
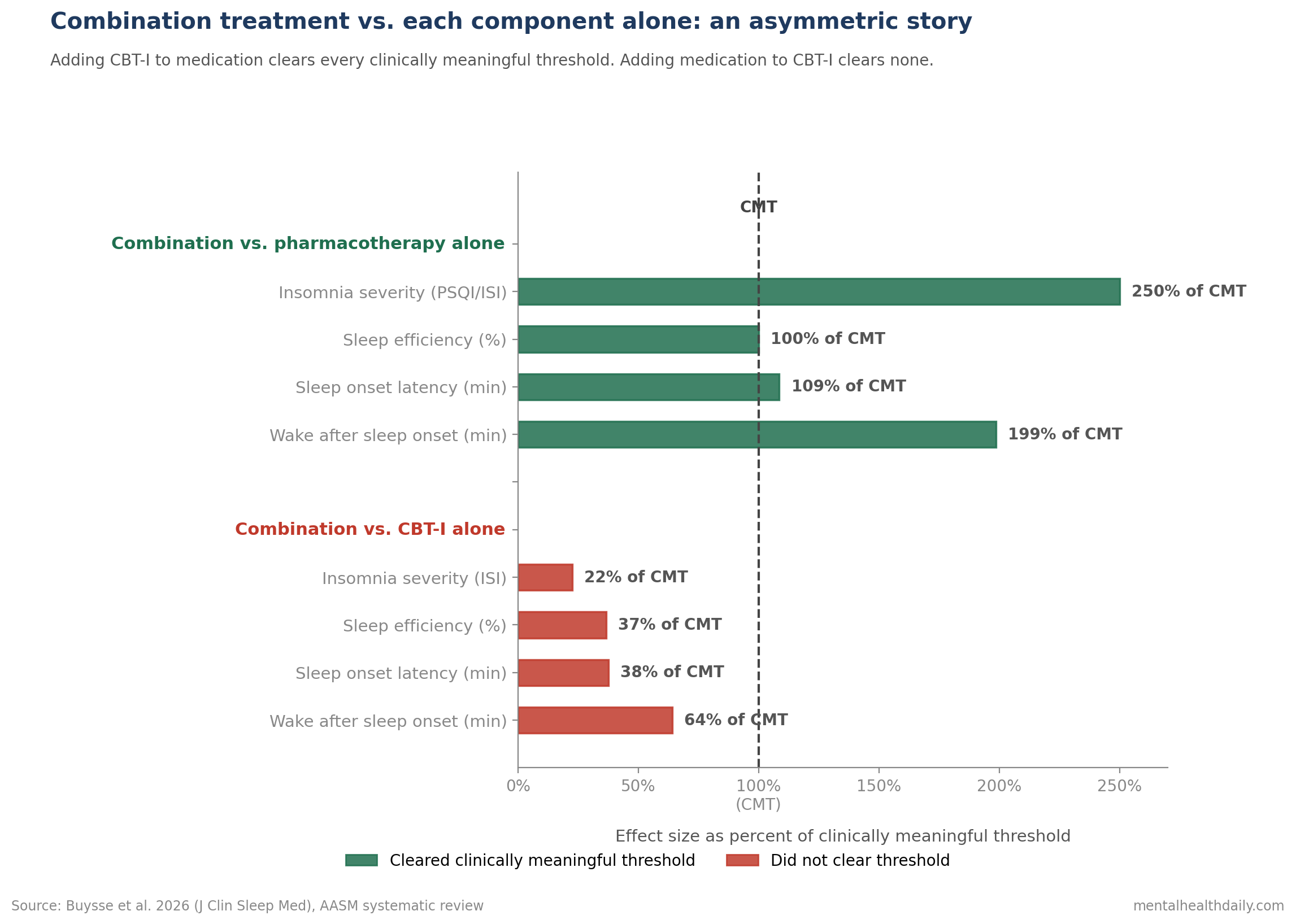
Patients with chronic insomnia frequently end up on both a sleep medication and cognitive behavioral therapy for insomnia (CBT-I), and a 2026 AASM meta-analysis of 15 RCTs from Buysse et al. found a clear asymmetry: adding CBT-I to medication helps, while adding medication to CBT-I adds little and may even worsen daytime depression scores.1
Research Highlights
- Combination beat pharmacotherapy alone on insomnia severity. SMD −0.67 (95% CI −0.97 to −0.36), translating to a 2.5-point improvement on the Pittsburgh Sleep Quality Index (CMT −1 point). Sleep efficiency rose 3.5%, sleep onset latency dropped 7.6 minutes, and wake after sleep onset dropped 13.9 minutes — all clinically meaningful.1
- Combination did NOT beat CBT-I alone on insomnia severity. SMD 0.10 (95% CI −0.17 to 0.37), an Insomnia Severity Index difference of 0.45 points (CMT −2 points). Sleep continuity outcomes also failed to reach the clinically meaningful threshold.1
- Adding meds to CBT-I produced higher post-treatment depression scores. Beck Depression Inventory was 2.1 points higher in the combination group (95% CI 0.54 to 3.67), and the SMD for daytime outcomes (0.39, 95% CI 0.10 to 0.68) reached statistical significance in the unfavorable direction.1
- Total sleep time modestly favored combination over CBT-I alone. MD +13.81 minutes (95% CI −6.78 to 34.41) at the +10 minute clinically meaningful threshold — a positive but uncertain effect.1
- GRADE certainty was low for most outcomes, downgraded primarily for risk of bias and imprecision. The strongest evidence is on combination beating pharmacotherapy alone for insomnia severity; the most novel finding is that combination does not improve on CBT-I alone.1
The Buysse review fits in a literature where CBT-I has, for a decade, been the standard-of-care first-line treatment for chronic insomnia.2,3 Sleep medications stay widely prescribed in routine practice, often before CBT-I is offered or while patients wait for access.
The previous AASM clinical practice guidelines covered behavioral and pharmacological treatments separately. Whether stacking them produces additive benefit, redundancy, or interference was the gap this review filled.
AASM 2026: 15 RCTs, Two PICO Comparisons, GRADE Certainty
The AASM task force searched PubMed and PsycINFO through June 2025, screened 1,179 articles, and identified 15 RCTs that met inclusion criteria.1
Two pre-specified PICO (Population, Intervention, Comparator, Outcome) questions structured the analysis:
- PICO 1: Combination treatment vs. pharmacotherapy alone — does adding CBT-I to a sleep medication beat the medication alone?
- PICO 2: Combination treatment vs. CBT-I alone — does adding a sleep medication to CBT-I beat CBT-I alone?
Critical outcomes included global insomnia severity (Insomnia Severity Index, Pittsburgh Sleep Quality Index), diary sleep continuity (sleep efficiency, sleep onset latency, wake after sleep onset), and daytime symptoms (depression, anxiety, fatigue, quality of life).
Each outcome had a pre-specified clinically meaningful threshold (CMT). For comparisons of combination treatment to a single active treatment, the CMT was set at half the placebo-comparison CMT, on the reasoning that incremental benefit over an already-active treatment is genuine but smaller.
Insomnia medications across the 15 RCTs included lormetazepam, temazepam, trazodone, zolpidem, and zopiclone — mostly benzodiazepine receptor agonists with one sedating antidepressant.
GRADE assessment was used to grade the certainty of evidence for each outcome (high, moderate, low, very low) based on risk of bias, imprecision, inconsistency, indirectness, and publication-bias risk.
Combination vs. Pharmacotherapy Alone: Adding CBT-I Helps
Six RCTs (n ≈ 178 in the global-severity analysis) compared CBT-I plus a sleep medication to that medication alone.1
The benefits clustered on the sleep outcomes:
- Global insomnia severity improved. SMD −0.67 (95% CI −0.97 to −0.36). Re-expressed in PSQI units, that is a 2.5-point lower score in the combination group (95% CI −3.64 to −1.35), well below the clinically meaningful threshold of −1 point.
- Sleep efficiency rose 3.5% (95% CI 0.23 to 6.89), at the CMT of +3.5%.
- Sleep onset latency dropped 7.6 minutes (95% CI −15.0 to −0.5), at the CMT of −7 minutes.
- Wake after sleep onset dropped 13.9 minutes (95% CI −27.4 to −0.9), well past the CMT of −7 minutes.
The pattern is consistent with what CBT-I trials show: behavioral and cognitive interventions improve sleep architecture and the subjective experience of insomnia in ways that medications alone don’t.4
Daytime outcomes did not reach the clinically meaningful threshold. The Beck Depression Inventory was 1.5 points lower in the combination group (95% CI −3.16 to 0.15) against a CMT of −2.5 points.
Total sleep time also missed the threshold (MD −15.48 minutes, 95% CI −43.63 to 12.67, CMT +10 minutes).
Side-effect data were thin (one study), with more reports of morning sleepiness in the combination group.
The task force judged the desirable benefits as small and the undesirable harms as minimal, and concluded combination treatment was preferred over pharmacotherapy alone for most patients.
Combination vs. CBT-I Alone: Adding Meds Adds Little
The second comparison is where the asymmetry shows up.
Six RCTs (n ≈ 228 for global severity) compared CBT-I plus a sleep medication to CBT-I alone.1
The sleep outcomes:
- Global insomnia severity: SMD 0.10 (95% CI −0.17 to 0.37). Re-expressed in ISI units, a 0.45-point difference (CMT −2 points) — functionally null.
- Sleep efficiency: +1.28% (95% CI −1.51 to 4.06; CMT +3.5%) — below threshold.
- Sleep onset latency: −2.63 minutes (95% CI −8.37 to 3.11; CMT −7 minutes) — below threshold.
- Wake after sleep onset: −4.48 minutes (95% CI −14.25 to 5.29; CMT −7 minutes) — below threshold.
None of the sleep outcomes cleared the clinically meaningful threshold. Adding a sleep medication to a CBT-I course does not, on average, improve insomnia severity or sleep continuity beyond what CBT-I produces alone.
Total sleep time was the one exception. MD +13.81 minutes (95% CI −6.78 to 34.41) at the +10 minute CMT — the point estimate clears the threshold but the confidence interval crosses zero.
Combination Treatment Raised Post-Treatment Depression Scores
Daytime mood signal: The most surprising finding involves daytime symptoms when meds are added to CBT-I.
The pooled SMD across daytime outcome instruments was 0.39 (95% CI 0.10 to 0.68) — a positive value here means the combination group did worse.1
Clinical scale translation: Re-expressed in BDI units, the post-treatment Beck Depression Inventory was 2.1 points higher in the combination group (95% CI 0.54 to 3.67) compared to CBT-I alone.
The CMT for the BDI in this comparison was −2.5 points. The combination group came in at +2.1, missing the threshold but in the unfavorable direction.
The certainty of evidence here was rated moderate — higher than for most other outcomes — meaning the depression effect is more robustly estimated than the sleep effects.
Plausible mechanisms: Two candidate explanations are reasonable. Sleep medications sometimes carry residual sedation and cognitive blunting effects that may show up on depression and fatigue scales. And patients on combination treatment may engage less actively with the cognitive and behavioral skills training in CBT-I if a medication is producing immediate sleep relief, dulling the long-term skill-building benefit.
The data don’t distinguish these mechanisms, but the directional signal — combination doing worse than CBT-I alone on daytime mood — is the kind of finding that should give clinicians pause before routinely adding a hypnotic to a CBT-I course.
Use Sleep Medication as an Add-On to CBT-I, Not the Other Way Around
The Buysse review’s central finding: CBT-I carries the effect, and medication adds little once CBT-I is in place.
- If a patient is already on a sleep medication, adding CBT-I provides clinically meaningful benefit. Insomnia severity, sleep efficiency, sleep onset, and wake after sleep onset all improved meaningfully when CBT-I was added to pharmacotherapy.
- If a patient is starting fresh, CBT-I alone is the better default. Adding a sleep medication does not measurably improve insomnia severity or sleep continuity beyond CBT-I, may produce worse depression scores, and adds the medication-related risks of dependence, daytime sedation, and rebound insomnia on discontinuation.
- If a patient is on long-term hypnotics and stable, transitioning to CBT-I-led care is supported by these data. The combination-vs-pharmacotherapy-alone comparison shows CBT-I addition meaningfully improves sleep outcomes, which positions a gradual taper plan for the medication once CBT-I is established.
- Cost considerations are real. CBT-I averages $100–$200 per session, typically across 4–8 sessions, vs. low monthly cost of generic hypnotics. The Buysse task force judged the additional cost of CBT-I as moderate but well-justified by the outcomes.
Low-Certainty RCTs Leave Tapering and Drug-Class Questions Open
Sequential vs. simultaneous combination was not tested directly. The 15 included RCTs all examined concurrent CBT-I + medication initiation. Real-world treatment more often involves sequential combinations — CBT-I started while a patient is already on medication, or medication added when CBT-I produces partial response. The data here don’t speak to those scenarios.
The medication mix is dominated by benzodiazepine receptor agonists. Lormetazepam, temazepam, zolpidem, and zopiclone account for most of the included data. Newer dual orexin receptor antagonists (suvorexant, lemborexant, daridorexant) and the FDA-approved low-dose doxepin were not represented in the meta-analyzable subset. Whether the asymmetry holds for these agents is untested here.
Long-term outcomes are sparse. Most studies measured outcomes immediately post-treatment, with follow-up periods limited. CBT-I’s known durability advantage at 12–24 months is not directly compared to combination treatment in this review.
Risk-of-bias and imprecision drove low GRADE certainty. Most outcomes were graded low certainty, meaning future RCTs could meaningfully change the effect estimates. The directional pattern is consistent across outcomes, but individual numerical effects should be read with that uncertainty in mind.
Questions About Combining CBT-I and Sleep Medication
Should I add CBT-I if I’m already taking a sleep medication?
The data clearly support adding CBT-I. Insomnia severity, sleep efficiency, sleep onset latency, and wake after sleep onset all improve meaningfully when CBT-I is added to a sleep medication.1
The combination cleared every clinically meaningful threshold for sleep outcomes in the AASM analysis. CBT-I addition is the strongest single recommendation that comes out of this review.
Should I add a sleep medication if I’m already in CBT-I?
The data do not support routinely adding medication to CBT-I. Sleep outcomes did not clear clinically meaningful thresholds, and the combination group had higher post-treatment depression scores (BDI +2.1 points, 95% CI 0.54 to 3.67).1
Some patients may need medication during the early weeks of CBT-I as a bridge, and that decision is reasonable in shared decision-making. The default expectation should not be that adding a hypnotic improves CBT-I outcomes.
Why might combination treatment be associated with higher depression scores?
Two plausible mechanisms: residual sedation and cognitive blunting from sleep medications can show up on depression and fatigue questionnaires; and immediate medication-driven sleep relief may reduce engagement with the skill-building components of CBT-I, weakening the long-term mood and cognitive benefits.1
The review does not directly test these mechanisms, but the moderate-certainty effect should give clinicians pause about adding hypnotics in patients with comorbid depression.
Which sleep medications were included?
Mostly benzodiazepine receptor agonists: lormetazepam, temazepam, zolpidem, and zopiclone. One study used trazodone (a sedating antidepressant). The newer dual orexin receptor antagonists (suvorexant, lemborexant, daridorexant) and low-dose doxepin were not represented.1 The combination-vs-CBT-I asymmetry may differ for these agents.
Is access to CBT-I a real constraint?
Yes. CBT-I-trained clinicians are concentrated in academic centers and large urban areas. Wait times of months are common in many settings. Digital CBT-I programs (Sleepio, SHUTi, others) have demonstrated efficacy and can fill this gap, though the Buysse review’s analyses focused on in-person CBT-I except for one self-help arm.1
References
- Combination treatment for chronic insomnia disorder in adults: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. Buysse DJ et al. Journal of Clinical Sleep Medicine. 2026;22(1):58. doi:10.1007/s44470-025-00039-7
- Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis. Trauer JM et al. Annals of Internal Medicine. 2015;163(3):191-204. doi:10.7326/m14-2841
- Behavioral and Psychological Treatments for Chronic Insomnia Disorder in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. Edinger JD et al. Journal of Clinical Sleep Medicine. 2021;17(2):255-262. doi:10.5664/jcsm.8986
- Comparative effectiveness of cognitive behavioral therapy for insomnia: a systematic review. Mitchell MD et al. BMC Family Practice. 2012;13:40. doi:10.1186/1471-2296-13-40
- European guideline for the diagnosis and treatment of insomnia. Riemann D et al. Journal of Sleep Research. 2017;26(6):675-700. doi:10.1111/jsr.12594
- Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. Sateia MJ et al. Journal of Clinical Sleep Medicine. 2017;13(2):307-349. doi:10.5664/jcsm.6470