The most-quoted figure on veteran suicide is “22 a day,” produced from 21-state death-certificate data for 1999–2010.2 The VA’s 2024 Annual Report — with mortality data through 2022 — puts the current daily count at 17.6 Veteran suicides, but the per-Veteran rate has gone the other way.1
Research Highlights
- Daily count was 17.6: 6,407 Veteran suicides occurred in 2022, out of 47,891 suicides among U.S. adults overall.1
- Rate gap remained large: the unadjusted Veteran suicide rate was 34.7 per 100,000 in 2022 vs. 17.1 per 100,000 in non-Veteran U.S. adults.1
- Firearms dominated methods: firearms were involved in 73.5% of Veteran suicide deaths in 2022 vs. 52.2% of non-Veteran adult suicide deaths.1
- VHA users were higher-risk but rose more slowly: Veterans with recent VHA care made up 40.1% of Veteran suicides vs. 33.7% of the Veteran population, but their 2001–2022 rate increases were smaller than among Veterans without recent VHA contact.1
- Post-separation risk peaked at 51.0: the 2019 separation cohort reached 51.0 suicides per 100,000 in the following 12 months, with much higher rates among those with pre-separation suicidal ideation or substance use diagnoses.1
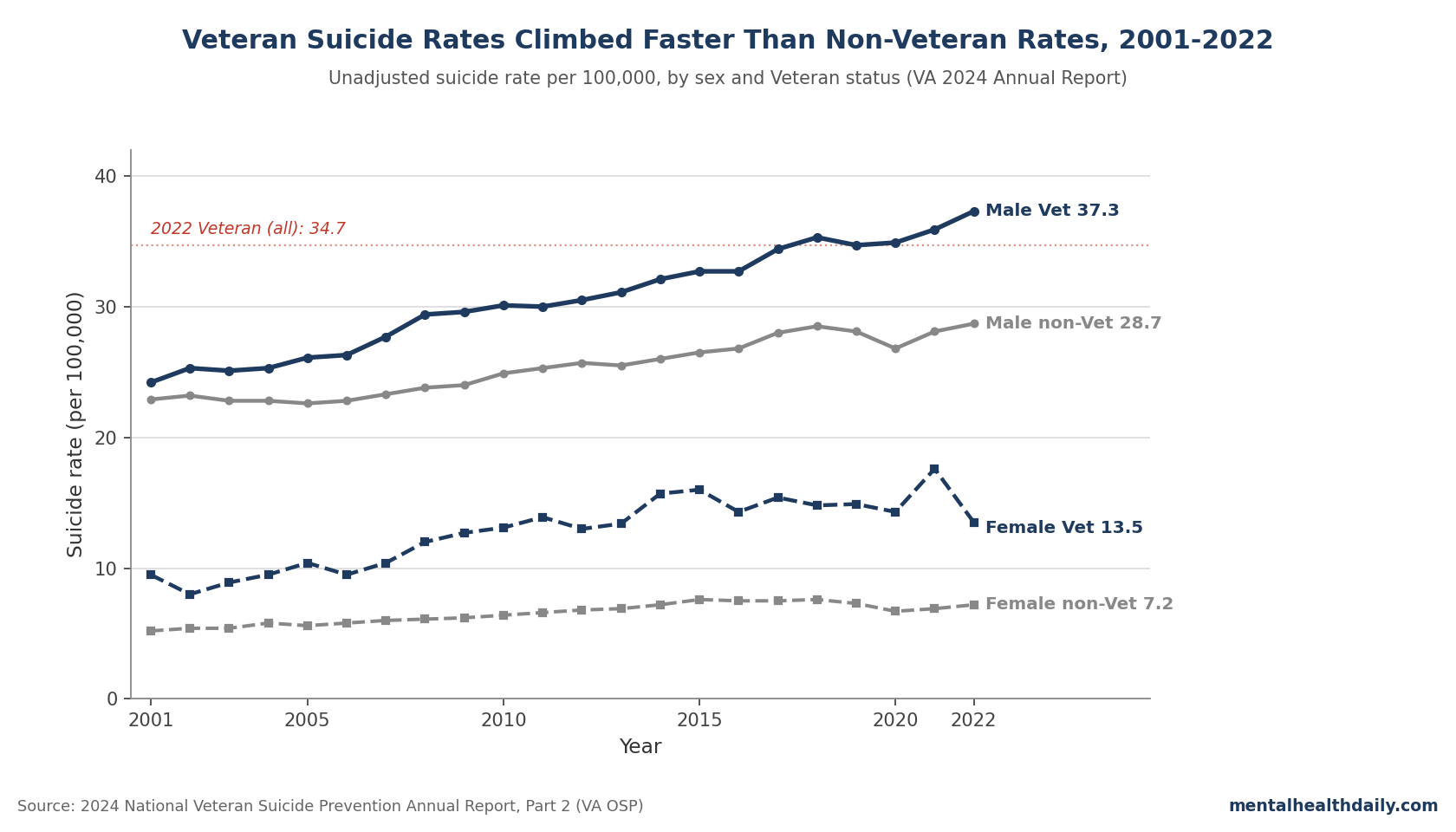
The 2024 report’s headline disaggregates: roughly 7.0 Veteran suicides per day among those who used Veterans Health Administration (VHA) care in 2021 or 2022, and 10.5 per day among other Veterans.1 The unadjusted Veteran rate climbed from 23.3 per 100,000 in 2001 to 34.7 per 100,000 in 2022 — a 49% relative rise — while the non-Veteran adult rate moved from 12.6 to 17.1 per 100,000.1
The per-day count fell partly because the Veteran population shrank 28.4% over the same window. The age-adjusted gap to non-Veteran adults is wider in 2022 than at any prior point in the report’s 22-year series.1
2022 Headline Numbers from the VA’s 2024 Report
Part 2 of the 2024 report covers Veteran mortality through 2022, the most recent year for which linked VA-DoD-CDC mortality data were complete at publication.1 The headline counts:
- 6,407 Veteran suicide deaths in 2022 — three more than in 2021. Of these, 6,136 were among male Veterans (up 83 from 2021) and 271 were among female Veterans (down 80).1
- 47,891 suicides among all U.S. adults in 2022, an average of 131.2 per day.1
- Unadjusted Veteran rate: 34.7 per 100,000 (up from 34.0 in 2021). Female-Veteran rate fell to 13.5 per 100,000 (from 17.6); male-Veteran rate rose to 37.3 per 100,000 (from 35.9).1
- Suicide was the 12th-leading cause of death for Veterans overall and the 2nd-leading cause for Veterans under 45.1
Why the “22 a Day” Figure Has Been Superseded
The “22 a day” statistic comes from the VA’s 2012 Suicide Data Report by Kemp and Bossarte, which used death-certificate data from 21 states for years 1999–2010 to estimate the proportion of U.S. suicides among Veterans, then applied that proportion to the national total.2
Why the old estimate drifted: the state set excluded large Veteran-population states, notably California and Texas, skewed older, and relied on death-certificate Veteran-status flags known to misclassify.3
Subsequent linkage of the VA-DoD Mortality Data Repository with CDC National Death Index records improved classification. By 2022 the figure stabilizes at 17.6 Veteran suicides per day, with a Veteran population that has shrunk 28.4% since 2001 (from 25.8 million to 18.5 million).1
Population shrinkage is why the absolute count can fall while the per-100,000 rate climbs — the rate, not the count, is the relevant burden measure. The per-day number is lower than “22,” but the per-Veteran risk has gone up.
VHA-Using vs. Other Veterans: What Selection Bias Hides
Veterans who use VHA care have higher unadjusted suicide rates than Veterans who do not. In 2022, Recent Veteran VHA Users (those with VHA inpatient or outpatient encounters in 2021 or 2022) accounted for 33.7% of the Veteran population but 40.1% of Veteran suicide deaths.1 A naive read would conclude that VHA care raises suicide risk. The 2024 report’s own framing pushes back.
VHA Users differ systematically from non-users: lower income, poorer health, more chronic medical and mental-health conditions, more trauma exposure, and more current suicidality.4,5 The selection-bias direction runs from elevated risk into VHA care, not the reverse.
The 2001–2022 trends reinforce this read. Over the full window:
- Male Veterans with Recent VHA Use: age-adjusted rate up 19.6%.1
- Male Veterans without Recent VHA Use: age-adjusted rate up 67.6%.1
- Female Veterans with Recent VHA Use: age-adjusted rate up 24.0%.1
- Female Veterans without Recent VHA Use: age-adjusted rate up 55.2%.1
VHA Users started higher and stayed higher in absolute terms, but their rate has risen substantially less than the rate among Veterans the VA does not see. None of this is a controlled comparison — selection into VHA care correlates with too many things to call this a treatment effect — but the differential trajectories are inconsistent with VHA care driving the broader rise.
Firearms Account for Nearly Three-Quarters of Veteran Suicide Deaths
The single most consistent method-specific finding in the report is that firearms dominate Veteran suicide. In 2022, firearms were involved in 73.5% of Veteran suicide deaths (74.8% of male, 45.4% of female) vs. 52.2% of non-Veteran adult suicide deaths (57.4% of male, 34.5% of female).1
Within the overall Veteran rate of 34.7 per 100,000, the firearm-specific component was 25.5 per 100,000, with suffocation contributing 4.5, poisoning 2.8, and other methods 1.8.1
The differential is largest for firearms. In 2022, the firearm suicide rate was 144.4% higher for female Veterans than for female non-Veterans, and 69.6% higher for male Veterans than for male non-Veterans.1 Veterans also report higher firearm ownership: roughly 107% higher among female Veterans and 62% higher among male Veterans, per 2015 National Firearm Survey estimates referenced in the report.1
This tracks the broader means-restriction literature. Mann et al.’ 2005 systematic review identified lethal-means restriction as one of only two interventions with consistent population-level evidence of reducing suicide; physician training in depression recognition was the other.6 Anestis 2017 found state-level firearm legislation tracked changes in firearm-suicide trajectories.7
The VA’s Behavioral Health Autopsy Program data flag unsecured firearms in the home in 27.1% of reviewed Veteran suicide cases.1 Voluntary safe-storage and lethal-means counseling are the highest-leverage targetable mechanism the literature has identified for this population.
Risk in the 12 Months After Separation From Active Service
The post-separation window is the single highest-risk period documented in the report. Across separation cohorts 2010–2021, the 12-month suicide rate ranged from 34.8 per 100,000 for the 2010 cohort to 51.0 per 100,000 for the 2019 cohort.1
By branch, the 2021 separation cohort’s 12-month rate ran highest in the Marine Corps (67.9 per 100,000), followed by Navy (46.9), Army (38.8), and Air Force (38.1).1
Pre-separation diagnoses sharpen the gradient enormously. In the same 2021 cohort, the 12-month post-separation suicide rate was:
- 190.9 per 100,000 for those with a Defense Health Agency diagnosis of suicidal ideation in the 12 months before separation.1
- 164.1 per 100,000 for those with a substance use disorder diagnosis.1
- 84.8 per 100,000 for those with any mental health diagnosis.1
Kang and Bullman’s 2015 cohort analysis of 1.3 million OEF/OIF Veterans found risk concentrated in the early post-separation window and among those with prior mental health contact.8 Reger et al.’ 2015 JAMA Psychiatry analysis of 3.9 million service members found that deployment itself was not associated with elevated suicide risk (HR 0.96, 99% CI 0.87–1.05), but separation from service was — particularly early separation and separation under less-than-honorable conditions.9
Screening implication: the highest-leverage screening window is the moment of separation, and the pre-separation DHA health record is the highest-yield input.
Subgroups With the Highest Documented Risk in 2022
Within VHA-care subgroups, the strongest signals:
- Active Behavioral Patient Record clinical flag: 166.1 per 100,000 in 2021–2022 vs. 40.3 per 100,000 for Veterans without an active or recent flag.1
- Veterans Crisis Line contact: in the 30 days after a documented 2021 VCL call, chat, or text, the suicide rate was 734.0 per 100,000, falling to 303.3 over the subsequent 12 months.1
- Justice, homelessness, and military sexual trauma flags: Veterans Justice Program contact, homelessness diagnoses, and positive military sexual trauma screens each marked substantially elevated 2022 rates.1
- Priority Group 5: this income-based eligibility group had the highest rate every year from 2005–2022, reaching 56.7 per 100,000 in 2022.1
These are descriptive risk-stratification signals, not experimental causal estimates. They still justify concentrating resources around Veterans who carry these flags, especially near crisis-line or justice-system contact.
Limitations of the 2024 Report
Three caveats deserve weight:
- The Veteran-vs.-non-Veteran age adjustment is fragile. Morral, Schell, and Smart 2023 showed age- and sex-adjustment changes the headline differentials substantially; the 92.4% female differential is best read as the upper end of plausible estimates.10
- Veteran-status classification has improved over time. The VA-DoD Mortality Data Repository improves on death-certificate-only methods by linking to service records, but coverage was lower in early years (2001–2010) than in later years (2015–2022). Apparent trend slope is partly identification slope.3
- The VHA-vs.-non-VHA comparison cannot identify a treatment effect. Selection bias runs from elevated risk into care. Even the differential trends (slower rise among VHA Users) cannot be cleanly attributed to VHA services without a counterfactual; eligibility expansions and changes in who enrolls confound. The honest read is descriptive, not causal.
Questions Veterans and Their Families Ask
Is the “22 a day” figure still accurate?
No. The current best estimate, from the 2024 VA report covering data through 2022, is 17.6 Veteran suicides per day. The “22” figure came from a 2012 analysis of 21 states’ death certificates and has since been superseded by linked VA-DoD-CDC mortality data. The per-day count has fallen partly because the Veteran population has shrunk 28.4% since 2001; the per-100,000 rate has risen.1,2
Is suicide higher among Veterans than the general population?
Yes, on every adjustment the 2024 report uses. The unadjusted rate is roughly 2× the non-Veteran adult rate (34.7 vs. 17.1 per 100,000). Age-adjusted, the female-Veteran rate runs 92.4% higher and the male-Veteran rate 44.3% higher than the corresponding non-Veteran rate. Differentials are largest in the 18- to 34-year-old age band.1
Why is the suicide rate higher in Veterans who use VHA care?
Selection bias. Veterans who enroll concentrate suicide risk factors — lower income, more chronic illness, more mental health diagnoses, more reported trauma, more current suicidality — relative to those who don’t. The slower long-run rise in VHA-Veteran rates is consistent with VHA care doing useful work, but the comparison cannot identify a treatment effect cleanly.1,4,5
What role do firearms play?
Firearms were involved in 73.5% of Veteran suicide deaths in 2022 vs. 52.2% in non-Veteran adults. The firearm-suicide rate is the dominant component of the overall Veteran rate (25.5 of 34.7 per 100,000). Higher firearm ownership accounts for most of the Veteran-vs.-non-Veteran differential.1,6,7
When is risk highest after leaving the military?
The 12 months following separation. Across cohorts 2010–2021, the 12-month post-separation rate ranged from 34.8 to 51.0 per 100,000, concentrating in those with pre-separation DHA diagnoses of suicidal ideation, substance use disorder, or other mental health conditions — up to 190.9 per 100,000.1,8
Did combat deployment raise suicide risk?
Reger et al.’ 2015 cohort analysis of 3.9 million service members found no association between deployment per se and suicide (HR 0.96, 99% CI 0.87–1.05). Separation from service did predict elevated risk, particularly early separation and less-than-honorable discharge.9
How can a Veteran in crisis get help right now?
In the United States, the 988 Suicide and Crisis Lifeline is reachable 24/7 by calling or texting 988. Veterans, service members, and their families can press 1 after dialing 988 to reach the Veterans Crisis Line, also available by text to 838255 or chat at VeteransCrisisLine.net.
References
- 2024 National Veteran Suicide Prevention Annual Report, Part 2 of 2: Report Findings. Office of Suicide Prevention, U.S. Department of Veterans Affairs. December 2024. mentalhealth.va.gov (PDF)
- Suicide Data Report, 2012. Kemp J, Bossarte R. Department of Veterans Affairs Mental Health Services, Suicide Prevention Program. 2013. va.gov (PDF)
- Reevaluating suicide mortality for Veterans with data from the VA-DoD Mortality Data Repository, 2000–2010. Hoffmire CA, Stephens B, Morley S, et al. Psychiatric Services. 2020;71(8):793–800. doi:10.1176/appi.ps.201900324
- Comparing mental and physical health of U.S. Veterans by VA healthcare use: implications for generalizability of research in the VA electronic health records. Fink DS, Stohl M, Mannes ZL, et al. BMC Health Services Research. 2022;22:1500. doi:10.1186/s12913-022-08899-y
- U.S. Veterans who do and do not utilize VA health care services: demographic, military, medical, and psychosocial characteristics. Meffert BN, Morabito DM, Sawicki DA, et al. Primary Care Companion CNS Disorders. 2019;21(1):18m02350. doi:10.4088/pcc.18m02350
- Suicide prevention strategies: a systematic review. Mann JJ, Apter A, Bertolote J, et al. JAMA. 2005;294(16):2064–2074. doi:10.1001/jama.294.16.2064
- Rising longitudinal trajectories in suicide rates: the role of firearm suicide rates and firearm legislation. Anestis MD, Selby EA, Butterworth SE. Preventive Medicine. 2017;100:159–166. doi:10.1016/j.ypmed.2017.04.032
- Suicide risk among 1.3 million Veterans who were on active duty during the Iraq and Afghanistan wars. Kang HK, Bullman TA, Smolenski DJ, Skopp NA, Gahm GA, Reger MA. Annals of Epidemiology. 2015;25(2):96–100. doi:10.1016/j.annepidem.2014.11.020
- Risk of suicide among US military service members following Operation Enduring Freedom or Operation Iraqi Freedom deployment and separation from the US military. Reger MA, Smolenski DJ, Skopp NA, et al. JAMA Psychiatry. 2015;72(6):561–569. doi:10.1001/jamapsychiatry.2014.3195
- Comparison of suicide rates among US Veteran and nonveteran populations. Morral AR, Schell TL, Smart R. JAMA Network Open. 2023;6(7):e2324191. doi:10.1001/jamanetworkopen.2023.24191