
A 299-person remote randomized trial found that 10 min of daily focused-attention meditation reduced anxiety and mind wandering more than waitlist control, with the strongest gains among adults who started with higher internalizing symptoms.
Research Highlights
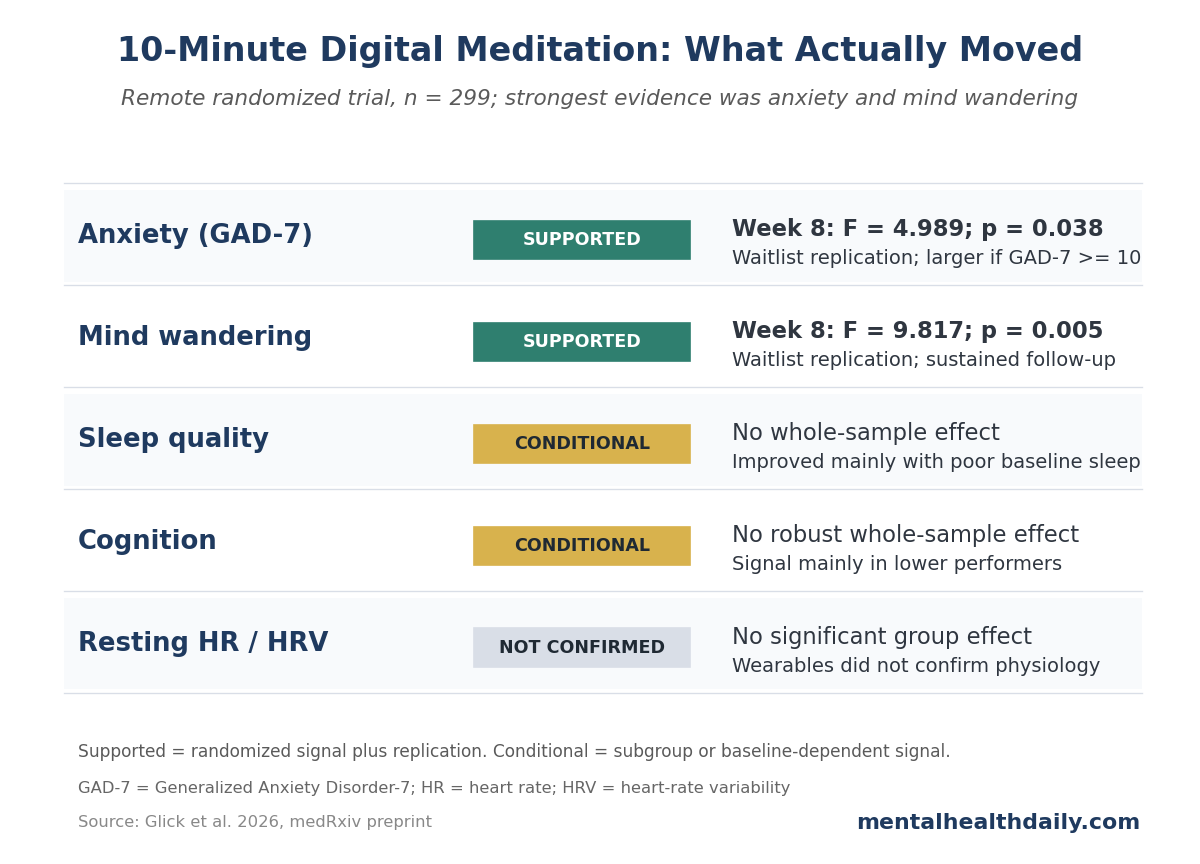
- Anxiety improved in the randomized phase: Glick et al. randomized 299 meditation-naive adults and found greater 8-week Generalized Anxiety Disorder-7 reduction with immediate meditation than with waitlist control (F = 4.989; p = 0.038).
- Mind wandering showed the clearer randomized signal: Mind Wandering Questionnaire scores fell more in the meditation arm than in the waitlist arm during the randomized phase (F = 9.817; p = 0.005), then replicated when waitlist participants received the same intervention.
- Baseline symptoms shaped response: participants with moderate or severe baseline anxiety had marked reductions after meditation (both p < 0.0001), while participants with minimal anxiety changed little.
- Cognition and physiology had weaker evidence than anxiety and mind wandering: Stroop and 2-back task improvements appeared mainly in lower-performing baseline quartiles, while resting heart rate and heart-rate variability did not show significant group-level effects.
- The evidence is promising but not clinical proof: this was a 299-person medRxiv preprint in undiagnosed adults, with waitlist control and substantial attrition, so it supports low-burden prevention more than treatment claims.
The result is useful but bounded: very brief digital meditation can move self-reported anxiety and attentional drift in a non-clinical sample. It is not yet evidence that a 10-min app-like protocol treats anxiety disorders or major depression.
The 2026 trial evaluated a focused-attention practice delivered remotely through brief instructor training, a mid-intervention check-in, and self-guided daily practice. Participants were asked to meditate for at least 10 min per day for 8 weeks inside a 16-week delayed-intervention design.
299 Adults Were Randomized to Immediate Meditation or Waitlist
Glick et al. assessed 681 people for eligibility and randomized 299 meditation-naive adults: 151 to immediate intervention and 148 to waitlist control. The primary analysis sample included 238 participants, with mean age 33.83 years and 154 women (66.7%).
Baseline symptom levels were mild on average, not clinical. Combined baseline Generalized Anxiety Disorder-7 (GAD-7; a 0-21 anxiety symptom scale) mean was 6.00 (SD 4.82). Baseline Pittsburgh Sleep Quality Index (PSQI; higher scores mean worse sleep quality) mean was 7.99 (SD 2.37), and baseline Mind Wandering Questionnaire (MWQ; higher scores mean more mind wandering) mean was 16.99 (SD 5.41).
Study snapshot:
- Randomized: 151 participants to immediate meditation and 148 to waitlist control.
- Analyzed: primary analysis sample of 238 participants.
- Practice dose: at least 10 min daily for 8 weeks.
- Follow-up structure: immediate-intervention participants were followed for another 8 weeks; waitlist participants later received the same intervention.
The design had 2 features that make the results more useful than a before-after meditation study:
- Randomized first phase: immediate meditation was compared with waitlist control from baseline to week 8.
- Internal replication: the waitlist group then received the same meditation training from week 8 to week 16, allowing within-participant replication.
The main tradeoff is the control condition. Waitlist control helps with randomization, but it does not fully match expectancy, instructor contact, daily structure, or the feeling of starting a self-improvement routine.
GAD-7 Anxiety Scores Fell More With Immediate Meditation
The primary psychological result was anxiety. During the randomized phase, immediate meditation produced greater GAD-7 reduction than waitlist control (F = 4.989; p = 0.038). When the waitlist group later received the intervention, anxiety decreased again within participants (t = −3.849; p < 0.001). The immediate-intervention group did not show rebound across the 8-week follow-up period.
The effect was not evenly distributed. Participants who started with moderate GAD-7 scores of 10-14 or severe scores of 15-21 had marked reductions after meditation (both p < 0.0001). Participants with minimal baseline anxiety had little room to improve and showed little change.
How to read the anxiety result:
- Best-supported claim: anxiety scores improved more with immediate meditation than with waiting during the first 8 weeks.
- Best-fit population: adults with at least moderate baseline anxiety symptoms, not people already near the floor of the scale.
- Overreach to avoid: treating this as proof that 10 min per day treats diagnosed generalized anxiety disorder.
Mind Wandering Improved More Clearly Than Sleep
Mind wandering was the second main signal. During the randomized phase, meditation reduced MWQ scores more than waitlist control (F = 9.817; p = 0.005). The delayed-intervention group replicated the effect after it received meditation (t = −4.146; p < 0.001), and reductions were sustained 8 weeks later in the immediate-intervention arm.
This fits the intervention better than many broad wellness claims. Focused-attention meditation trains repeated noticing and redirecting of attention. Reduced mind wandering is close to the mechanism the practice is designed to exercise.
Sleep was more conditional. Across the whole sample, PSQI change did not reach statistical significance. In stratified analyses, participants in the third and fourth quartiles of baseline sleep disturbance improved (p < 0.05), while those in the best baseline-sleep quartile had somewhat higher PSQI scores after intervention (p = 0.042).
- Mind wandering: randomized signal, delayed-arm replication, and sustained follow-up all pointed in the same direction.
- Sleep: improvement appeared mainly among participants who started with worse sleep.
- Mechanistic fit: attention training maps more directly onto mind wandering than onto sleep architecture.
Internalizing Symptoms Moved as a Single Latent Dimension
The most interesting analysis was not any one questionnaire. The researchers used exploratory factor analysis, a statistical method that looks for shared patterns across measures, and found a 2-factor structure explaining 42% of baseline variance.
The first factor, Internalization and Negative Affect, loaded positively on perceived stress, depressive symptoms, anxiety, rumination, and mind wandering, and negatively on quality of life and social connectedness. During the randomized phase, meditation reduced this factor more than waitlist control (F = 11.195; p = 0.002). The effect replicated in the delayed-intervention arm (t = −5.106; p < 0.001) and was sustained at follow-up.
The second factor, Resilience and Strength, did not show a consistent whole-sample effect. Participants in the lowest baseline quartile improved (t = 2.281; p = 0.02), but the broader pattern was weaker than the internalizing-symptom result.
The factor analysis gives the trial a more coherent shape:
- Internalizing symptoms moved: anxiety, stress, depressive symptoms, rumination, mind wandering, lower quality of life, and lower connectedness behaved like a linked symptom cluster.
- Strength traits did not broadly move: character-strength and resilience-related measures were not consistently changed across the whole sample.
- Baseline burden mattered again: people starting higher on the internalizing factor tended to show larger changes.
Cognitive and Wearable Outcomes Were Much Less Convincing
The study also measured Stroop and 2-back task performance through web-based cognitive testing. Whole-sample accuracy did not show robust between-arm differences during the randomized phase, and reaction times improved across both arms, a pattern consistent with practice effects from repeated testing.
The cognitive signal appeared mainly in participants with lower baseline performance. In the lowest-performing quartile, meditation exposure was associated with improved accuracy and reaction time on both Stroop and 2-back tasks (both p < 0.05). That is plausible, but it is subgroup evidence. It should not be advertised as broad cognitive enhancement.
Wearable-derived physiology was even weaker. Resting heart rate trended downward during meditation periods, but between-group differences were not statistically significant. Heart-rate variability also failed to separate meditation from control periods. The study therefore supports psychological change more strongly than autonomic re-regulation.
- Cognition: possible benefit among lower baseline performers; no robust whole-sample accuracy effect.
- Reaction time: improved across both meditation and control periods, which may reflect repeated-task practice.
- Wearables: resting heart rate and heart-rate variability did not confirm a strong physiological shift.
Brief Digital Meditation in the Anxiety Evidence Base
The broader meditation literature supports modest average benefits, with a lot of heterogeneity. Goyal et al. found mindfulness meditation programs produced moderate evidence of improved anxiety, depression, and pain, but the effects were not magical and comparisons against active treatments were less dramatic. Goldberg et al. reviewed 44 meta-analyses and concluded that mindfulness-based interventions have empirical support, while also warning that the evidence varies by comparison condition, population, and outcome.
The Glick et al. trial clarifies dose and delivery. Many meditation programs require 20-45 min sessions, multiweek classes, in-person groups, or intensive practice. This intervention asked for at least 10 min per day, delivered remotely, in meditation-naive adults.
Low burden affects adherence. A smaller intervention that people actually do may beat a theoretically stronger intervention that disappears after week 1.
Limitations of This Remote Meditation Trial
The paper was a preprint. It had not been certified by peer review at the time of the PDF. The data may hold up, but preprint status should lower confidence until review, correction, and possible revision.
The control group was waitlist, not active placebo. A waitlist comparison cannot fully separate meditation-specific effects from expectancy, attention, time structure, contact with study staff, or the simple act of starting a self-improvement routine.
Attrition was substantial. The trial randomized 299 people, while the primary analysis table listed 238 participants. Self-guided digital interventions often lose participants, and completers may be more motivated or more responsive than non-completers.
The sample was non-clinical. Participants were undiagnosed adults, many living in or near the San Francisco Bay Area. Results may not generalize to panic disorder, generalized anxiety disorder, major depression, severe insomnia, lower-resource populations, or people who dislike meditation.
Questions About 10-Minute Digital Meditation
Is 10 min per day enough to reduce anxiety?
In this trial, yes for self-reported anxiety in a non-clinical sample, especially among participants with higher baseline symptoms. The result should not be stretched into a claim that 10 min treats diagnosed anxiety disorders.
Did meditation improve depression?
Depressive symptoms improved mainly among participants with elevated baseline Patient Health Questionnaire-8 scores, but anxiety and mind wandering were the cleaner primary findings. The article should not be framed as a depression-treatment trial.
Did wearables confirm a physiological effect?
No firm physiological effect was shown. Resting heart rate moved directionally, but not significantly, and heart-rate variability did not distinguish meditation from control periods.
Who is most likely to benefit?
The trial points to people with higher baseline internalizing symptoms: more anxiety, rumination, mind wandering, stress, and lower quality of life. People starting near the healthy end of the scale had less measurable room to improve.
For most adults, a 10-min focused-attention practice is a low-risk experiment when anxiety, rumination, or mind wandering are mild-to-moderate problems. This trial does not show that meditation changes everything; it shows that a low-burden protocol can shift the internalizing-symptom cluster for people who start with enough symptoms to measure.
References
- Glick CC, Pirzada S, Quah S, et al. A fully remote randomized controlled trial of an ultra-brief digital meditation intervention reduces internalizing symptoms. medRxiv. 2026. doi:10.64898/2026.04.19.26351219
- Goyal M, Singh S, Sibinga EMS, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Internal Medicine. 2014;174(3):357-368. doi:10.1001/jamainternmed.2013.13018
- Goldberg SB, Riordan KM, Sun S, Davidson RJ. The empirical status of mindfulness-based interventions: a systematic review of 44 meta-analyses of randomized controlled trials. Perspectives on Psychological Science. 2022;17(1):108-130. doi:10.1177/1745691620968771
- Sevilla-Llewellyn-Jones J, Santesteban-Echarri O, Pryor I, McGorry P, Alvarez-Jimenez M. Web-based mindfulness interventions for mental health treatment: systematic review and meta-analysis. JMIR Mental Health. 2018;5(3):e10278. doi:10.2196/10278
- Rahl HA, Lindsay EK, Pacilio LE, Brown KW, Creswell JD. Brief mindfulness meditation training reduces mind wandering: the critical role of acceptance. Emotion. 2017;17(2):224-230. doi:10.1037/emo0000250
- Van Dam NT, van Vugt MK, Vago DR, et al. Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science. 2018;13(1):36-61. doi:10.1177/1745691617709589