A 2026 medRxiv preprint found that 10 severe obsessive-compulsive disorder patients treated with anterior-limb-of-internal-capsule DBS had a 42.9% average Y-BOCS symptom decrease over 6 months while alpha-band activity in the anterior globus pallidus externus fell.1 The strongest read is a response-marker signal: GPe alpha decreased during effective OCD DBS, but the sample is too small to treat the signal as a programming rule.
Research Highlights
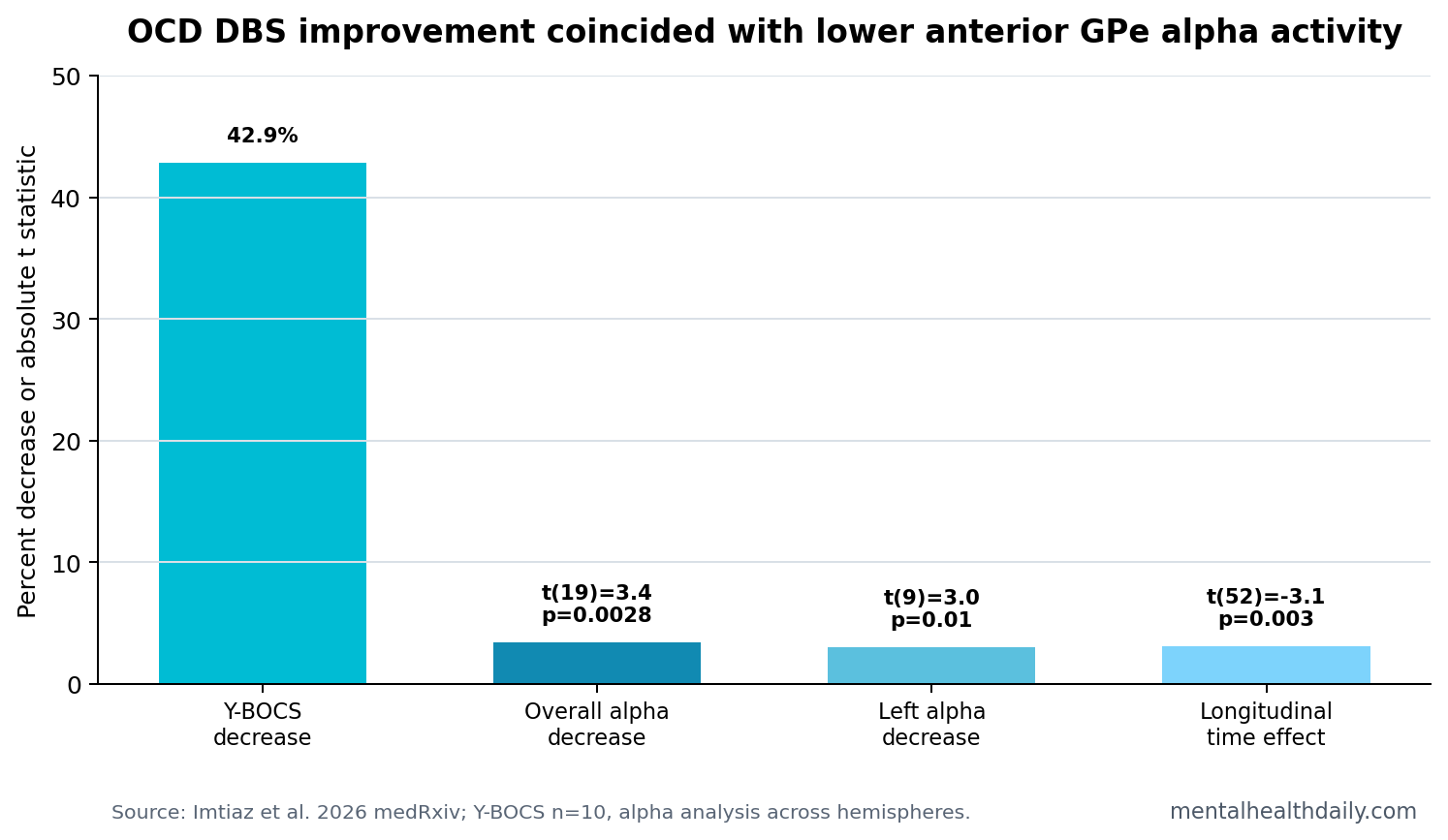
- OCD symptoms decreased: mean Y-BOCS fell from 30.1 ± 4.4 at baseline to 17.0 ± 5.1 after 6 months, a 42.9% decrease, p = 5.8 x 10−5.1
- Alpha power decreased: GPe alpha-band activity declined across hemispheres, t(19) = 3.4, 95% CI 0.19 to 0.80, p = 2.8 x 10−3.1
- Specificity looked symptom-linked: BDI and BAI scores did not substantially change at 6 months, while the OCD-specific Y-BOCS did.1
- The nonresponder was informative: the only patient without a Y-BOCS decrease also never showed alpha decrease in either hemisphere during the 6-month follow-up.1
- Evidence remains preliminary: this was a 10-patient 2026 preprint with 1 complete nonresponder, not a validated closed-loop OCD DBS biomarker.
Obsessive-compulsive disorder (OCD) involves intrusive thoughts, urges, or images and repetitive behaviors or mental rituals meant to reduce distress. Severe refractory OCD can be disabling enough that deep brain stimulation becomes a consideration after standard medication and psychotherapy options fail.
Deep brain stimulation (DBS) uses implanted electrodes to deliver electrical pulses to a target circuit. Imtiaz et al. stimulated dorsal contacts in the anterior limb of the internal capsule (ALIC), a white-matter route linked to OCD improvement, while recording local field potentials from ventral contacts located in the anterior globus pallidus externus (GPe), a gray-matter node in the indirect corticostriatal pathway.
Y-BOCS Scores Fell 42.9% Over 6 Months of ALIC DBS
The Yale-Brown Obsessive Compulsive Scale (Y-BOCS) is the standard clinician-rated severity scale for OCD symptoms. In the 2026 cohort, mean baseline Y-BOCS was 30.1 ± 4.4, consistent with severe symptoms. After 6 months of active DBS, mean Y-BOCS was 17.0 ± 5.1.1
Magnitude: average Y-BOCS decreased 42.9%, with paired t(9) = 7.1, 95% CI 8.9 to 17.3, p = 5.8 x 10−5. In contrast, Beck Depression Inventory and Beck Anxiety Inventory scores did not show substantial 6-month change. That pattern suggests the clinical effect was more OCD-specific than a broad mood/anxiety improvement.
Anterior GPe Alpha Activity Decreased After Treatment
Alpha-band activity refers to rhythmic neural power around 7 to 12 Hz. Alpha rhythms are not automatically good or bad; the meaning depends on the circuit, task, disease, and recording site. Here, the question was whether alpha-band power in the anterior GPe changed during clinically effective ALIC DBS.
Across baseline and 6-month recordings, alpha activity decreased significantly, t(19) = 3.4, 95% CI 0.19 to 0.80, p = 2.8 x 10−3. Hemisphere-specific analysis found decreases in both hemispheres, but only the left hemisphere reached conventional significance: t(9) = 3.0, 95% CI 0.16 to 1.12, p = 0.01. The right hemisphere result was t(9) = 1.8, p = 0.1.1
Removing the single patient who did not clinically improve made the alpha decrease larger: t(17) = 4.0, 95% CI 0.27 to 0.89, p = 9.3 x 10−4. That is biologically coherent, but it also shows why larger samples with more nonresponders are needed. A biomarker cannot be validated on one negative case.
GPe Recordings Put the Indirect Pathway in the OCD DBS Story
The globus pallidus externus is part of the basal ganglia, a set of circuits involved in action selection, inhibition, habits, and behavioral control. In OCD, indirect-pathway models are attractive because compulsive rituals can be understood partly as difficulty suppressing repetitive action or thought loops.
Prior DBS evidence already points beyond a single target. Subthalamic nucleus stimulation reduced severe OCD symptoms in earlier work, and ventral capsule/ventral striatum or BNST sensing studies have reported low-frequency oscillatory changes in responders.2,3 The 2026 paper adds anatomical specificity by using a consistent ALIC stimulation strategy while recording from anterior GPe gray matter.
- Stimulation target: ALIC white matter at a tractographic network target derived from prior DBS responders.
- Recording target: ventral DBS contacts anchored in anterior GPe gray matter.
- Candidate signal: alpha-band power that fell during clinical improvement.
Intermediate Time Points Linked Alpha Change to Y-BOCS Change
The researchers also examined available intermediate time points between baseline and 6 months. About 85% of bimonthly time points had both clinical and neural data. Alpha power changed over time, t(52) = −3.1, p = 3 x 10−3. Adding Y-BOCS to the model showed a relationship between alpha-power change and Y-BOCS change, t(51) = 2.1, p = 0.04.1
Longitudinal logic: a useful biomarker should move with symptom change over time, in addition to differing before and after treatment. This preprint provides an early version of that evidence, but not enough to define a patient-level threshold.
10 Patients and 1 Nonresponder Keep the Biomarker Preliminary
Evidence-strength note: this was a small preprint in a specialized surgical cohort. It can support the hypothesis that anterior GPe alpha power is a DBS response marker in OCD. It cannot prove that clinicians should adjust stimulation based on alpha power, that GPe alpha works across implant strategies, or that the signal predicts response before symptoms improve.
The main next step is not more broad speculation about the basal ganglia. It is a larger, prespecified sensing study that includes enough responders and nonresponders to test whether alpha power predicts clinical course, distinguishes relapse from noise, and changes when stimulation settings are modified.
Still, the result is useful. OCD DBS research needs readouts that are closer to circuit function than a monthly symptom score. GPe alpha activity is now a concrete candidate, especially because the only complete clinical nonresponder showed the opposite electrophysiology pattern.
Why the Nonresponder Cannot Carry the Whole Biomarker Claim
The single nonresponder is scientifically interesting because the clinical and electrophysiological patterns lined up: no Y-BOCS decrease and no alpha decrease. That observation makes the response-marker hypothesis more coherent. It does not validate the marker, because 1 nonresponder cannot define the false-positive rate, false-negative rate, or threshold behavior of the signal.
A clinically useful OCD DBS marker would need to answer harder questions. Does alpha fail to decrease before clinicians know treatment is not working? Does alpha rise before relapse? Does alpha change when stimulation settings are adjusted? Does medication change alpha independently of OCD symptoms? Does provoked obsession, stress, sleep loss, or electrode impedance produce misleading shifts?
Validation standard: the next cohort needs enough nonresponders and partial responders to test prediction, thresholds, and false alarms. Without that, the marker remains a mechanistic clue and a candidate programming aid rather than a clinical control signal.
ALIC Stimulation and GPe Recording Tie White Matter to Gray Matter
The implant strategy is a major reason the paper is more specific than a broad DBS outcome report. Stimulating the ALIC targets white-matter pathways, while recording from anterior GPe gives a gray-matter readout from a connected basal-ganglia node. That pairing lets the study ask whether network-level treatment produces a measurable change inside the indirect pathway.
Indirect pathway is shorthand for a basal-ganglia route that helps suppress actions or action tendencies. In OCD, that route is relevant because compulsions can be understood partly as repetitive action plans or mental routines that are difficult to inhibit. The GPe is not the whole OCD circuit, but it is a plausible place to look for a physiological trace of restored inhibitory control.
- White-matter intervention: ALIC stimulation engages fibers connected to frontal, subcortical, and limbic nodes.
- Gray-matter readout: GPe LFPs measure local rhythmic activity rather than only electrode location.
- Network hypothesis: symptom improvement should coincide with changed activity in a connected node along with current delivery at the lead tip.
That network framing also explains why the finding should be replicated across targets. If GPe alpha is a general OCD response marker, it should appear in related DBS strategies. If it is specific to this ALIC-GPe geometry, the marker may be useful but narrower.
Programming implication: alpha should be treated as a candidate readout to test prospectively, not as a current rule for changing stimulation.
Clinical programming would need thresholds, artifacts checks, symptom anchors, and replication across implant centers.
Questions About OCD DBS and GPe Alpha
Does lower GPe alpha mean OCD is improving?
Not by itself. In this 10-patient cohort, alpha decreased during clinical improvement, but the signal has not been validated as an individual treatment rule.
Why did the researchers record from GPe while stimulating ALIC?
The lead trajectory allowed dorsal contacts to stimulate ALIC white matter and ventral contacts to record from anterior GPe gray matter. That made it possible to observe a basal-ganglia node while treating a connected white-matter pathway.
What would make this biomarker clinically useful?
Prospective validation would need to show that alpha changes predict response, relapse, or programming needs before ordinary clinical assessment can, across multiple centers and implant strategies.
References
- Imtiaz SA, et al. Globus pallidus externus (GPe) alpha band activity decreases after deep brain stimulation in clinically responsive obsessive-compulsive disorder patients. medRxiv. 2026. doi:10.64898/2026.04.10.26350428
- Mallet L, et al. Subthalamic nucleus stimulation in severe obsessive-compulsive disorder. New England Journal of Medicine. 2008. PubMed
- Provenza NR, et al. Sensing obsessive-compulsive disorder deep brain stimulation response through low-frequency neural activity. PubMed
- Arbab T, et al. Globus pallidus alpha activity during provoked compulsions in obsessive-compulsive disorder DBS patients. PubMed