Clozapine has been the most effective antipsychotic in schizophrenia for almost 40 years, yet it is still routinely held back until patients have failed multiple alternatives over many years — a “third-line, after years of failure” default that a 2026 Current Opinion review by Davani et al. argues is no longer supported by the evidence.1
Research Highlights
- Sequential trials show diminishing returns. First-line antipsychotic response is 53%; the second-line response drops to 26%. Switching to clozapine third-line yields 43% response, almost double the 26% from a third non-clozapine antipsychotic. In first-episode psychosis the gap widens further: 45% with clozapine vs. 15% with another antipsychotic.1
- Switching to clozapine after first relapse cuts the next relapse risk by 34%. In a Finnish nationwide cohort of 3,000 first-episode patients, clozapine after first relapse produced an adjusted hazard ratio (aHR) of 0.66 (95% CI 0.49–0.89), with 2-year relapse rates of 57.1% on clozapine vs. 73.2% on continued non-clozapine treatment.1
- Starting clozapine within 3 years of first episode improves negative symptoms and functioning relative to delayed clozapine. Earlier initiation was associated with higher negative-symptom remission (exp[B] = 0.38, p = 0.02) and higher Global Assessment of Functioning scores (β = 0.12, p = 0.046). Positive symptoms responded regardless of timing.1
- Real-world delays are measured in years. Mean time from first episode to clozapine in routine care: 9.81 years. Average delay after meeting treatment-resistance criteria: 47.7 months. In specialized early-intervention services, the same delay drops to 55 days.1
- Only 7.8% of patients receive clozapine despite 30.2% meeting eligibility criteria. The bottleneck is implementation, not evidence. The FDA’s November 2024 elimination of the clozapine REMS monitoring program removes one of the largest practical barriers.1
Clozapine has carried a “drug of last resort” reputation since Kane et al.’ 1988 trial established it as superior to chlorpromazine in patients who had failed other antipsychotics.2 That reputation is partly a side-effect story (agranulocytosis — a severe and potentially fatal drop in white blood cells — was the original reason for monitoring requirements).
It is also partly a system story. Specialized clinics, blood-monitoring infrastructure, and prescriber comfort with the drug all need to be in place before earlier prescribing becomes routine.
The Davani synthesis lands in a literature where the case for “earlier” has been quietly building for a decade. Its contribution is to lay the recent evidence side-by-side with the implementation gap.
Davani 2026: Six Studies, Five Years of First-Episode Data
The review is a scoping review — a structured synthesis that maps available evidence rather than pooling effect sizes formally — covering 6 studies that met inclusion criteria from 130 records screened.1
The included studies span:
- Two observational cohorts on real-world clozapine use in first-episode and early-phase samples (Pechuán et al. 2024, n = 255; Muñoz-Manchado et al. 2024, n = 254).
- One Finnish population-based registry study (Taipale et al. 2025, n = 3,000) comparing treatment strategies after first relapse.
- Two systematic reviews of treatment response, including one specifically on sequential antipsychotic trials in psychosis (O’Donoghue et al. 2024, n = 2,522).
- One umbrella review — a review of meta-analyses — on early-onset psychosis (Salazar de Pablo et al. 2024, n = 25,983, mean age 15.1 years).
The clinical question the review answers is narrow: what happens when clozapine is moved earlier in the treatment sequence in early-stage schizophrenia? The answer is consistent across study designs.
Sequential Antipsychotic Trials Have Sharply Diminishing Returns
The headline data point in the review comes from O’Donoghue et al.’s systematic review of sequential antipsychotic trials.1
Response rates fall steeply with each successive trial of a non-clozapine antipsychotic:
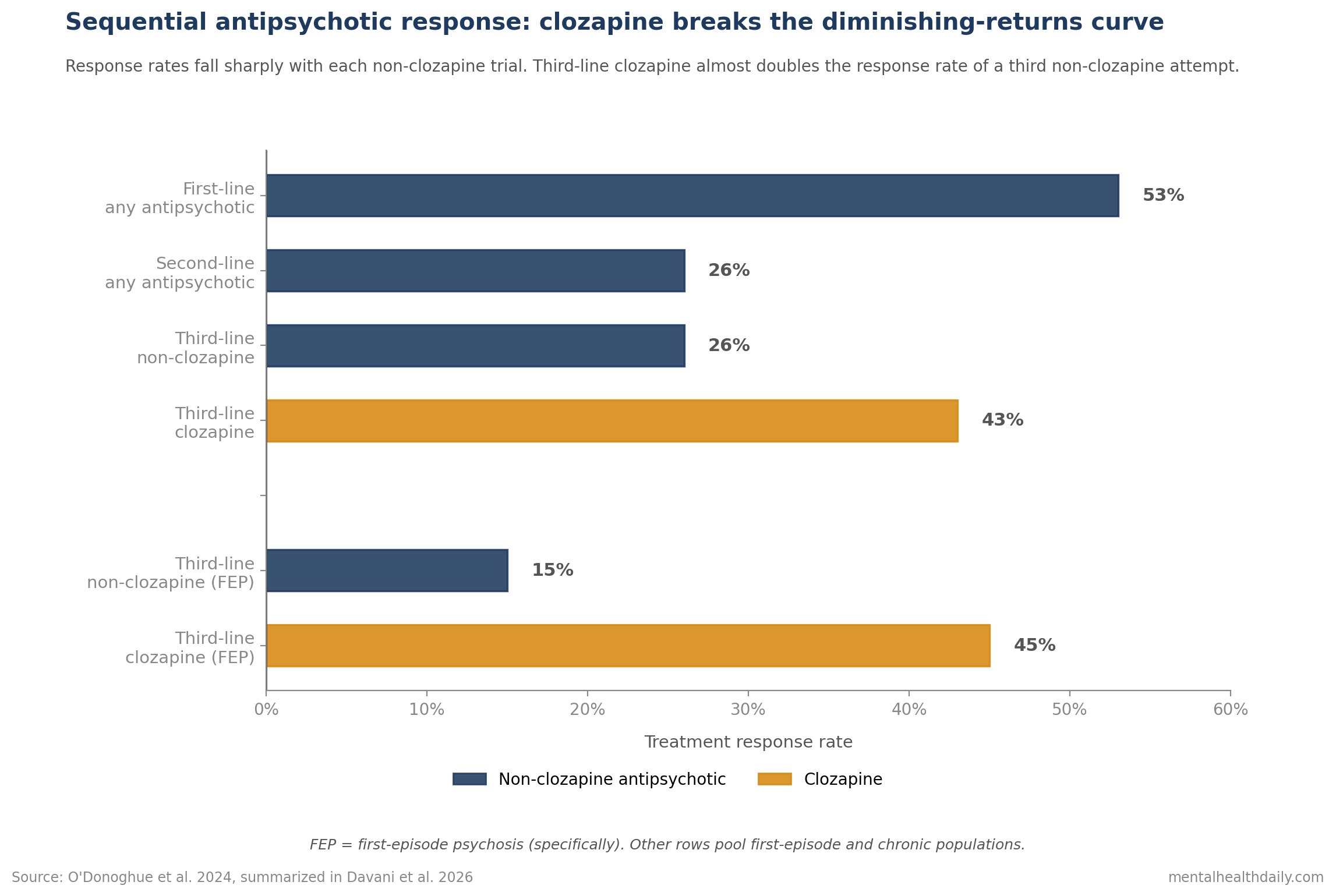
First-line response: 53% (95% CI 0.38–0.68). Most patients improve on the first antipsychotic they are given.
Second-line response: 26% (95% CI 0.15–0.39). Half the response rate of first-line.
Third-line non-clozapine response: 26% (95% CI 0.05–0.54). Switching to yet another second-generation antipsychotic produces no further gain on average.
Third-line clozapine response: 43% (95% CI 0.19–0.69) — nearly double the third-line non-clozapine rate.
In first-episode psychosis specifically the difference is even starker: third-line clozapine reached 45% response (95% CI 0.0–0.97) vs. about 15% for non-clozapine alternatives.1
The implication is direct. Once a patient has failed two non-clozapine antipsychotics, a third non-clozapine attempt has roughly a 1-in-4 chance of working. Clozapine has roughly a 1-in-2 chance.
This is the diminishing-returns curve that Howes et al.’ Treatment Response and Resistance in Psychosis (TRRIP) consensus guidelines have been pointing at since 2017 as the basis for defining treatment-resistant schizophrenia (TRS) at “failure of 2 adequate trials.”3
The 3-Year Window: Negative Symptoms and Functioning Respond Better
Early initiation widens the response on a different axis: it changes which symptom domains improve, with the largest gains in the symptoms that are usually hardest to treat.
The Muñoz-Manchado et al. 2024 cohort (n = 254 clozapine-treated patients, mean age at first episode 22.4 years) examined the timing-outcome relationship directly.1
When clozapine was started within 3 years of first episode:
- Negative symptom remission improved. exp(B) = 0.38, p = 0.02. (exp(B) is the exponentiated regression coefficient, similar to an odds ratio — values below 1.0 mean lower remission with longer delay; here, the longer the delay, the worse the remission.)
- Global Assessment of Functioning (GAF) scores improved relative to delayed clozapine. β = 0.12, p = 0.046 in the regression of GAF on time-to-clozapine. A small but statistically reliable functional advantage for earlier initiation.
- Positive symptom remission was unaffected by timing. Voices and delusions respond to clozapine regardless of when in the illness it is started.
This is the part of the timing argument that matters most for long-term outcomes.
Negative symptoms (flattened affect, social withdrawal, motivational deficits) and functional decline are the symptom domains most resistant to standard antipsychotics, most predictive of long-term disability, and most likely to become entrenched if untreated.
The Salazar de Pablo et al. 2024 umbrella review extends this picture in early-onset psychosis. Clozapine produced a standardized mean difference (SMD) of 1.6 for overall symptoms — substantially larger than olanzapine (0.77) or risperidone (0.43), the two most-prescribed alternatives in early-stage care.1
An SMD of 1.6 is large by any standard in psychiatric drug trials. For comparison, most antidepressants produce SMDs between 0.2 and 0.4 vs. placebo.
Switching to Clozapine After First Relapse Cuts Risk 34%
Taipale et al.’ 2025 analysis of the Finnish nationwide registry (n = 3,000 first-episode schizophrenia patients with at least one relapse) is the strongest real-world data point in the review.1
Patients who switched to clozapine after first relapse had:
- 34% lower risk of a second relapse compared to staying on or switching between non-clozapine antipsychotics. Adjusted hazard ratio = 0.66, 95% CI 0.49–0.89.
- 2-year second-relapse rates of 57.1% on clozapine vs. 73.2% on continued non-clozapine monotherapy.
An adjusted hazard ratio (aHR) of 0.66 with a confidence interval that does not cross 1.0 means the data essentially rule out “no benefit” and confirm a sizeable effect on relapse prevention.
This finding lines up with Tiihonen et al.’ 2017 nationwide cohort, which found clozapine had the lowest risk of treatment failure and rehospitalization among 29,823 Finnish patients with schizophrenia followed for up to 20 years.4
The mechanism is straightforward. Each relapse is associated with worse functional outcomes, increased disability, higher all-cause mortality, and reduced likelihood of stable remission.1 A drug that prevents relapses prevents the cumulative damage of the illness course.
Why Clozapine Stays Underutilized: 7.8% Get It Despite 30.2% Meeting Criteria
The implementation gap is the part of the story that ought to embarrass the field.
The Pechuán et al. 2024 cohort of 255 first-episode patients in a specialized early-intervention service found:
- 30.2% met treatment-resistance criteria within 2 years of first episode.1
- Only 7.8% actually received clozapine in that timeframe.1
- The gap between “eligible” and “treated” is roughly 4-fold.
The Muñoz-Manchado et al. 2024 cohort puts a number on the delay itself.
Mean time from first episode to clozapine initiation in routine care: 9.81 years. Average delay specifically after a treatment-resistance diagnosis was made: 47.7 months.1
Compare that to the Pechuán cohort, where a specialized early-intervention service achieved a median time-to-clozapine of 55 days from first antipsychotic.1
Same drug, same monitoring requirements. The difference is service design.
Three barriers consistently appear in the literature:
- Monitoring infrastructure. Until November 2024, US clozapine prescribing required adherence to the FDA’s Risk Evaluation and Mitigation Strategy (REMS) program: regular absolute neutrophil count (ANC) testing to catch agranulocytosis early. The FDA eliminated the REMS program after an advisory committee found it obstructed access without improving safety outcomes. Routine ANC monitoring is still standard practice but no longer enforced as a federally tracked program.1
- Clinician hesitancy. Many psychiatrists never prescribe clozapine. Those who do often default to it only after multiple non-clozapine trials, in line with older consensus guidelines.
- Patient and family concerns. The “drug of last resort” framing means clozapine is sometimes presented to patients as the option you reach for when nothing else has worked — a framing that builds reluctance into the decision.
Earlier Clozapine Needs Monitoring Capacity, Not More Failed Trials
The Davani review’s central recommendation is to move clozapine from third-line to second-line in early-stage schizophrenia.
- After the first antipsychotic fails, clozapine should be on the table. The 26% response rate to a second non-clozapine antipsychotic vs. the prospect of clozapine’s larger response in the same patient population is the core risk-benefit calculation.
- After first relapse, clozapine is now backed by Finnish registry data showing a 34% reduction in next-relapse risk. Continuing or switching between non-clozapine antipsychotics after a relapse is a defensible default only if the patient explicitly declines clozapine.
- Within 3 years of first episode, the timing matters for negative symptoms and functioning. Delays past this window may mean foregoing the symptom domains where clozapine’s advantage is largest.
- Side effects are real and need to be discussed honestly. Sedation, hypersalivation, constipation, weight gain, and metabolic effects are common; agranulocytosis is rare (well under 1% with appropriate monitoring) but serious. Real-world discontinuation rates around 35% are partly side-effect-driven.1
- Specialized early-intervention services dramatically reduce delays. Where they exist, a 55-day initiation window replaces the 9.81-year routine-care default. Patients and families benefit from asking whether such a service is accessible.
What this review doesn’t change: clozapine remains the most effective antipsychotic for treatment-resistant cases, with the caveat that it requires more careful management than alternatives. The argument is not that more people should be on clozapine in absolute terms — it is that the people who clearly meet criteria should not have to wait 9 years to get it.
Evidence Gaps Remain Around Mortality, REMS Removal, and First-Episode Use
It is a scoping review, not a meta-analysis. The authors did not pool effect sizes formally or perform a risk-of-bias assessment, which limits how confidently effect estimates can be generalized.
Most included studies are observational. Randomized comparisons of early vs. delayed clozapine initiation remain rare. The one RCT included (Asenjo-Lobos et al. 2025, n = 63) compared clozapine to quetiapine in first-episode schizophrenia and found similar 8-week response (68% vs. 66%, RR 1.03, 95% CI 0.73–1.46) — a short follow-up that doesn’t capture relapse prevention.1
The biomarker layer is still emerging. The review highlights three biomarkers under active investigation: the Striatal Connectivity Index from resting-state fMRI for predicting non-response to first-line antipsychotics, MC4R genotype for antipsychotic-induced weight gain, and HLA-DQB1 genotype for clozapine-induced agranulocytosis risk. None is in routine clinical use yet.1
Long-term comparative effectiveness data in early-stage populations specifically remain thin. Most of what we know about clozapine’s long-run mortality and rehospitalization advantages comes from chronic populations.
Questions About Clozapine in Early-Stage Schizophrenia
Should clozapine be prescribed earlier than current guidelines suggest?
The evidence in this review supports moving clozapine from third-line to second-line in early-stage schizophrenia — specifically, after the first non-clozapine antipsychotic fails, or after a first relapse on a non-clozapine antipsychotic.
The 34% reduction in next-relapse risk after first relapse, the doubling of response rate over a third non-clozapine trial, and the negative-symptom and functioning advantage when started within 3 years of first episode all point in the same direction.1
How serious is the agranulocytosis risk?
Agranulocytosis — a severe drop in neutrophils (the white blood cells that fight bacterial infection) — remains the headline safety concern. The risk is highest in the first 18 weeks and falls substantially afterward.
With routine absolute neutrophil count (ANC) monitoring, clinically significant agranulocytosis occurs in well under 1% of patients. The FDA’s November 2024 elimination of the REMS program reflected an advisory-committee judgment that mandatory federal monitoring obstructed access without measurably improving safety beyond what good clinical practice already provides.1
What about side effects other than agranulocytosis?
Sedation, hypersalivation, constipation, weight gain, and metabolic effects (changes in BMI and triglycerides in over 50% of patients) are common.1
These are manageable but not trivial. Real-world discontinuation rates run around 35% in early-stage cohorts — a number that needs to be weighed against the alternative of cycling through non-clozapine antipsychotics with progressively lower response rates.
Does clozapine work as well in first-episode patients as in chronic schizophrenia?
The available data suggest yes, with possibly larger benefits in first-episode populations specifically. The Asenjo-Lobos RCT showed similar short-term response to quetiapine in first-episode patients (68% vs. 66%), but the third-line response gap was largest in first-episode psychosis (45% with clozapine vs. 15% without).1
Long-term comparisons in first-episode populations specifically are still sparse.
References
- Clozapine treatment in the early stages of schizophrenia. Davani AJ, Gallego JA & Malhotra AK. Current Opinion in Psychiatry. 2026;39(3):209-215. doi:10.1097/yco.0000000000001059
- Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Kane J, Honigfeld G, Singer J & Meltzer H. Archives of General Psychiatry. 1988;45(9):789-796. doi:10.1001/archpsyc.1988.01800330013001
- Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology. Howes OD et al. American Journal of Psychiatry. 2017;174(3):216-229. doi:10.1176/appi.ajp.2016.16050503
- Real-world effectiveness of antipsychotic treatments in a nationwide cohort of 29,823 patients with schizophrenia. Tiihonen J et al. JAMA Psychiatry. 2017;74(7):686-693. doi:10.1001/jamapsychiatry.2017.1322
- Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Leucht S et al. The Lancet. 2013;382(9896):951-962. doi:10.1016/s0140-6736(13)60733-3
- Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Siskind D, McCartney L, Goldschlager R & Kisely S. British Journal of Psychiatry. 2016;209(5):385-392. doi:10.1192/bjp.bp.115.177261