group-blended arm and from 35.51 to 29.94 in the unguided arm.
Process measures moved in the expected direction too: mindfulness skills, decentering, and self-compassion improved, which makes the symptom change more coherent than a distress-score drop alone.
Unguided Delivery Had Higher Dropout
Symptom comparison: symptoms improved similarly in the 2 online formats, while retention separated them more clearly. The time-by-intervention tests were non-significant for psychological distress, fear of recurrence, fatigue, rumination, mindfulness skills, decentering, self-compassion, and well-being. In plain terms, the analysis did not show a reliable symptom-change advantage for either delivery format.
Dropout definition: dropout was defined as attending fewer than 4 of 8 sessions, the threshold the researchers treated as the minimum meaningful dose. Overall, 48 of 161 participants dropped out before that point. Dropout was 11 of 71 in group-blended MBCT, or 15%, compared with 37 of 90 in individual-unguided MBCT, or 41%.
Implementation tradeoff: unguided online care may be cheaper and easier to scale, but the higher dropout rate shows the cost of removing therapist and group contact. Self-guided modules place more burden on the patient to initiate sessions, persist through difficult weeks, and translate exercises into daily life. Group contact adds scheduling friction, but it also adds accountability, social presence, and therapist scaffolding.
Distress and dropout: highly distressed participants were more likely to discontinue group-blended MBCT than lower-distress participants in that arm. Psychological distress did not predict dropout in the unguided arm. This was an exploratory finding, but it cautions against a lazy rule that “more distressed patients need groups.” Some patients may benefit from therapist contact; others may find group participation burdensome when distress is high.
Rumination and Low Self-Compassion Predicted Larger Gains
Predictor pattern: higher baseline rumination predicted greater distress reduction over time. Lower baseline mindfulness skills and lower self-compassion also predicted larger distress reductions. Decentering, cancer diagnosis, age, sex, treatment intent, and time since diagnosis did not predict distress improvement over the follow-up window.
Mechanism fit: the biggest gains may appear when online MBCT targets an active problem: repetitive thinking, difficulty stepping back from thoughts, and harsh self-evaluation during illness. Those are exactly the processes MBCT is designed to train.
Adjacent evidence: the broader cancer mindfulness literature also supports durable distress reduction. Cillessen et al. previously synthesized randomized trials of mindfulness-based interventions for cancer patients and survivors and found benefits across psychological and physical health outcomes.2 Compen et al. reported that face-to-face and internet-based MBCT reduced psychological distress in a multicenter randomized trial.3 Wang et al. later found web-based mindfulness interventions improved several cancer-related outcomes across meta-analyses.4
Format interpretation: the Badaghi et al. analysis adds durability and format nuance. It does not overturn the broader mindfulness literature. It says that online delivery can preserve benefit through 9 months, while adherence and patient fit remain central design problems.
Limitations of This Long-Term Analysis
Secondary analysis: the long-term and moderator questions were not the primary endpoint of the original 3-arm randomized trial. They are informative, but they should be read as follow-up evidence rather than a definitive format-selection trial.
Attrition was substantial: by 9 months, outcome counts were lower than baseline counts. For psychological distress, the 9-month analysis included 43 group-blended participants and 53 unguided participants.
No care-as-usual arm remained in the long-term comparison: participants initially assigned to care as usual were later rerandomized into the 2 MBCT formats if they were willing. That helps answer format questions, but it limits long-term comparison against no MBCT.
Moderator power was limited: the researchers explicitly noted that no power calculation was conducted for long-term effects or moderation analyses. Small or moderate format-by-patient-profile differences could have been missed.
The sample was not all cancer patients: most participants were women, nearly half had breast cancer, and most were treated with curative intent. Results may differ in advanced cancer, lower-resource settings, men with cancer, or patients with severe depression, cognitive impairment, or major treatment toxicity.
Questions About Online MBCT for Cancer Distress
Why test online MBCT in cancer care?
Online mindfulness-based cognitive therapy can deliver meditation, attention training, decentering, and self-compassion skills without requiring repeated clinic visits. In this 161-person cancer sample, both online formats reduced distress through 9 months.
Did group sessions work better than unguided online modules?
The analysis did not show a reliable symptom-change advantage for group-blended delivery over individual-unguided delivery. Both formats improved distress through 9 months.
Dropout differed sharply. Group-blended delivery had lower early dropout, while unguided delivery lost more participants before 4 sessions.
Who might benefit most?
Participants with more rumination, lower mindfulness skills, and lower self-compassion at baseline tended to show larger reductions in distress. That fits MBCT’s focus on repetitive thinking, self-criticism, and how people relate to difficult thoughts.
Can online MBCT replace oncology mental-health care?
Online MBCT is better viewed as one scalable support option. Patients with severe depression, suicidality, trauma symptoms, complex medication issues, or major functional impairment still need individualized mental-health assessment and care.
References
- Long-Term Outcomes, Moderators, and Predictors in Online Mindfulness-Based Cognitive Therapy for People With Cancer: Secondary Analysis of a Randomized Controlled Trial. Badaghi N et al. Journal of Medical Internet Research. 2026;28:e79928. doi:10.2196/79928
- Mindfulness-Based Interventions for Psychological and Physical Health Outcomes in Cancer Patients and Survivors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Cillessen L et al. Psycho-Oncology. 2019;28(12):2257-2269. doi:10.1002/pon.5214
- Face-to-Face and Internet-Based Mindfulness-Based Cognitive Therapy Compared With Treatment as Usual in Reducing Psychological Distress in Patients With Cancer: A Multicenter Randomized Controlled Trial. Compen F et al. Journal of Clinical Oncology. 2018;36(23):2413-2421. doi:10.1200/JCO.2017.76.5669
- Effectiveness of Web-Based Mindfulness-Based Interventions for Patients With Cancer: Systematic Review and Meta-Analyses. Wang T et al. Journal of Medical Internet Research. 2024;26:e47704. doi:10.2196/47704
- Effectiveness of Online Mindfulness-Based Interventions for Cancer Patients: A Systematic Review and Meta-Analysis. Fan M et al. Japanese Journal of Clinical Oncology. 2023;53(11):1068-1076. doi:10.1093/jjco/hyad101
- Positive Health Outcomes of Mindfulness-Based Interventions for Cancer Patients and Survivors: A Systematic Review and Meta-Analysis. Badaghi N et al. Clinical Psychology Review. 2024;114:102505. doi:10.1016/j.cpr.2024.102505